Download presentation
Presentation is loading. Please wait.

1
MISCELLANEOUS ISSUES IN PPCI CULPRIT VESSEL ONLY VS MULTIVESSEL PCI DURING PPCI ADJUNCTIVE THROMBECTOMY/EMBOLIC PROTECTION/ASPIRATION DES vs BMS

2
40-65% of the patients presenting with STEMI have multivessel disease (MVD), which has been associated with worse clinical outcome as compared with single-vessel disease Multivessel intervention ?
, which has been associated with worse clinical outcome as compared with single-vessel disease Multivessel intervention")
3
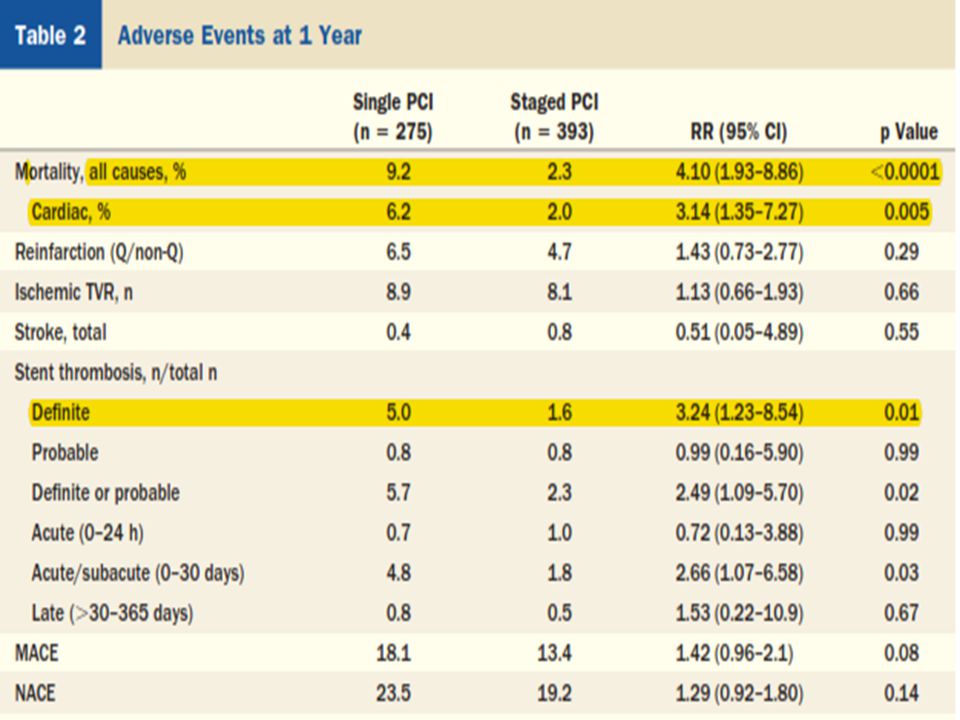
Prognostic Impact of Staged Versus “One-Time” Multivessel PCI in AMI.. Analysis From the HORIZONS- AMI Trial [JACC aug 2011] Aim … to compare a one-time PPCI of the culprit and nonculprit lesions vs PCI of only the culprit lesion and staged nonculprit PCI at a later date HORIZONS-AMI trial … prosp open label multicentre trial.. 668 of the 3,602 STEMI patients enrolled (18.5%) underwent PCI of culprit and nonculprit lesions for multivessel disease. Patients were categorized into a single PCI strategy (n=275) vs staged PCI (n=393). The endpoints analyzed are the 1-year rates of MACEs and its components, death,reinfarction, TVR for ischemia and stroke.
 underwent PCI of culprit and nonculprit lesions for multivessel disease. Patients were categorized into a single PCI strategy (n=275) vs staged PCI (n=393). The endpoints analyzed are the 1-year rates of MACEs and its components, death,reinfarction, TVR for ischemia and stroke..")
7
Single versus staged PCI was a/w higher 1-year mortality (9.2% vs. 2.3%; p<0.0001) higher cardiac mortality (6.2% vs. 2.0%;P=0.005) higher definite/probable ST (5.7% vs. 2.3%; p=0.02) trend toward greater MACE (18.1% vs. 13.4%; p=0.08). In patients undergoing truly elective multivessel PCI also, mortality advantage was maintained.
 higher cardiac mortality (6.2% vs. 2.0%;P=0.005) higher definite/probable ST (5.7% vs. 2.3%; p=0.02) trend toward greater MACE (18.1% vs. 13.4%; p=0.08). In patients undergoing truly elective multivessel PCI also, mortality advantage was maintained..")
8
Culprit Vessel PCI Versus Multivessel and Staged PCI for STEMI Patients With MVD.. Hannan et al … jacc 2010 STEMI with MVD….2003-2006 subdivided into culprit vessel PCI and those who underwent multivessel PCI during the index procedure, during the index admission or staged within 60 days of the index admission. Of the 4,024 pts in the study, 3,521 (87.5%) underwent only culprit vessel revascularization at the time of primary PCI and the remainder underwent multivessel revascularization at the time of primary PCI.
 underwent only culprit vessel revascularization at the time of primary PCI and the remainder underwent multivessel revascularization at the time of primary PCI..")
