Download presentation
Presentation is loading. Please wait.

1
PCI VS CABG JOURNAL REVIEW
DR.SANDEEP .R SR CARDIO

2
INTRODUCTION

3
CABG VS MULTIVESSEL PCI
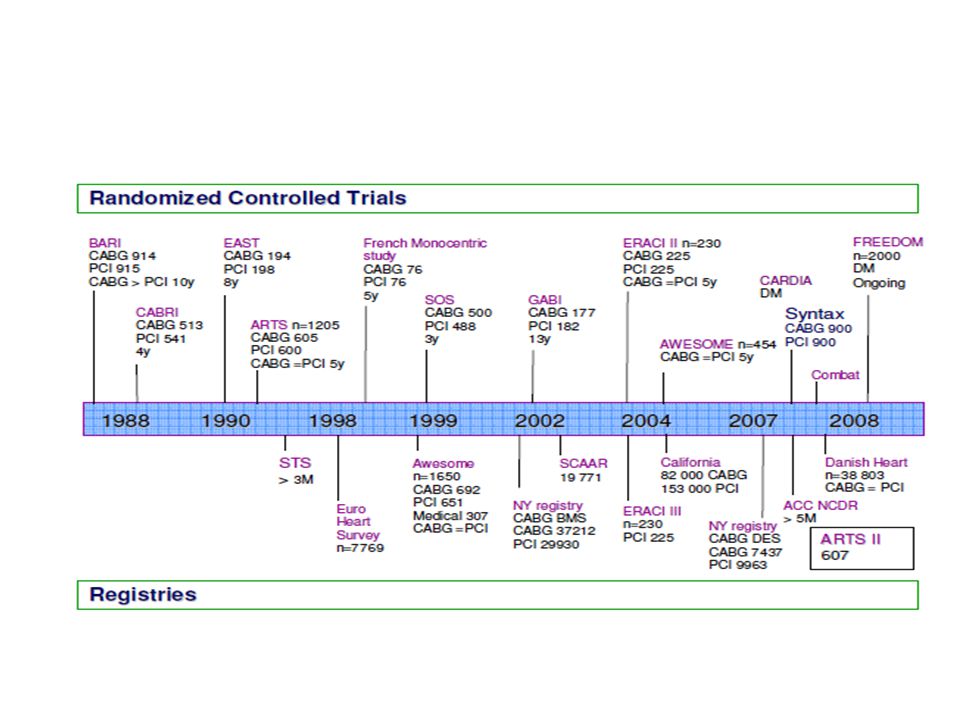
Bypass Angioplasty Revascularization Investigation Trial Multicenter randomized trial comparing CABG & PTCA Eligible pts had symptomatic CAD or severe Ischemia on exercise testing, and angio proven stenosis >50% in > 1 myocardial territory N IN 18 centres betw. AUG1988 – Aug1991 Primary outcomes -- cumulative rates of survival, Q-wave M .I, and survival free of Q-wave M.I in-hospital complications, crossovers & TVR Between August 1988 and August 1991, 1829 patients at 18 clinical centers were randomized to undergo either CABG or PTCA.1 The mean age was 61 years, and one fourth of the cohort were women. More than half of the patients had a history of myocardial infarction, and 9% had a history of treated congestive heart failure. Approximately 20% had diabetes treated with oral agents or insulin; another 5% had untreated diabetes. Two thirds of the patients had unstable angina. Forty-one percent of patients had triplevessel disease; more than one third had at least one totally occluded coronary artery. Overall, the mean percentage of myocardium jeopardized by a lesion of at least 50% was 61%. Twenty-two percent of the patients had an ejection fraction less than 50%. None of these baseline characteristics were significantly different between the treatment groups.

4
RESULTS The rates of in-hospital mortality were similar 1.3% with CABG VS 1.1% with PTCA More patients assigned to CABG had Q-wave myocardial infarctions in the hospital than did patients assigned to PTCA, 4-5% vs 2.1% (P < .01) TVR more in PTCA (6.3% IN PTCA VS 0.1% in CABG group P < .001)
 TVR more in PTCA (6.3% IN PTCA VS 0.1% in CABG group P < .001)")
6
CABRI TRIAL Objective: RCT CABG VS PCI N- 1054
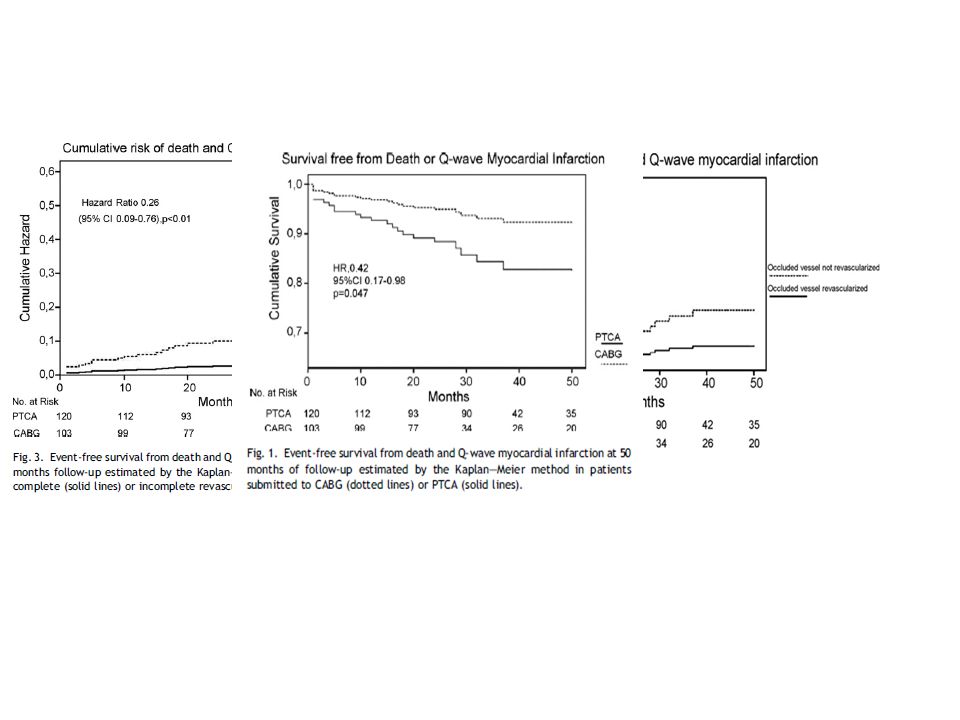
Conclusion: In patients with multivessel coronary disease and chronic occlusion of a major epicardial vessel, achieving of a complete revascularization by reopening or bypassing the occluded vessel is associated with a significantly better long-term prognosis.

