Download presentation
Presentation is loading. Please wait.

5
Abdulwahab Telmesani FRCPC, FAAP Associate Prof. of Pediatrics Umm Al-Qura University INFLAMMATORY BOWEL DISEASE IN CHILDREN

6
CROHN’S DISEASE ULCERATIVE COLITIS INDETERMENANT (non specific) COLITIS INFLAMMATORY BOWEL DISEASE IN CHILDREN
 COLITIS INFLAMMATORY BOWEL DISEASE IN CHILDREN")
7
1/3 of the incidence of IBD occurs in < 20 years of Age INFLAMMATORY BOWEL DISEASE IN CHILDREN

8
Highest in Scandinavian Western European North American Jews > Non Jews Urban > Rural Lowest in Asian African South American INFLAMMATORY BOWEL DISEASE IN CHILDREN

9
10-25% in first degree relatives 7% in siblings Linkage with chromosome 16, 12, 14, 19, 6 & 1 STRONG GENETIC PREDISPOSITION

10
IBD IN SAUDI ARABIA Not Uncommon Adult > Children UC > CD Milder than the west

11
Proinflammatory Cytokines & Eicosanoids Active inflammation Increase permeability & vasodilatation Symptoms & Signs Cont.# PATHOPHYSILOLOGY

12
SYMPTOMS / SIGNS: Diarrhea Abdominal pain Protein Loss Bleeding Electrolyte Loss Stricture Formation PATHOPHYSIOLOGY

13
CROHN’S DISEASE 90% of patients have small bowel affected Classically terminal ileum 10-15% Only colon affected 60% Ileocolitis 20% have perirectal disease Cont.# EXPRESSION & DISTRIBUTION

14
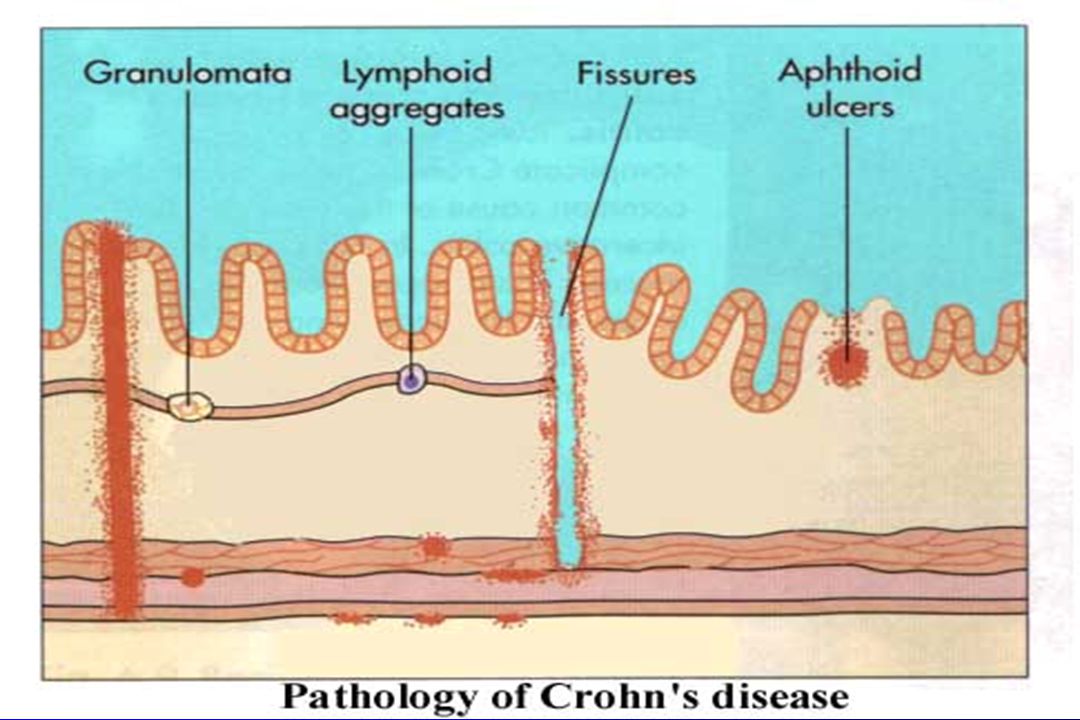
Trans mural inflammation Fistulas arise when inflammation extends through the serosa (Bladder, Vagina, Perineum) Granuloma is the Hallmark of Chron’s disease, found in 30% of all cases. EXPRESSION & DISTRIBUTION

17
ULCERATIVE COLITIS 5% Proctitis 10-15% proctosigmoiditis 30-40% up to splenic flexure 50% pancolitis Almost always starts at the rectum Pathology limited to the mucosa Crypt abscesses, distorted architecture & goblet cell depletion, are typical EXPRESSION & DISTRIBUTION

