Download presentation
Presentation is loading. Please wait.

1
Just a Biopsy Sara is 19 yrs old girl, Presented to the hospital with history of Progressive SOB, cough weight loss and fatigability for 6 weeks. Dyspnoea occurs with minimal exertion and and associated with orthopnea. Cough is productive of yellowish sputum with occasional hemoptysis.

2
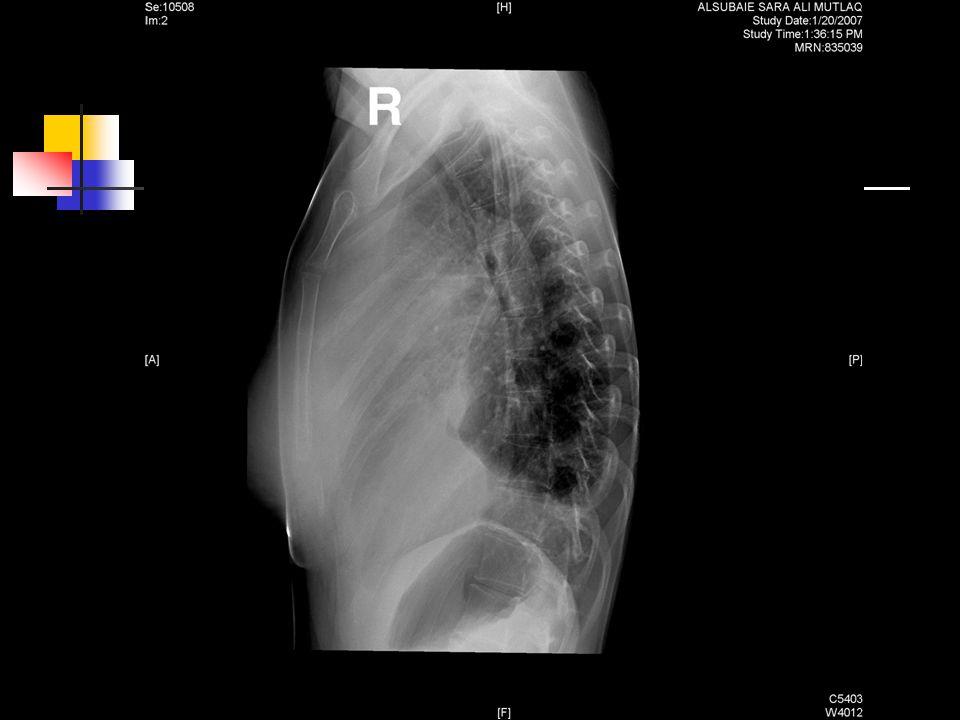
Week before admission she started to have dysphagia. She was admitted to Medical ward on 25/12/1427 for further investigations and management. Routine investigations were done. CXR showed huge mediastinal mass