8
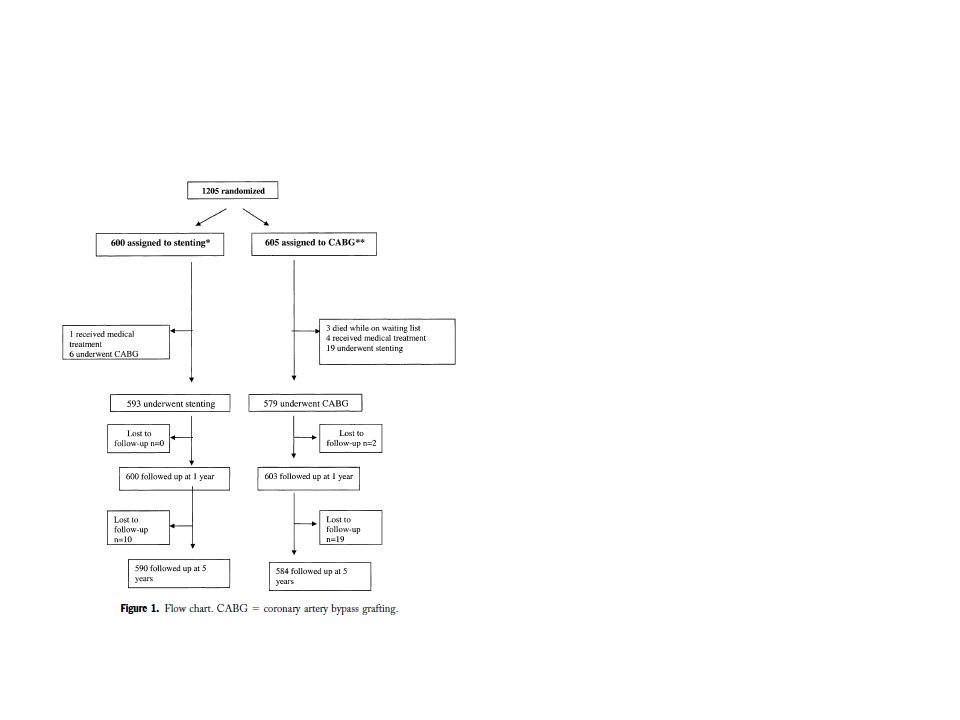
ARTS OBJECTIVES The long-term (five-year) comparative results of treatment of multivessel coronary artery disease with stenting or coronary artery bypass grafting (CABG) is at present unknown. BACKGROUND The Arterial Revascularization Therapies Study (ARTS) was designed to compare CABG and stenting in patients with multivessel disease. METHODS A total of 1,205 patients with the potential for equivalent revascularization were randomly assigned to CABG (n 605) or stent implantation (n 600). The primary clinical end point was freedom from major adverse cardiac and cerebrovascular events (MACCE) at one year; MACCE at five-year follow-up constituted the final secondary end point. RESULTS At five years, there were 48 and 46 deaths in the stent and CABG groups, respectively (8.0% vs. 7.6%; p 0.83; relative risk [RR], 1.05; 95% confidence interval [CI], 0.71 to 1.55). Among 208 diabetic patients, mortality was 13.4% in the stent group and 8.3% in the CABG group (p 0.27; RR, 1.61; 95% CI, 0.71 to 3.63). Overall freedom from death, stroke, or myocardial infarction was not significantly different between groups (18.2% in the stent group vs. 14.9% in the surgical group; p 0.14; RR, 1.22; 95% CI, 0.95 to 1.58). The incidence of repeat revascularization was significantly higher in the stent group (30.3%) than in the CABG group (8.8%; p ; RR, 3.46;95% CI, 2.61 to 4.60). The composite event-free survival rate was 58.3% in the stent group and 78.2% in the CABG group (p ; RR, 1.91;95% CI, 1.60 to 2.28). CONCLUSIONS At five years there was no difference in mortality between stenting and surgery for multivessel disease. Furthermore, the incidence of stroke or myocardial infarction was not significantly different between the two groups. However, overall MACCE was higher in the stent group, driven by the increased need for repeat revascularization.
 is at present unknown. BACKGROUND The Arterial Revascularization Therapies Study (ARTS) was designed to compare CABG. and stenting in patients with multivessel disease. METHODS A total of 1,205 patients with the potential for equivalent revascularization were randomly. assigned to CABG (n 605) or stent implantation (n 600). The primary clinical end point. was freedom from major adverse cardiac and cerebrovascular events (MACCE) at one year; MACCE at five-year follow-up constituted the final secondary end point. RESULTS At five years, there were 48 and 46 deaths in the stent and CABG groups, respectively (8.0% vs. 7.6%; p 0.83; relative risk [RR], 1.05; 95% confidence interval [CI], 0.71 to 1.55). Among 208 diabetic patients, mortality was 13.4% in the stent group and 8.3% in the CABG. group (p 0.27; RR, 1.61; 95% CI, 0.71 to 3.63). Overall freedom from death, stroke, or. myocardial infarction was not significantly different between groups (18.2% in the stent group. vs. 14.9% in the surgical group; p 0.14; RR, 1.22; 95% CI, 0.95 to 1.58). The incidence. of repeat revascularization was significantly higher in the stent group (30.3%) than in the. CABG group (8.8%; p 0.001; RR, 3.46;95% CI, 2.61 to 4.60). The composite event-free. survival rate was 58.3% in the stent group and 78.2% in the CABG group (p ; RR, 1.91;95% CI, 1.60 to 2.28). CONCLUSIONS At five years there was no difference in mortality between stenting and surgery for multivessel. disease. Furthermore, the incidence of stroke or myocardial infarction was not significantly. different between the two groups. However, overall MACCE was higher in the stent group, driven by the increased need for repeat revascularization.")