18
ULCERATIVE COLITIS Commonly Bloody mucoid diarrhea frequent loose stool lower abdominal pain more with defecation PRESENTATION Fulminant disease (10-15% of PT’s) > 6 Bloody stools per day Abdominal tenderness Fever, tachycardia Anemia Hypoalbuminemia Cont.#
 > 6 Bloody stools per day Abdominal tenderness Fever, tachycardia Anemia Hypoalbuminemia Cont.#")
19
Constipation in proctitis Colonic carcinoma 1% by 10 years 1-2%per year thereafter Anorexia &Weight loss < Crohn’s Disease PRESENTATION{CONTD}

23
PRESENTATION CROHN’S DISEASE Abdominal pain ( awakens patient from sleep) Site of disease dictates the nature & site of pain Ileum RT quadrant pain Gastroduodinal dyspeptic pain Diarrhea & Rectal Bleeding may resemble U.C. Cont.#

24
PRESENTATION Perianal disease(Fissures, fistulas & skin tags) Intestinal obstruction is common Abscesses (Interloop, intramesentric, retroperitoneal, iliopsoas or subdiaphragmatic) Carcinoma (Crohn’s Colitis)
 Intestinal obstruction is common Abscesses (Interloop, intramesentric, retroperitoneal, iliopsoas or subdiaphragmatic) Carcinoma (Crohn’s Colitis)")
28
EXTRAINTESTINAL MANIFESTATIONS SYSTEMICLOCALISED Fever Eyes {C.D. > U.C. } Joints MalaiseSkin Anorexia + wt lossLiver {C.D. 40% > U.C. 10%}Bone Delayed Growth & Kidneys Sexual Development Vascular {C.D. > U.C.}Hematological Heart

29
EXTRAINTESTINAL MANIFESTATIONS EYE Uveitis, Episcleritis, Keratitis, RetinalVasculitis LIVER Sclerosing cholangitis U.C.>C.D. SKIN Erythema nodosum C.D.>U.C. Pyoderma gangrenosum U.C.> C.D.

30
EXTRAINTESTINAL MANIFESTATIONS - JOINTS Arthralgia or Arthritis, Knees > Ankles > Hips> Wrists> Elbow Most common localised manifestations {ankylosing spondylitis, sacroilitis}U.C.>C.D. - BONE Demineralization {Steroid+Rest+Vit D def,Decreased Protein} - KIDNEYS Ca oxalate,Ca phosphate,Uric acid. Inflammation

31
EXTRAINTESTINAL MANIFESTATIONS -VASCULAR Thrombocytosis Thrombophlebitis Activation of clotting cascade - HEMATOLOGICAL Anemia {B12 +Folic Acid def.} Effect of chemotherapy - HEART Perimyocarditis (good prognosis)
")
34
DIAGNOSIS Hx & P/E: Stool Analysis + C/S WBC N or slightly elevated ESR Elevated 70 % Thrombocytosis 60% Albumin

35
DIAGNOSIS Endoscopy Vs Radiology

36
ENDOSCOPY Sigmoidoscopy Colonoscopy Ileum Upper endoscopy

37
ULCERATIVE COLITIS Mucosa: Erythematus Granular Friable Loss of normal vascular

39
CROHN’S Aphus Lesions Psudopolyps Patchy Distribution Bx normal mucosa

41
RADIOLOGY -Upper G.I. Series Irrigular nodular and thickend bowel loops stenosis, ulcers & fistulas -Abdominal U/S & C.T. for complication of Crohn’s Disease

42
TREATMENT AIM: Relief of symptoms Improve quality of life Improve growth

43
TREATMENT Pharmacotherapy Nutrition Surgery

44
TREATMENT Pharmacotherapy: 5- Aminosalicylate (P.O. Knema) Sulfasalzine
 Sulfasalzine")
45
TREATMENT Corticosteroids: Prednisone Budesonide

46
TREATMENT Antibiotics: Metronidazol Ciprofloxacin

47
TREATMENT Immunomodulators: 6- mercaptopurine Asathioprine Cyclosporine

48
TREATMENT Anti-tumer necrosis factor -Alpha Infliximab CDP571 Thalidomide Others

49
TREATMENT Clonidine (better than Sulfasulazine) Na chromoglycate (No favorable effect)
 Na chromoglycate (No favorable effect)")
50
ANTIDIARRHEAL DRUGS Loperamide : Frequency of Diarrhea Contraindicated in sever colitis

51
SURGERY Indications: Intractability Hemorrhage Perforations Obstructions Carcinoma

52
SURGERY 10-25% of U.C. will need colectomy with in 5 years of diagnosis. 50-75% of Crohn’s Disease will require Sx with in 10-15 years of diagnosis.

53
NUTRITION - Elemental diet alone may in duce remission in Crohn’s disease - May need N.G. feeding - Caloric intake growth catch-up

Similar presentations




















, FRCS (Glasg), FAMS, DNB, FACS, FICS Professor of Surgery.>")

 Kristina Blaslov Mentor: A. Žmegač Horvat.>")





 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")


: –5 cases per 100,000 –High incidence in.>")
 Idiopathic IBD is comprised of CD+UC and is characterized by chronic bowel inflammation. Idiopathic IBD is comprised of.>")