9
259 pts underwent staged PCI during the index admission and 538 pts underwent staged PCI within 60 days of the index procedure. For patients without hemodynamic compromise, culprit vessel PCI during the index procedure was associated with lower in-hospital mortality than multivessel PCI during the index procedure (0.9% vs. 2.4%, p=0.04). Patients undergoing staged multivessel PCI within 60 days after the index procedure had a significantly lower 12-month mortality rate than patients undergoing culprit vessel PCI only (1.3% vs. 3.3%, p= 0.04).
. Patients undergoing staged multivessel PCI within 60 days after the index procedure had a significantly lower 12-month mortality rate than patients undergoing culprit vessel PCI only (1.3% vs. 3.3%, p= 0.04)..")
10
Culprit Vessel Only Versus Multivessel and Staged PCI for MVD in STEMI ….A Pairwise and Network Meta-Analysis Vlaar et al. JACC Aug 2011 4 prospective and 14 retrospective studies involving 40,280 pts [STEMI pts with MVD who underwent PCI] Pairwise and network meta-analyses were performed on 3 PCI strategies 1) culprit PCI 2) multivessel PCI 3) staged PCI. The primary endpoint was short-term[1month] mortality Secondary endpoints were long term mortality, reinfarction, any revascularization, major bleeding and stroke
 culprit PCI 2) multivessel PCI 3) staged PCI. The primary endpoint was short-term[1month] mortality Secondary endpoints were long term mortality, reinfarction, any revascularization, major bleeding and stroke.")
12
Five studies compared all 3 PCI strategies;10 studies compared culprit PCI versus MV-PCI ; 2 studies compared culprit PCI versus staged PCI, and 1 study compared MV-PCI versus staged PCI Timing of staged procedures….majority …. during hospitalization or within 1 month after index PCI The staged PCI strategy was superior in comparison with culprit PCI (odds ratio [OR]: 3.03, 95% CI: 1.41 to 6.51, p=0.005) and MV-PCI (OR: 5.31, 95% CI: 2.31 to 12.21, p= 0.0001). Mortality was lower in the culprit PCI strategy as compared with MV-PCI (OR: 0.66, 95% CI: 0.48 to 0.89, p 0.007).
 and MV-PCI (OR: 5.31, 95% CI: 2.31 to 12.21, p= ). Mortality was lower in the culprit PCI strategy as compared with MV-PCI (OR: 0.66, 95% CI: 0.48 to 0.89, p 0.007)..")
13
Current guidelines indicate that MV-PCI should not be performed in hemodynamic stable STEMI patients. Only for patients in cardiogenic shock, PCI may be recommended for all critically stenosed large epicardial coronary arteries. However, no randomized data have been published indicating that MV-PCI is beneficial for cardiogenic shock patients. A deferred angioplasty strategy of nonculprit lesions should remain the standard approach in patients with STEMI undergoing primary PCI