12
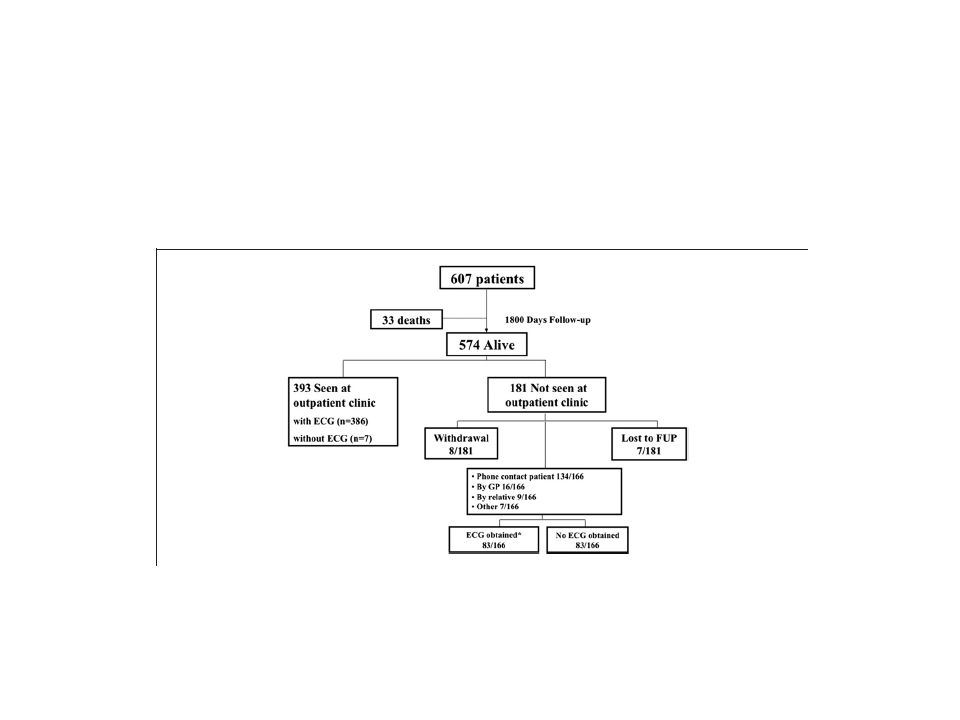
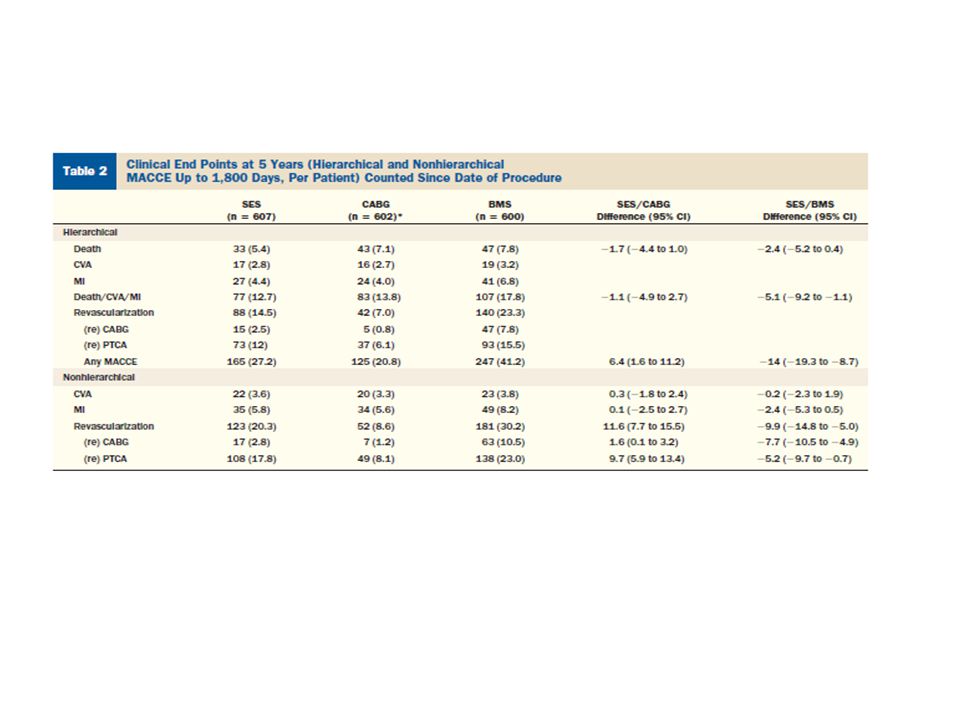
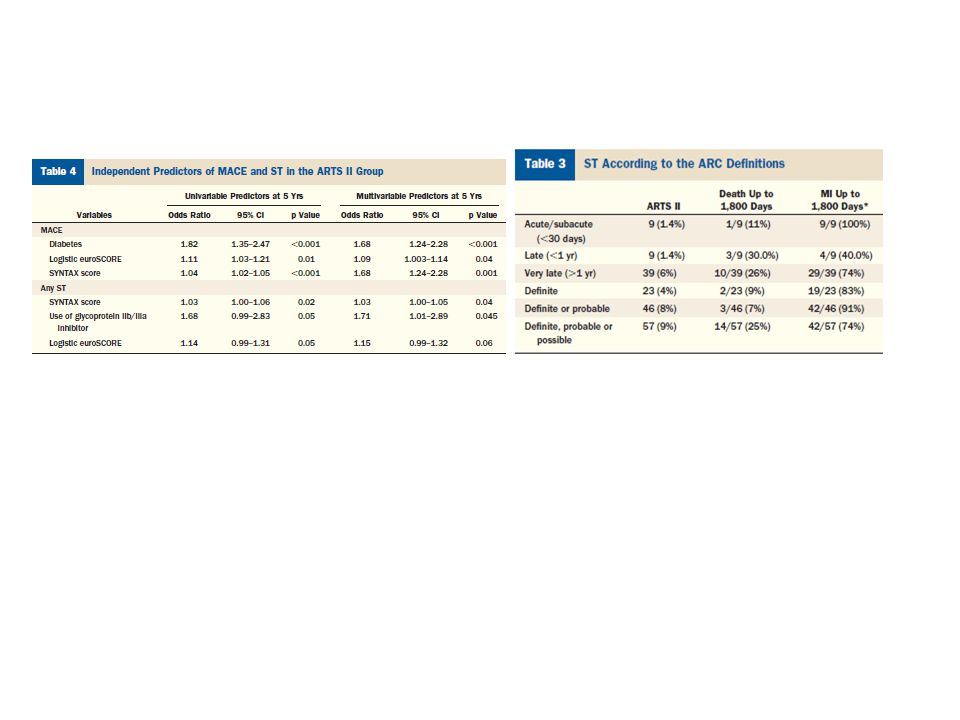
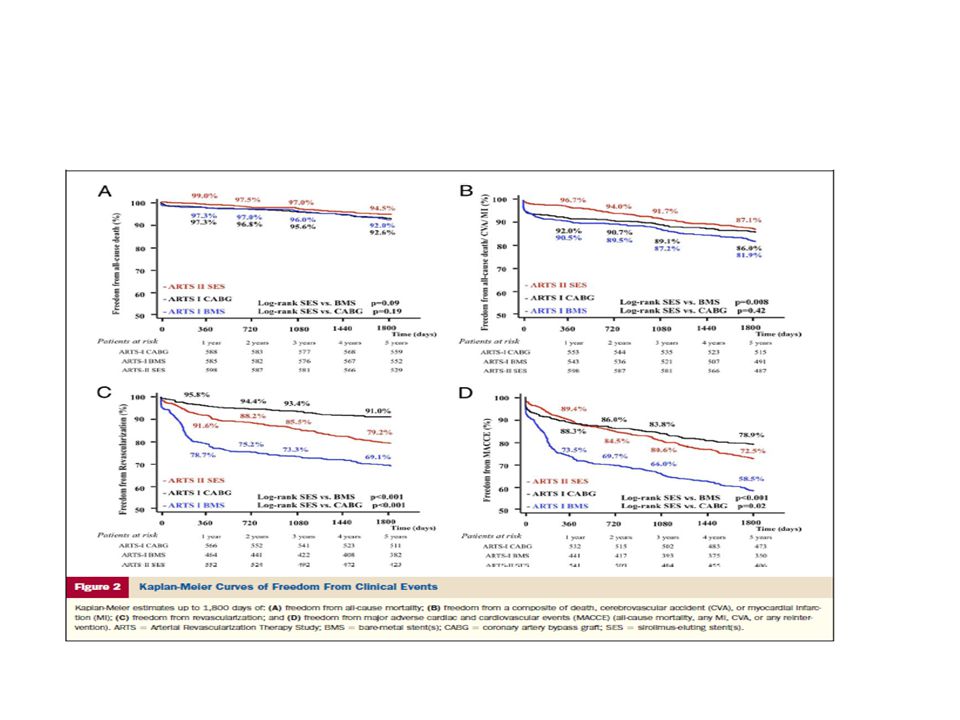
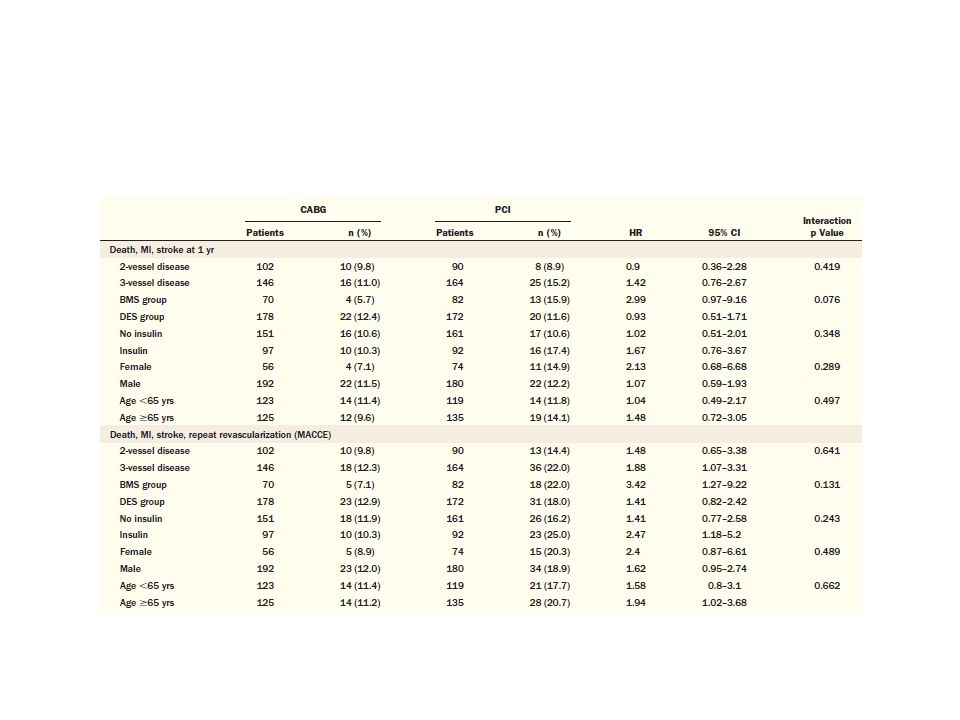
ARTS II Objectives The purpose of this study is to compare the 5-year clinical outcomes, safety, and efficacy of sirolimus-eluting stents (SES) in the ARTS II (Arterial Revascularization Therapies Study II) with the outcomes of coronary artery bypass graft (CABG) and bare-metal stenting (BMS) from the ARTS I. Background The long-term outcomes after SES implantation in patients with multivessel disease remains to be established. Methods The ARTS I was a randomized trial of 1,205 patients with multivessel disease comparing CABG and BMS. The ARTS II study was a nonrandomized trial with the Cypher sirolimus-eluting stent (Cordis, a Johnson & Johnson Company, Warren, New Jersey), applying the same inclusion and exclusion criteria, end points, and protocol definitions. The ARTS II trial enrolled 607 patients, with an attempt to enroll at least one-third of patients with 3-vessel disease. Results At 5-year, the death/stroke/myocardial infarction event-free survival rate was 87.1% in ARTS II SES, versus 86.0% (p 0.1) and 81.9% (p ) in ARTS I CABG and BMS cohorts, respectively. The 5-year major adverse cardiac and cerebrovascular event (MACCE) rate in ARTS II (27.5%) was significantly higher than ARTS I CABG (21.1%, p 0.02), and lower than in ARTS I BMS (41.5%, p ). The cumulative incidence of definite stent thrombosis was 3.8%. Thirty-two percent (56 of 176) of major adverse cardiac events (MACE) at 5 years were related to possible, probable, or definite stent thrombosis. Conclusions At 5 years, SES had a safety record comparable to CABG and superior to BMS, and a MACCE rate that was higher than in patients treated with CABG, and lower than in those treated with BMS. Approximately one-third of the events seen with SES could be prevented through the elimination of early, late, and very late stent thrombosis. (J Am Coll Cardiol 2010;55:1093–101) © 2010 by the American College of Cardiology Foundation