5
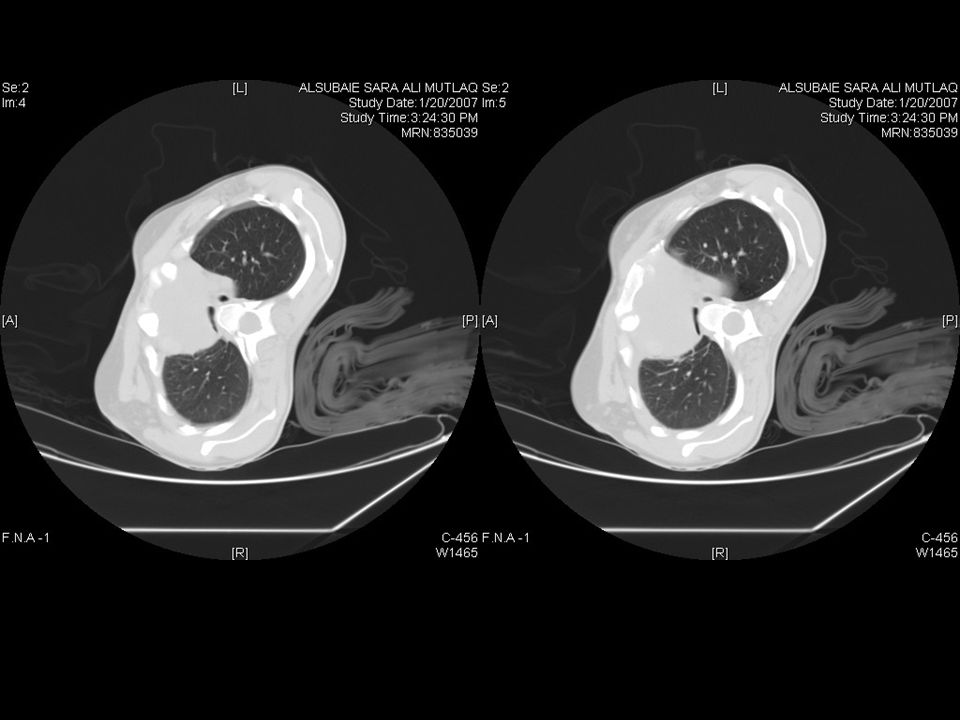
Then, The patient was booked for urgent chest CT scan and CT guided biopsy but procedure was cancelled because the patient can not lie down (flat on the bed). CT done in (semi) lateral position.
 lateral position..")
8
Pleural tap was done and there was no evidence of malignant cell. Mediastinoscopic biopsy was taken But the result was not informative and TRUE CUT biopsy was suggested To reach the diagnosis. On 5/1/28 the patient was booked for emergency mini thoracotomy and true cut Biopsy.

9
Preoperative Anesthetic Assessment History: Clinical Examination: She was looking fair. Conciuos,alert and oreinted. She can lie comfortable only on right lateral position. She was afebrile, with normal vital signs. RR 18, HR 80, BP 110/60, Spo2 98% on RA.

10
Cont.. PreOperative Anesthetic Assessment CVS: NAD Resp: Good air entry Bilatrally with harsh breath sounds. A.W: Mallampati 1, TMD >6.5cm She has dilated Neck Veins and over the right side of the chest (SVC obstruction).
..")
11
Cont.. PreOperative Anesthetic Assessment Biochemical analysis, normal PFT: was done but the patient was not able to do it Properly. PredPrePre/ Pred FVC3.58.9526.7 FEV13.21.8125.1 FEV1/ %fvc 89.284.394.5 PEF6.962.0729.8

12
Cont.. PreOperative Anesthetic Assessment Preoperative Orders ECG,ABG were Requested. High Risk Consent. ICU bed.

13
Cont.. PreOperative Anesthetic Assessment ECG : Right Axis Deviaton. ABG : Normal. MICU bed was Available. So the patient was taken for the O.R. on Wednesday 5/2/1428.

14
IntraOperative Course Induction Routine monitors were attached. 18 G cannula was inserted. Inhalational induction with Sevoflurane 8% with O2 while the patient in semi sitting position. Sedating dose of propofol was used 40mg plus 50 mcg of fentanyl.

15
Cont.. IntraOperative Course Lidocaine 10% was sprayed on the base of the tongue and Pharynx. 2ml of 2%lidocaine was injected intratracheal. By ordinary laryngoscope patient was intubated with 7.0 ETT, smooth intubation. Another dose of fentanyl 50mcg was given.

16
Cont.. IntraOperative Course Then the patient was kept spontaneously Breathing with some assistance manually as needed. A.W pressure was high during manual assistance of ventialtion, because the patient was almost flat during Surgical Procedure.

17
Cont.. IntraOperative Course The Procedure lasted almost 40 minutes during which the patient was hemodynamiclly stable. SpO2 98-99%, EtCO2 60-85. Multiple Biopsies were taken After aspiration from Anterior Mediastinal mass Through the left 2 nd Intercostal Space and left ICT was inserted.