14
MISCELLANEOUS ISSUES IN 1 0 PCI Culprit vessel only vs multivessel PCI during PPCI ADJUNCTIVE THROMBECTOMY/EMBOLIC PROTECTION/ASPIRATION DES vs BMS

16
Thrombus Aspiration during Primary PCI in Acute MI Study [TAPAS] … nejm 2008 single-center, prospective, randomized trial Inclusion criteria symptoms s/o a/c myocardial ischemia > 30 mts onset of symptoms < 12 hours STE> 0.1 mV in ≥ 2 leads Exclusion criteria Rescue PCI Disease- life expectancy <6 months
![Thrombus Aspiration during Primary PCI in Acute MI Study [TAPAS] … nejm 2008 single-center, prospective, randomized trial Inclusion criteria symptoms s/o a/c myocardial ischemia > 30 mts onset of symptoms < 12 hours STE> 0.1 mV in ≥ 2 leads Exclusion criteria Rescue PCI Disease- life expectancy <6 months](http://images.slideplayer.com/13/4143369/slides/slide_16.jpg "Thrombus Aspiration during Primary PCI in Acute MI Study [TAPAS] … nejm 2008 single-center, prospective, randomized trial Inclusion criteria symptoms s/o a/c myocardial ischemia > 30 mts onset of symptoms < 12 hours STE> 0.1 mV in ≥ 2 leads Exclusion criteria Rescue PCI Disease- life expectancy <6 months")
17
Before CAG,1071 pts randomised to thrombus aspirn grp(535), conventional pci grp(536).. 1 0 end point : postprocedural myocardial blush grade of 0 or 1 2 0 end points : postprocedural frequencies of TIMI flow grade of 3, complete STR, the absence of persistent ST-segment deviation, TVR, reinfarction, death and the combination of MACE by 30 days after randomization.