 in the ARTS II (Arterial Revascularization Therapies Study II) with the outcomes of coronary artery. bypass graft (CABG) and bare-metal stenting (BMS) from the ARTS I. Background The long-term outcomes after SES implantation in patients with multivessel disease remains to be established. Methods The ARTS I was a randomized trial of 1,205 patients with multivessel disease comparing CABG and BMS. The ARTS II study. was a nonrandomized trial with the Cypher sirolimus-eluting stent (Cordis, a Johnson & Johnson Company, Warren, New. Jersey), applying the same inclusion and exclusion criteria, end points, and protocol definitions. The ARTS II trial enrolled. 607 patients, with an attempt to enroll at least one-third of patients with 3-vessel disease. Results At 5-year, the death/stroke/myocardial infarction event-free survival rate was 87.1% in ARTS II SES, versus. 86.0% (p 0.1) and 81.9% (p 0.007) in ARTS I CABG and BMS cohorts, respectively. The 5-year major adverse. cardiac and cerebrovascular event (MACCE) rate in ARTS II (27.5%) was significantly higher than ARTS I. CABG (21.1%, p 0.02), and lower than in ARTS I BMS (41.5%, p 0.001). The cumulative incidence of definite. stent thrombosis was 3.8%. Thirty-two percent (56 of 176) of major adverse cardiac events (MACE) at 5. years were related to possible, probable, or definite stent thrombosis. Conclusions At 5 years, SES had a safety record comparable to CABG and superior to BMS, and a MACCE rate that was. higher than in patients treated with CABG, and lower than in those treated with BMS. Approximately one-third of. the events seen with SES could be prevented through the elimination of early, late, and very late stent. thrombosis. (J Am Coll Cardiol 2010;55:1093–101) © 2010 by the American College of Cardiology Foundation.")