18
Cont.. IntraOperative Course Intraoperative Bronchoscopy was done which showed external compression on trachea and bronchi.

20
Cont.. IntraOperative Course At the end of The Procedure The patient was given A chance of Extubation But She did not gain consciousness and maintain good ventilatory parameter. So she was Re Intubated and kept spontaneously breathing with CPAP and was transferred to MICU.

21
PostOperative Course In MICU the patient was kept Intubated sedated and Ventilated for 7days. In the first day she developed High Airway Pressure and desaturation which was solved by Changing the patient Positioning…(Positioning!) PCV: FiO2 0.4, P:20 Tv:600+, R18.
 PCV: FiO2 0.4, P:20 Tv:600+, R18..")
22
Cont.. PostOperative Course On 6/1/28 the result of the Biopsy was revealed As: NON-HODGKIN LYMPHOMA B-CELL TYPE. Same day Chemotherapy was started. On 9/1/28, Bronchoscopy was done which showed external compression at carina almost complete during Expiration.

24
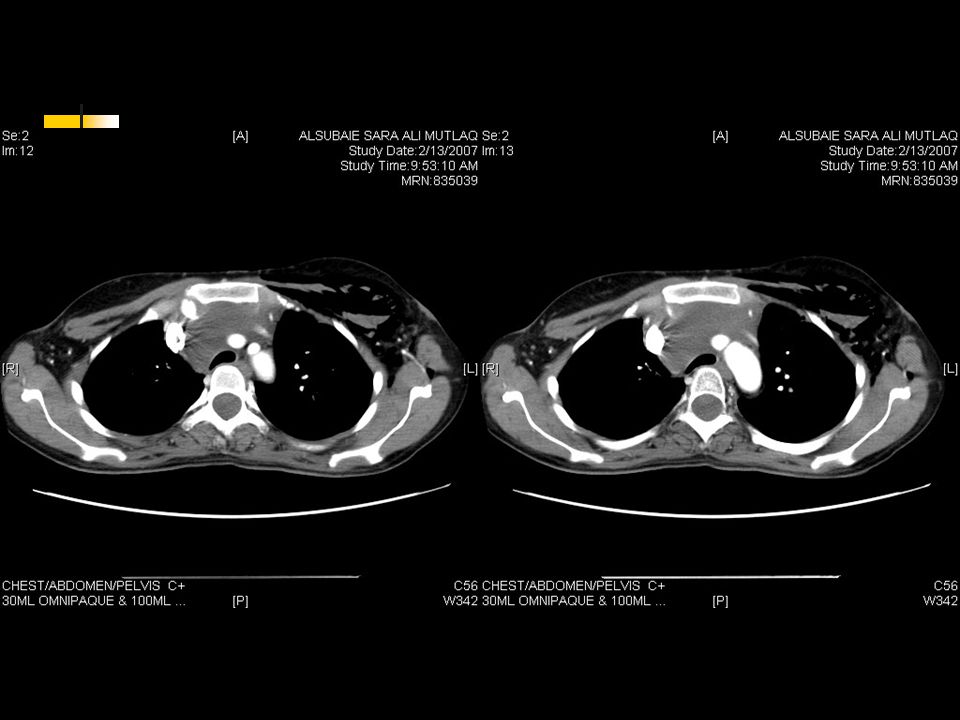
Cont.. PostOperative Course Five days after Chemotherapy the patint was extubated - (12/1/28). And she was kept for Four days in MICU. On 16/12/28 the patient was discharged from MICU to the medical ward and She was able to lie flat without any respiratory compromise. On 17/1/28, CT scan of the chest was repeated.

28
On 29/1/28, the patient was discharged from the hospital with home medicines and appointments For investigations and follow up for further Chemotherapy cycles.

29
Before ChemoRxAfter ChemoRx

30
Before ChemoRxAfter ChemoRx

Similar presentations























 Seen In OPD 2/12 History SOB,Dry Cough, Wt loss.>")