18
On the basis of the initial angiographic findings, 33 patients (approximately 6%) in each group did not undergo PCI. In the thrombus-aspiration group, aspiration and direct stent implantation were performed in 295 patients (55.1%), balloon dilation was performed before stent implantation in 153 patients (28.6%) and conventional PCI was performed in 54 patients (10.1%) in whom the operator judged the target artery to be too small or too tortuous to permit use of the aspiration catheter
, balloon dilation was performed before stent implantation in 153 patients (28.6%) and conventional PCI was performed in 54 patients (10.1%) in whom the operator judged the target artery to be too small or too tortuous to permit use of the aspiration catheter.")
20
Aspiration before stenting results in improved myocardial reperfusion -documented by imprvt in the MBG -increased STR -reduced residual ST-seg deviation benefit - consistently present in all patients….. irrespective of baseline clinical or angio characteristics ( age, sex, IRA, preprocedural TIMI flow or visible thrombus )
.")
21
The EXPIRA (Thrombectomy With Export Catheter in IRA during 1 0 pci) Prospective, Randomized Trial To evaluate the impact of a manual intracoronary aspiration thrombectomy device, Export Medtronic as adjunctive therapy [EM-PCI] on procedural outcomes, MBG and 90-min STR 70% and on microvascular obstruction(MVO) and Infarct Size assessed by CE- MRI in patients with anterior STEMI.
![The EXPIRA (Thrombectomy With Export Catheter in IRA during 1 0 pci) Prospective, Randomized Trial To evaluate the impact of a manual intracoronary aspiration thrombectomy device, Export Medtronic as adjunctive therapy [EM-PCI] on procedural outcomes, MBG and 90-min STR 70% and on microvascular obstruction(MVO) and Infarct Size assessed by CE- MRI in patients with anterior STEMI.](http://images.slideplayer.com/13/4143369/slides/slide_21.jpg "The EXPIRA (Thrombectomy With Export Catheter in IRA during 1 0 pci) Prospective, Randomized Trial To evaluate the impact of a manual intracoronary aspiration thrombectomy device, Export Medtronic as adjunctive therapy [EM-PCI] on procedural outcomes, MBG and 90-min STR 70% and on microvascular obstruction(MVO) and Infarct Size assessed by CE- MRI in patients with anterior STEMI.")
23
Inclusion criteria first STEMI within 9 h from symptoms onset, IRA> 2.5 mm in diameter, thrombus score > 3, TIMI grade 18 years. Primary end points were the occurrence of myocardial blush grade>2 and the rate of 90-min STr >70%. RESULTS : Primary end points occurred more frequently in EM- PCI (MBG>2: 88% vs 59%, p<0.0001; STr: 63% vs 39%, p=0.001) At 9 months, no differences were observed in terms of cumulative MACE…..S-PCI had a higher incidence of cardiac death (p=0.02) than did EM-PCI
 At 9 months, no differences were observed in terms of cumulative MACE…..S-PCI had a higher incidence of cardiac death (p=0.02) than did EM-PCI.")
24
CE-MRI results: No differences in the baseline EF, volumes and IS were observed between the 2 groups. Postprocedural rate of MBG >2 and STr >70% was higher in the EM-PCI group (89% vs. 59% and 84% vs. 40% respectively; p 0.0001). In the acute phase, greater incidence and extent of MVO was observed in the S-PCI group vs the EM- PCI group (72.9% vs. 31.5%, p=0.0005; and 3.7+2.6 g vs. 1.7 +1.9 g, p= 0.0003 respectively); no differences were observed in IS. At 3 months, a reduction in final IS was detected in the EM-PCI group (IS mass from 17+15g to11+ 8.7 g, p=0.004; IS% from 14+12% to 9+4.5 %, p=0.001), whereas no changes were observed in the S-PCI group. MVO was not observed in either group at follow-up.
. In the acute phase, greater incidence and extent of MVO was observed in the S-PCI group vs the EM- PCI group (72.9% vs. 31.5%, p=0.0005; and g vs g, p= respectively); no differences were observed in IS. At 3 months, a reduction in final IS was detected in the EM-PCI group (IS mass from 17+15g to g, p=0.004; IS% from 14+12% to %, p=0.001), whereas no changes were observed in the S-PCI group. MVO was not observed in either group at follow-up..")
26
Relation between Final Myocardial Blush Grade and Cardiac Death and MACE at 2-years follow-up. Cardiac death (%) 0 1.8 11.1 38 0.001 MACE (%) 4.3 9.1 22.2 37.5 0.003
 MACE (%)")
27
Relation between % STR and Cardiac Death / MACE at 2-years follow-up Cardiac death (%) 0.9 7.3 0.023 MACE (%) 3.7 17.6 0.002
 MACE (%)")
28
Pretreatment with manual thrombectomy - results in a lower cardiac mortality and a lower incidence of other MACEs at 2-year Occurrence of cardiac death and MACE is significantly related to final MBG and ST-segment resolution

30
The Angiojet thrombectomy system, used in the AIMI trial, is a 4F catheter connected with a driving unit, which generates high-velocity saline jets at the distal end of the catheter. The resulting vortex fragments and aspirates thrombus material in a collecting lumen