18
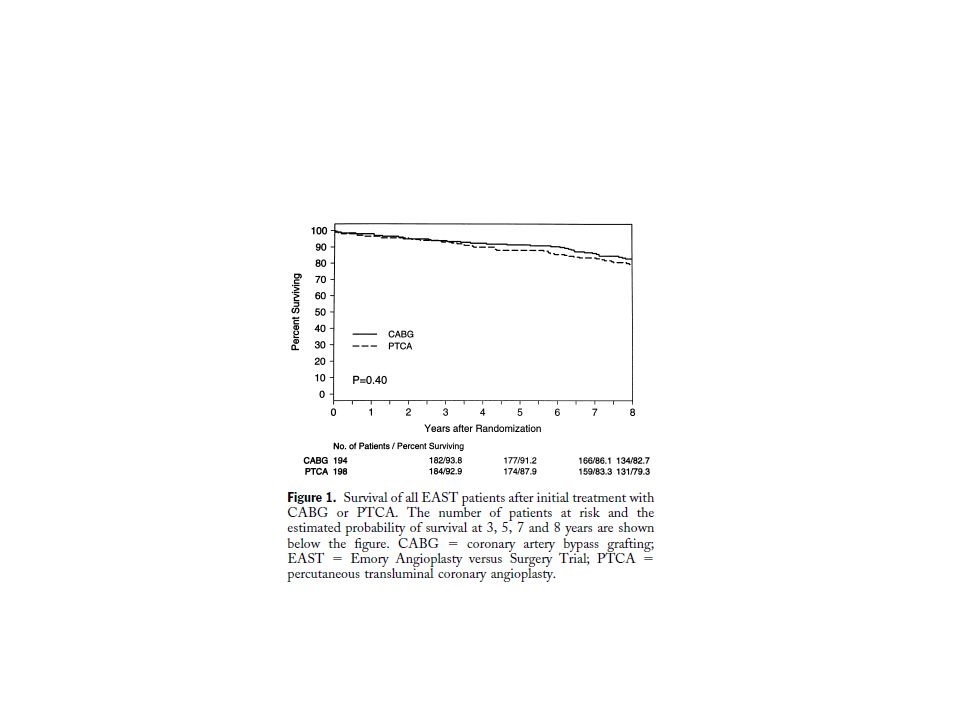
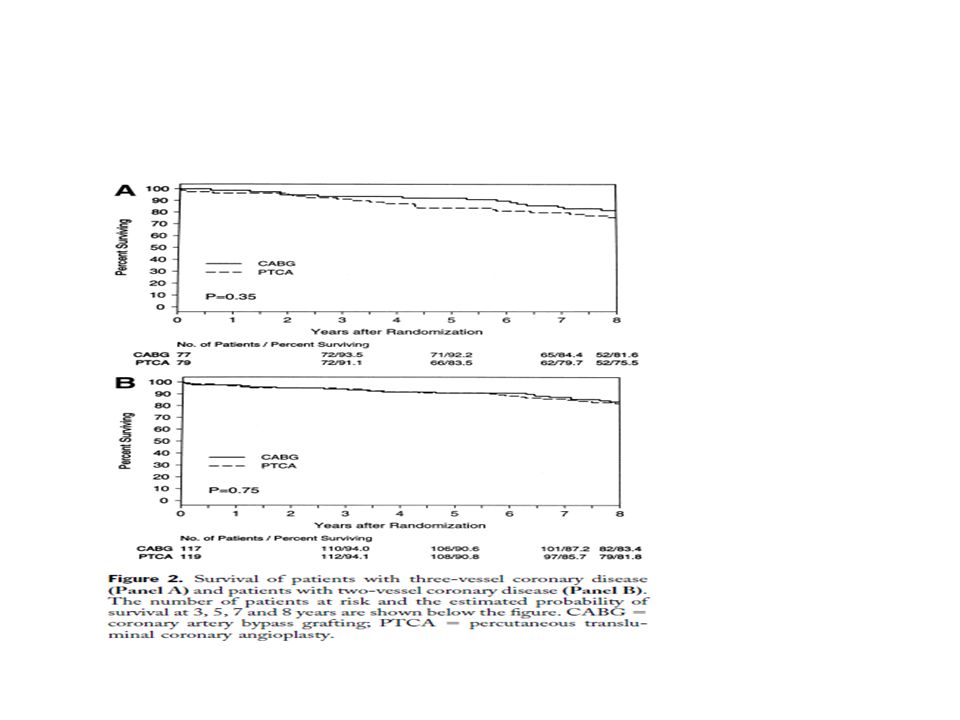
EAST OBJECTIVES To evaluate the long-term outcome of patients randomized to coronary bypass surgery or coronary angioplasty. BACKGROUND The Emory Angioplasty versus Surgery Trial (EAST) is a single center randomized comparison of a strategy of initial coronary angioplasty (n 5 198) or coronary bypass surgery (n 5 194) for patients with multivessel coronary artery disease. The primary end point (death, myocardial infarction or a large ischemic defect at 3 years) was not different, and repeat revascularization was significantly greater in the angioplasty group. Subsequently, the National Heart, Lung and Blood Institute supported a five-year extension of the trial. METHODS After the three year anniversary visit, annual questionnaires, telephone contact and examination of medical records were accomplished until death or the eight year anniversary in 100% of the patients surviving at 3 years. RESULTS Survival at 8 years is 79.3% in the angioplasty group and 82.7% in the surgical group (p 5 0.40). Patients with proximal left anterior descending stenosis and those with diabetes tended to have better late survival with surgical intervention although not reaching statistical significance. After the first 3 years, repeat interventions remained relatively equal for both treatment groups. CONCLUSIONS Long-term survival is not significantly different between angioplasty and surgery, and late (three to eight year) revascularization procedures were infrequent. Patients without treated diabetes had similar survival in both groups. (J Am Coll Cardiol 2000;35:1116 –21) © 2000 by the American College of Cardiology
 is a single center randomized. comparison of a strategy of initial coronary angioplasty (n 5 198) or coronary bypass surgery. (n 5 194) for patients with multivessel coronary artery disease. The primary end point (death, myocardial infarction or a large ischemic defect at 3 years) was not different, and repeat. revascularization was significantly greater in the angioplasty group. Subsequently, the. National Heart, Lung and Blood Institute supported a five-year extension of the trial. METHODS After the three year anniversary visit, annual questionnaires, telephone contact and examination. of medical records were accomplished until death or the eight year anniversary in 100% of the patients surviving at 3 years. RESULTS Survival at 8 years is 79.3% in the angioplasty group and 82.7% in the surgical group (p ). Patients with proximal left anterior descending stenosis and those with diabetes tended. to have better late survival with surgical intervention although not reaching statistical. significance. After the first 3 years, repeat interventions remained relatively equal for both. treatment groups. CONCLUSIONS Long-term survival is not significantly different between angioplasty and surgery, and late. (three to eight year) revascularization procedures were infrequent. Patients without treated. diabetes had similar survival in both groups. (J Am Coll Cardiol 2000;35:1116 –21) © by the American College of Cardiology.")