31
X AMINE ST trial Prosp randomised multicentric study X sizer thrombectomy + PCI [100pts] vs conventional PCI[101 pts] in AMI <12 hrs & initial TIMI flow grade 0 to 1 The magnitude of STR 1 h after PCI was the primary end point. Magnitude of STR was greater in the X-Sizer group (7.5 vs 4.9 mm p=0.033) as is STR>50% (68% vs 53%; p=0.037);distal embolization was reduced (2% vs 10%; p=0.033);TIMI flow grade3 was obtained in 96% vs 89% (p=0.105). Myocardial blush grade 3 was similar (30% vs. 31%; p=NS). Six-month clinical outcome was comparable (death 6% vs 4% and MACCE 13% vs 13%)
![X AMINE ST trial Prosp randomised multicentric study X sizer thrombectomy + PCI [100pts] vs conventional PCI[101 pts] in AMI <12 hrs & initial TIMI flow grade 0 to 1 The magnitude of STR 1 h after PCI was the primary end point.](http://images.slideplayer.com/13/4143369/slides/slide_31.jpg "Magnitude of STR was greater in the X-Sizer group (7.5 vs 4.9 mm p=0.033) as is STR>50% (68% vs 53%; p=0.037);distal embolization was reduced (2% vs 10%; p=0.033);TIMI flow grade3 was obtained in 96% vs 89% (p=0.105). Myocardial blush grade 3 was similar (30% vs. 31%; p=NS). Six-month clinical outcome was comparable (death 6% vs 4% and MACCE 13% vs 13%).")
32
So intracoronary thrombectomy with the X-Sizer catheter during catheter-based treatment of AMI improved myocardial reperfusion in patients presenting with TIMI flow grade 0 to 1, as assessed by a lower rate of distal embolization and a higher rate of STR.

33
EMERALD: Enhanced Myocardial Efficacy and Removal by Aspiration of Liberated Debris … jacc 2004 To assess the safety and efficacy of GuardWire distal protection device in AMI pts undergoing PPCI or rescue PCI. Inclusion Criteria Patients with acute MI > 30 minutes and ≤ 6 hours in duration > 2 mm of ST-segment elevation MI in ≥ 2 contiguous leads or left bundle branch block Absence of cardiogenic shock Reference vessel diameter 2.5-5.0 mm ≥ 3 cm of distal vessel available Exclusion Criteria Multivessel intervention acutely required Multivessel disease requiring surgery within 30 days Upfront use of atherothrombectomy catheters

34
GuardWire temporary occlusion–aspiration system, used in the EMERALD trial……0.014 in. guidewire with a distal elastomeric occlusive balloon. Balloon inflation is obtained through the EZ Flator. After intervention, performed in the absence of antegrade flow, liberated debris is aspirated through the 5F monorail export catheter.

35
Primary end points Complete (≥ 70%) STR 30 mts after the last angio Infarct size as assessed by technetium-99m sestamibi scintigraphy imaging at 5-14 days Secondary Endpoints Myocardial blush score MACE defined as the combined endpoint of death, new-onset severe HF, new-onset severe hypotension, or readmission for LVF at 30-day follow-up.
 STR 30 mts after the last angio Infarct size as assessed by technetium-99m sestamibi scintigraphy imaging at 5-14 days Secondary Endpoints Myocardial blush score MACE defined as the combined endpoint of death, new-onset severe HF, new-onset severe hypotension, or readmission for LVF at 30-day follow-up.")
36
501 patients.. randomized to either PCI using GuardWire (n = 252) or standard PCI (n=249)
 or standard PCI (n=249)")
39
Thus EMERALD trial failed to show a beneficial effect from the use of distal embolic protection devices in acute MI patients.

41
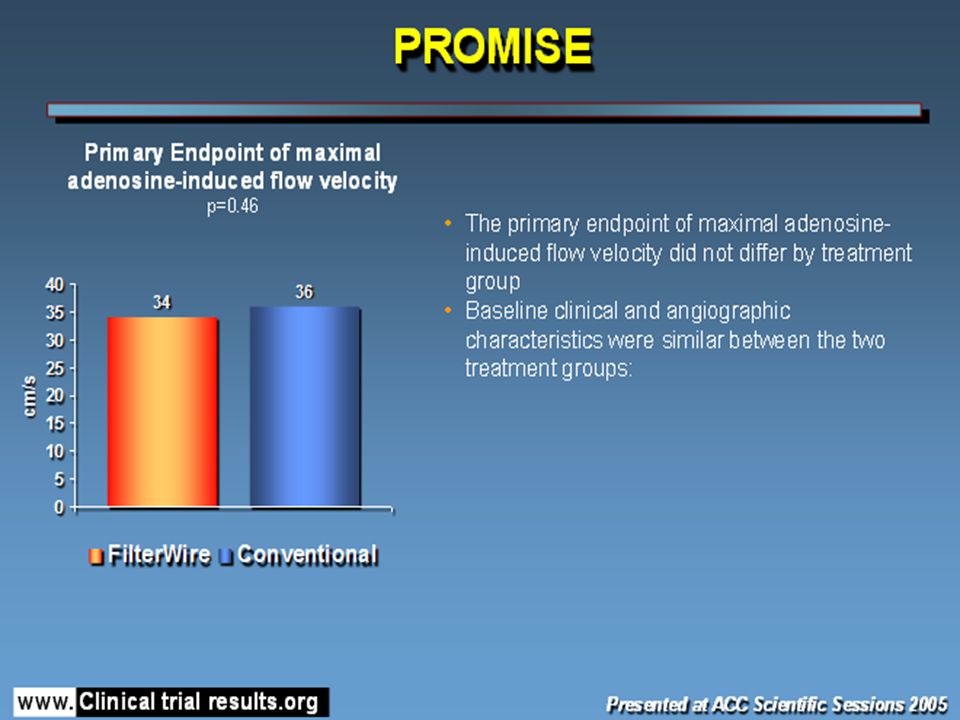
The FilterWire system : non-occlusive, filter-based distal protection device[polyurethane porous membrane filter] (pore size 110 mm) attached to a nitinol loop at the distal end of a 0.014 in. guidewire
![The FilterWire system : non-occlusive, filter-based distal protection device[polyurethane porous membrane filter] (pore size 110 mm) attached to a nitinol loop at the distal end of a in.](http://images.slideplayer.com/13/4143369/slides/slide_41.jpg "guidewire.")
44
Randomized Comparison of Distal Protection Versus Conventional Treatment in PPCI [DEDICATION trial] 626 patients with STEMI referred within 12 h Random. to PCI performed with (n=312) or without (n=314) distal protection. 1 0 end point was complete (>70%) STR. Blood levels of trop-T and CK-MB were monitored before and after the procedure, and LV wall motion index (WMI) was performed before discharge.
![Randomized Comparison of Distal Protection Versus Conventional Treatment in PPCI [DEDICATION trial] 626 patients with STEMI referred within 12 h Random.](http://images.slideplayer.com/13/4143369/slides/slide_44.jpg "to PCI performed with (n=312) or without (n=314) distal protection. 1 0 end point was complete (>70%) STR. Blood levels of trop-T and CK-MB were monitored before and after the procedure, and LV wall motion index (WMI) was performed before discharge..")
45
No significant difference in the occurrence of the primary end point (76% vs. 72%, p=0.29), no difference in maximum trop T (4.8 µg/l and 5.0 µg/l, p=0.87) or maximum creatine kinase-MB (185 µg/l and 184 µg/l,P=0.99), and no difference in median WMI (1.70 vs. 1.70, p=0.35). The rate of MACCE 1 month after PCI was 5.4% with distal protection and 3.2% with conventional Rx (p 0.17). The routine use of distal protection by a filterwire system during primary PCI does not seem to improve microvascular perfusion, limit infarct size, or reduce the occurrence of MACCE
, no difference in maximum trop T (4.8 µg/l and 5.0 µg/l, p=0.87) or maximum creatine kinase-MB (185 µg/l and 184 µg/l,P=0.99), and no difference in median WMI (1.70 vs. 1.70, p=0.35). The rate of MACCE 1 month after PCI was 5.4% with distal protection and 3.2% with conventional Rx (p 0.17). The routine use of distal protection by a filterwire system during primary PCI does not seem to improve microvascular perfusion, limit infarct size, or reduce the occurrence of MACCE.")
46
2011 guidelines … Aspiration thrombectomy is reasonable for patients undergoing primary PCI [IIa]
![2011 guidelines … Aspiration thrombectomy is reasonable for patients undergoing primary PCI [IIa]](http://images.slideplayer.com/13/4143369/slides/slide_46.jpg "2011 guidelines … Aspiration thrombectomy is reasonable for patients undergoing primary PCI [IIa]")
47
JetStent Trial