23
The Angina With Extremely Serious Operative Mortality Evaluation (AWESOME)
OBJECTIVES-- long-term percutaneous coronary intervention (PCI) and coronary artery bypas s graft (CABG) survival among post-CABG patients included in the Angina With Extremely Serious Operative Mortality Evaluation (AWESOME) randomized trial and prospective registry. BACKGROUND Repeat CABG surgery is associated with a higher risk of mortality than first-time CABG. The AWESOME is the first randomized trial comparing CABG with PCI to include post-CABG patients. METHODS Over a five-year period (1995 to 2000), patients at 16 hospitals were screened to identify a cohort of 2,431 individuals who had medically refractory myocardial ischemia and at least one of five high-risk factors. There were 454 patients in the randomized trial, of whom 142 had prior CABG. In the physician-directed registry of 1,650 patients, 719 had prior CABG. Of the 327 patient-choice registry patients, 119 had at least one prior CABG. The CABG and PCI survivals for the three groups were compared using Kaplan-Meier curves and log-rank tests. RESULTS The CABG and PCI three-year survival rates were 73% and 76% respectively for the 142 randomized patients (75 and 67 patients) (log-rank NS). In the physician-directed registry, 155 patients were assigned to reoperation and 357 to PCI (207 received medical therapy); 36-month survivals were 71% and 77% respectively (log-rank NS). In the patient-choice registry, 32 patients chose reoperation and 74 chose PCI (13 received medical therapy); 36-month survivals were 65% and 86% respectively (log-rank test p 0.01). CONCLUSION Percutaneous coronary intervention is preferable to CABG for many post-CABG patients. (J Am Coll Cardiol 2002;40:1951– 4) © 2002 by the American College of Cardiology Foundation
 and coronary. artery bypas s graft (CABG) survival among post-CABG patients included in the Angina. With Extremely Serious Operative Mortality Evaluation (AWESOME) randomized trial. and prospective registry. BACKGROUND Repeat CABG surgery is associated with a higher risk of mortality than first-time CABG. The AWESOME is the first randomized trial comparing CABG with PCI to include. post-CABG patients. METHODS Over a five-year period (1995 to 2000), patients at 16 hospitals were screened to identify a. cohort of 2,431 individuals who had medically refractory myocardial ischemia and at least one. of five high-risk factors. There were 454 patients in the randomized trial, of whom 142 had. prior CABG. In the physician-directed registry of 1,650 patients, 719 had prior CABG. Of. the 327 patient-choice registry patients, 119 had at least one prior CABG. The CABG and. PCI survivals for the three groups were compared using Kaplan-Meier curves and log-rank. tests. RESULTS The CABG and PCI three-year survival rates were 73% and 76% respectively for the 142. randomized patients (75 and 67 patients) (log-rank NS). In the physician-directed registry, 155 patients were assigned to reoperation and 357 to PCI (207 received medical therapy); 36-month survivals were 71% and 77% respectively (log-rank NS). In the patient-choice. registry, 32 patients chose reoperation and 74 chose PCI (13 received medical therapy); 36-month survivals were 65% and 86% respectively (log-rank test p 0.01). CONCLUSION Percutaneous coronary intervention is preferable to CABG for many post-CABG. patients. (J Am Coll Cardiol 2002;40:1951– 4) © 2002 by the American College of. Cardiology Foundation.")
25
Randomized Comparison of
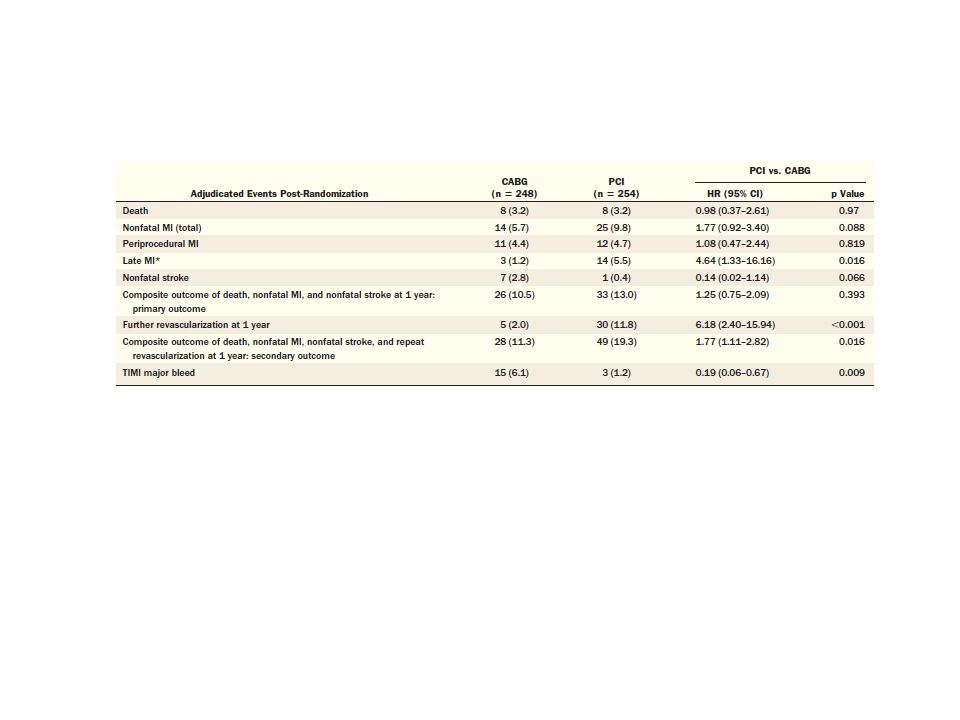