48
INFUSE-AMI Trial

49
Systemic inhibition of GPIIb/IIIa receptors with intravenous abciximab

51
MISCELLANEOUS ISSUES IN 1 0 PCI CULPRIT VESSEL ONLY VS MULTIVESSEL PCI DURING PPCI ADJUNCTIVE THROMBECTOMY/EMBOLIC PROTECTION/ASPIRATION DES VS BMS

52
DES in AMI (RCTs)
")
54
TYPHOON Trial Single-blind, multicentered, prospective...2003-2005 Exclusion criteria : administration of fibrinolytics for the index infarction, overt AHF, a previously documented LVEF of <30%, previous MI and an estimated life expectancy of <12 months. Primary endpoint – TVF(target vessel failure) at 12 mo Angiographic follow-up on 174 pts at 8 mo [Criteria for angiographic exclusion …. previous PCI of the IRA, excessive tortuosity or calcification, ostial or multiple lesions, massive thrombus in the IRA, bifurcation or LMCA disease and severe multivessel disease requiring surgical revascularization] Target lesion with maximum length of 30 mm and located in a native coronary artery with a reference-vessel diameter of 2.25-3.50 mm.
 at 12 mo Angiographic follow-up on 174 pts at 8 mo [Criteria for angiographic exclusion …. previous PCI of the IRA, excessive tortuosity or calcification, ostial or multiple lesions, massive thrombus in the IRA, bifurcation or LMCA disease and severe multivessel disease requiring surgical revascularization] Target lesion with maximum length of 30 mm and located in a native coronary artery with a reference-vessel diameter of mm..")
55
Typhoon … results @ 12 months

56
TYPHOON … Use of SES provided significant reduction in TVR at 12 mo 4 year F/U of TYPHOON [jacc interv 2011 Jan] Freedom from TLR at 4 years was signif better in the SES group (92.4% vs. 85.1%; p = 0.002) No signif diff in 1. freedom from cardiac death (97.6% and 95.9%; p = 0.37) 2. freedom from repeat myocardial infarction (94.8% and 95.6%; p = 0.85) 3. definite/probable stent thrombosis (SES: 4.4%, BMS: 4.8%, p = 0.83) At 4 yrs, the all-cause death rate was 5.8% in the SES and 7.0% in the BMS group (p = 0.61).
![TYPHOON … Use of SES provided significant reduction in TVR at 12 mo 4 year F/U of TYPHOON [jacc interv 2011 Jan] Freedom from TLR at 4 years was signif better in the SES group (92.4% vs.](http://images.slideplayer.com/13/4143369/slides/slide_56.jpg "85.1%; p = 0.002) No signif diff in 1. freedom from cardiac death (97.6% and 95.9%; p = 0.37) 2. freedom from repeat myocardial infarction (94.8% and 95.6%; p = 0.85) 3. definite/probable stent thrombosis (SES: 4.4%, BMS: 4.8%, p = 0.83) At 4 yrs, the all-cause death rate was 5.8% in the SES and 7.0% in the BMS group (p = 0.61)..")
57
PASSION prospective, single-blind, RCT… Netherlands primary end point … the first occurrence of MACE 2 0 end point …. occurrence of ST. Failed to show a significant benefit with the use of PES vs BMS Lack of angiographic follow-up may have contributed to the findings No difference in ST between the groups only 12 mo data

58
PASSION 5 yr F/U … jacc interv 2011 to elucidate a possible long-term benefit of DES over BMS in STEMI in terms of MACE and to address the concern of (very) late ST. At 5-year follow-up….The composite end point of cardiac death, recurrent MI, or TLR was reached in 56 (18.6%) versus 66 (21.8%) patients in the PES and the BMS groups, respectively (HR: 0.82, 95% CI:0.58 to 1.18; p=0.28) Up to 5-years follow-up, no difference in the occurrence of definite or probable ST was seen, although there might be a higher incidence of (very) late ST using PES.
 versus 66 (21.8%) patients in the PES and the BMS groups, respectively (HR: 0.82, 95% CI:0.58 to 1.18; p=0.28) Up to 5-years follow-up, no difference in the occurrence of definite or probable ST was seen, although there might be a higher incidence of (very) late ST using PES..")
59
Passion f/u

60
SESAMI trial : Randomized single center study 320 patients with acute STEMI- 12 month follow up SES vs BMS in 1:1 randomization The infarct-related vessel had to be a native coronary artery with a visually estimated reference diameter >2.5 and < 4.0 mm Primary endpoint – angiographic binary restenosis (ABR) at 12 mo [Binary Restenosis was defined as 50% reduction of the initial lumen diameter in the target lesion inside or at the proximal and distal 5 mm of the stent]
![SESAMI trial : Randomized single center study 320 patients with acute STEMI- 12 month follow up SES vs BMS in 1:1 randomization The infarct-related vessel had to be a native coronary artery with a visually estimated reference diameter >2.5 and < 4.0 mm Primary endpoint – angiographic binary restenosis (ABR) at 12 mo [Binary Restenosis was defined as 50% reduction of the initial lumen diameter in the target lesion inside or at the proximal and distal 5 mm of the stent]](http://images.slideplayer.com/13/4143369/slides/slide_60.jpg "SESAMI trial : Randomized single center study 320 patients with acute STEMI- 12 month follow up SES vs BMS in 1:1 randomization The infarct-related vessel had to be a native coronary artery with a visually estimated reference diameter >2.5 and < 4.0 mm Primary endpoint – angiographic binary restenosis (ABR) at 12 mo [Binary Restenosis was defined as 50% reduction of the initial lumen diameter in the target lesion inside or at the proximal and distal 5 mm of the stent]")
61
SESAMI

62
At 1 Year SES had a lower ABR than did BMS Clinical endpoints (TLR, TVR, TVF and MACE) were significantly better in the SES group 12-month ST rates were similar between groups
 were significantly better in the SES group 12-month ST rates were similar between groups")
63
Typhoon & SESAMI trial showed a large absolute difference in TLR in favor of SES, at 4.3% versus 11.2% (p 0.02) in SES and BMS,respectively. These differences, however, were larger than those observed in PASSION and HORIZONS-AMI.The larger differences in repeat revascularization between the 2 stent groups in both TYPHOON and SESAMI were mainly due to a much higher incidence in the BMS groups. Why this disparity ? could have been influenced by routine angiographic follow-up within the first year after implantation. the stent platform of the DES used in PASSION TRIAL was the exact same stent platform with which it was compared.[cf. TYPHOON and SESAMI, in which a DES was compared with a range of types BMS, possibly resulting in less favorable outcome after the use of BMS.

64
In current clinical practice guidelines, the use of DES in acute STEMI is mentioned only as a method to reduce restenosis. Because there is no evidence for a reduction in the occurrence of death, recurrent MI or ST, the guidelines of the European Society of Cardiology or the American College of Cardiology/American Heart Association do not make a general recommendation for the use of DES in the setting of STEMI.

65
THANK YOU

66
TIMI thrombus grade 0, no cineangiographic characteristics of thrombus are present; in TIMI thrombus grade 1, possible thrombus is present, with such angiography characteristics as reduced contrast density, haziness, irregular lesion contour, or a smooth convex "meniscus" at the site of total occlusion suggestive but not diagnostic of thrombus; in TIMI thrombus grade 2, there is definite thrombus, with greatest dimensions ≤1/2 the vessel diameter; in TIMI thrombus grade 3, there is definite thrombus but with greatest linear dimension >1/2 but <2 vessel diameters; in TIMI thrombus grade 4, there is definite thrombus, with the largest dimension ≥2 vessel diameters; and in TIMI thrombus grade 5, there is total occlusion.

Similar presentations