Percutaneous Coronary Intervention With Coronary Artery Bypass Grafting in Diabetic Patients 1-Year Results of the CARDia (Coronary Artery Revascularization in Diabetes) Trial Objectives The purpose of this study was to compare the safety and efficacy of percutaneous coronary intervention (PCI) with stenting against coronary artery bypass grafting (CABG) in patients with diabetes and symptomatic multivessel coronary artery disease. Background CABG is the established method of revascularization in patients with diabetes and multivessel coronary disease, but with advances in PCI, there is uncertainty whether CABG remains the preferred method of revascularization. Methods The primary outcome was a composite of all-cause mortality, myocardial infarction (MI), and stroke, and the main secondary outcome included the addition of repeat revascularization to the primary outcome events. A total of 510 diabetic patients with multivessel or complex single-vessel coronary disease from 24 centers were randomized to PCI plus stenting (and routine abciximab) or CABG. The primary comparison used a noninferiority method with the upper boundary of the 95% confidence interval (CI) not to exceed 1.3 to declare PCI noninferior. Bare-metal stents were used initially, but a switch to Cypher (sirolimus drug-eluting) stents (Cordis, Johnson & Johnson, Bridgewater, New Jersey) was made when these became available. Results At 1 year of follow-up, the composite rate of death, MI, and stroke was 10.5% in the CABG group and 13.0% in the PCI group (hazard ratio [HR]: 1.25, 95% CI: 0.75 to 2.09; p 0.39), all-cause mortality rates were 3.2% and 3.2%, and the rates of death, MI, stroke, or repeat revascularization were 11.3% and 19.3% (HR: 1.77, 95% CI: 1.11 to 2.82; p 0.02), respectively. When the patients who underwent CABG were compared with the subset of patients who received drug-eluting stents (69% of patients), the primary outcome rates were 12.4% and 11.6% (HR: 0.93, 95% CI: 0.51 to 1.71; p 0.82), respectively. Conclusions The CARDia (Coronary Artery Revascularization in Diabetes) trial is the first randomized trial of coronary revascularization in diabetic patients, but the 1-year results did not show that PCI is noninferior to CABG. However, the CARDia trial did show that multivessel PCI is feasible in patients with diabetes, but longer-term follow-up and data from other trials will be needed to provide a more precise comparison of the efficacy of these 2 revascularization strategies. (The Coronary Artery Revascularisation in Diabetes trial; ISRCTN ) (J Am Coll Cardiol 2010;55:432–40) © 2010 by the American College of Cardiology Foundation
 Trial. Objectives The purpose of this study was to compare the safety and efficacy of percutaneous coronary intervention (PCI) with stenting against coronary artery bypass grafting (CABG) in patients with diabetes and symptomatic multivessel. coronary artery disease. Background CABG is the established method of revascularization in patients with diabetes and multivessel coronary disease, but with advances in PCI, there is uncertainty whether CABG remains the preferred method of revascularization. Methods The primary outcome was a composite of all-cause mortality, myocardial infarction (MI), and stroke, and the. main secondary outcome included the addition of repeat revascularization to the primary outcome events. A. total of 510 diabetic patients with multivessel or complex single-vessel coronary disease from 24 centers were. randomized to PCI plus stenting (and routine abciximab) or CABG. The primary comparison used a noninferiority. method with the upper boundary of the 95% confidence interval (CI) not to exceed 1.3 to declare PCI noninferior. Bare-metal stents were used initially, but a switch to Cypher (sirolimus drug-eluting) stents (Cordis, Johnson. & Johnson, Bridgewater, New Jersey) was made when these became available. Results At 1 year of follow-up, the composite rate of death, MI, and stroke was 10.5% in the CABG group and 13.0% in. the PCI group (hazard ratio [HR]: 1.25, 95% CI: 0.75 to 2.09; p 0.39), all-cause mortality rates were 3.2% and. 3.2%, and the rates of death, MI, stroke, or repeat revascularization were 11.3% and 19.3% (HR: 1.77, 95% CI: 1.11 to 2.82; p 0.02), respectively. When the patients who underwent CABG were compared with the subset. of patients who received drug-eluting stents (69% of patients), the primary outcome rates were 12.4% and. 11.6% (HR: 0.93, 95% CI: 0.51 to 1.71; p 0.82), respectively. Conclusions The CARDia (Coronary Artery Revascularization in Diabetes) trial is the first randomized trial of coronary revascularization. in diabetic patients, but the 1-year results did not show that PCI is noninferior to CABG. However, the. CARDia trial did show that multivessel PCI is feasible in patients with diabetes, but longer-term follow-up and. data from other trials will be needed to provide a more precise comparison of the efficacy of these 2 revascularization. strategies. (The Coronary Artery Revascularisation in Diabetes trial; ISRCTN ) (J Am Coll. Cardiol 2010;55:432–40) © 2010 by the American College of Cardiology Foundation.")
30
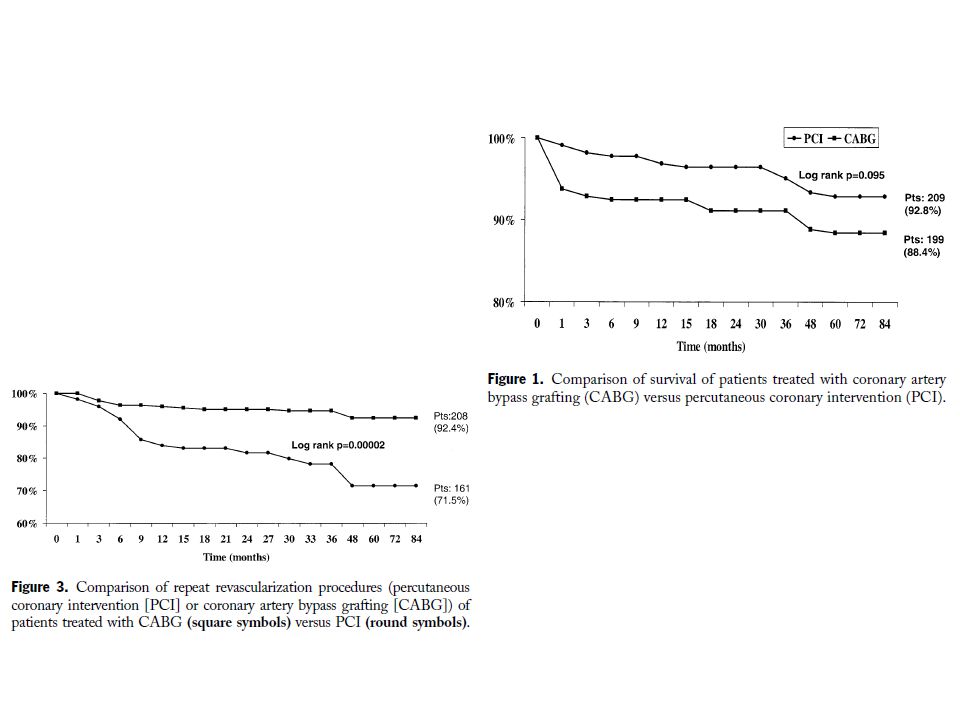
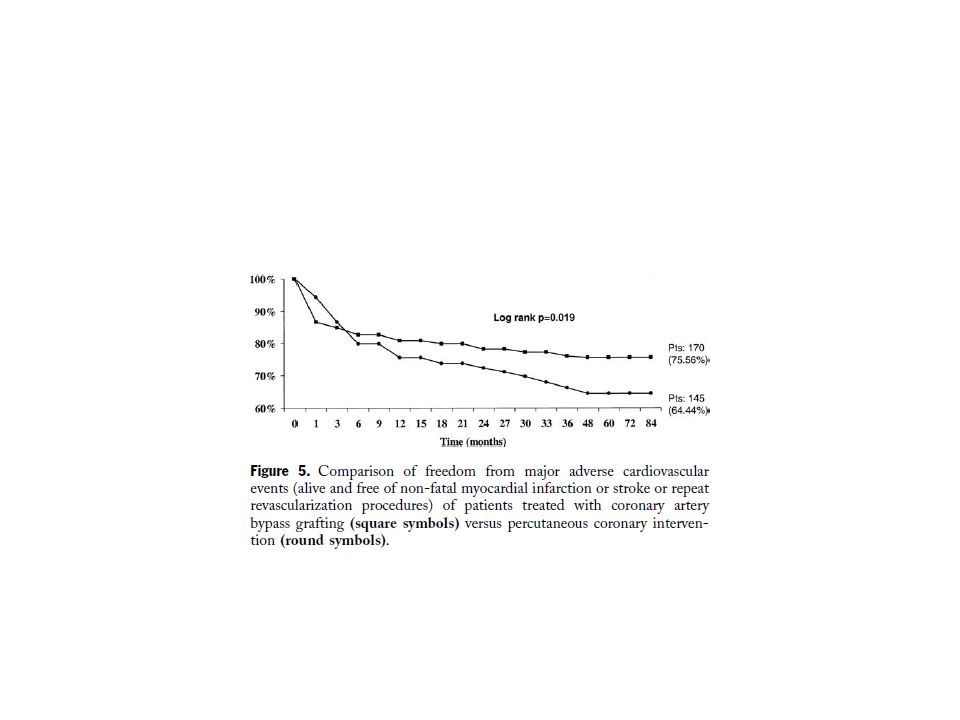
Five-Year Follow-Up of the Argentine
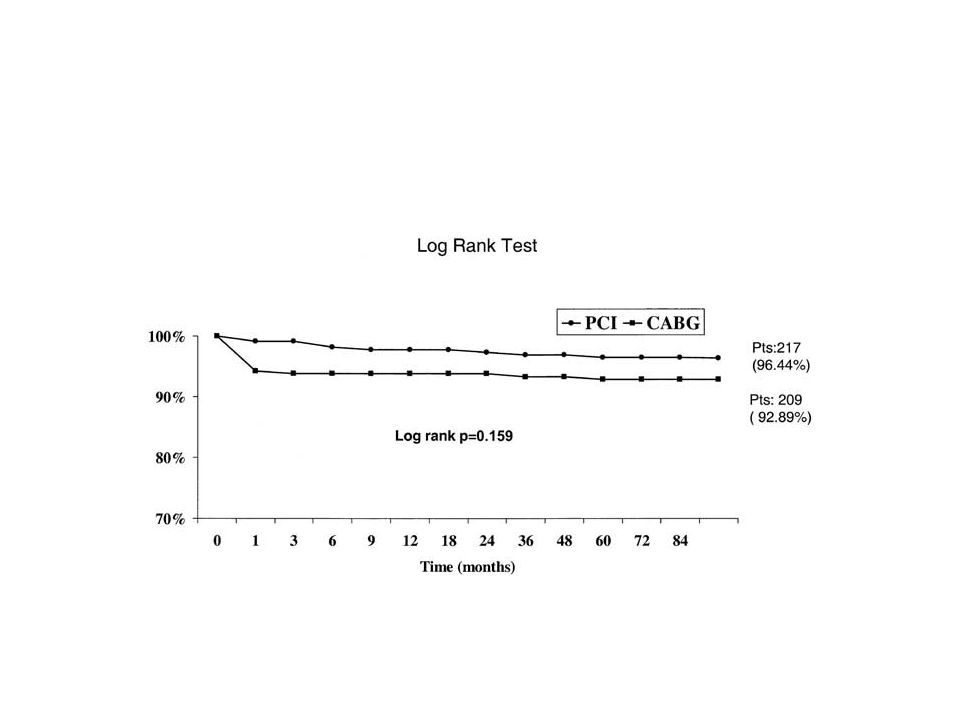
Randomized Trial of Coronary Angioplasty With Stenting Versus Coronary Bypass Surgery in Patients OBJECTIVES The purpose of the present study is to report the five-year follow-up results of the ERACI II trial. BACKGROUND Immediate and one-year follow-up results of the ERACI II study showed a prognosis advantage of percutaneous coronary intervention (PCI) with stents over coronary artery bypass grafting (CABG). METHODS A total of 450 patients were randomly assigned to undergo either PCI (n 225); or CABG (n 225). Only patients with multi-vessel disease were enrolled. Clinical follow-up during five years was obtained in 92% of the total population after hospital discharge. The primary end point of the study was to compare freedom from major adverse cardiovascular events (MACE) at 30 days, 1 year, 3 years, and 5 years of follow-up. RESULTS At five years of follow-up, patients initially treated with PCI had similar survival and freedom from non-fatal acute myocardial infarction than those initially treated with CABG (92.8% vs. 88.4% and 97.3% vs. 94% respectively, p 0.16). Freedom from repeat revascularization procedures (PCI/CABG) was significantly lower with PCI compared with CABG (71.5% vs. 92.4%, p ). Freedom from MACE was also significantly lower with PCI compared with CABG (65.3% vs. 76.4%; p ). At five years similar numbers of patients randomized to each revascularization procedure were asymptomatic or with class I angina. CONCLUSIONS At five years of follow-up, in the ERACI II study, there were no survival benefits from any revascularization procedure; however patients initially treated with CABG had better freedom from repeat revascularization procedures and from MACE. (J Am Coll Cardiol 2005;46: 582–8) © 2005 by the American College of Cardiology FoundationWith Multiple Vessel Disease (ERACI II)
 with stents over coronary artery. bypass grafting (CABG). METHODS A total of 450 patients were randomly assigned to undergo either PCI (n 225); or CABG. (n 225). Only patients with multi-vessel disease were enrolled. Clinical follow-up during. five years was obtained in 92% of the total population after hospital discharge. The primary. end point of the study was to compare freedom from major adverse cardiovascular events. (MACE) at 30 days, 1 year, 3 years, and 5 years of follow-up. RESULTS At five years of follow-up, patients initially treated with PCI had similar survival and freedom. from non-fatal acute myocardial infarction than those initially treated with CABG (92.8% vs. 88.4% and 97.3% vs. 94% respectively, p 0.16). Freedom from repeat revascularization. procedures (PCI/CABG) was significantly lower with PCI compared with CABG (71.5% vs. 92.4%, p ). Freedom from MACE was also significantly lower with PCI compared. with CABG (65.3% vs. 76.4%; p 0.013). At five years similar numbers of patients. randomized to each revascularization procedure were asymptomatic or with class I angina. CONCLUSIONS At five years of follow-up, in the ERACI II study, there were no survival benefits from any. revascularization procedure; however patients initially treated with CABG had better freedom. from repeat revascularization procedures and from MACE. (J Am Coll Cardiol 2005;46: 582–8) © 2005 by the American College of Cardiology FoundationWith Multiple Vessel Disease (ERACI II)")
Similar presentations





















>")




: a Randomized Controlled Clinical Trial of Therapeutic Strategies.>")
