Download presentation
Presentation is loading. Please wait.

1
GOOD MORNING www.anaesthesia.co.inwww.anaesthesia.co.in anaesthesia.co.in@gmail.comanaesthesia.co.in@gmail.com

2
Oxygen Therapy & O 2 Delivery Systems Piyush / Dr.Chitra

3
Oxygen Colorless,odorless Scheele prepared before Priestley but could not recognise it. By Priestley in 1774 MW-32 Noninflammable but strongly helps combustion

4
Oxygen cascade During transit from the ambient air to the cellular structures the po2 oxygen drops from 152mm Hg to a few mmHg in the mitochondria this gradient drop is described as oxygen cascade

5
O 2 Cascade Air mitochondria

6
O 2 Cascade Atm. Air (dry) Lower Resp. Tract (moist 37 o c) 159mm Hg (20.95 % of 760) 149mm Hg 20.95 % of 713 (760-47) Humidification 6 Vol % (47mm Hg)
 159mm Hg (20.95 % of 760) 149mm Hg % of 713 (760-47) Humidification 6 Vol % (47mm Hg).")
7
O 2 Cascade 149mm Hg (20.95 % of 713) O 2 consumption Lower Resp. Tract (moist 37 o c) Alv. ventilation Alveolar air 101mm Hg P A O 2 = F I O 2 (Pb – 47) – PaCo 2 x F
 Alv. ventilation Alveolar air 101mm Hg P A O 2 = F I O 2 (Pb – 47) – PaCo 2 x F.")
8
O 2 Cascade Venous admixture 101mm Hg Alveolar air Arterial blood 97mm Hg P a O 2 = 100 – 0.3 x age (years) mm Hg A – a = 4 – 25 mmHg
 mm Hg A – a = 4 – 25 mmHg")
9
Venous admixture ( physiological shunt) O 2 Cascade Low VA/QNormal True shunt (normal anatomical shunt) Pulmonary (Bronchial veins) Extra Pulm. (Thebesian veins) Normal = upto 5 % of cardiac output
 Normal = upto 5 % of cardiac output.")
10
O 2 Cascade Utilization by tissue Arterial blood P a O 2 = 97mm Hg (Sat. > 95 %) Mixed Venous blood P V O 2 = 40mm Hg Sat. 75% Cell Mitochondria PO 2 7 – 37 mmHg Pasteur point – The critical level for aerobic metab. to continue (PO 2 1-2 mmHg in mitochondria, 22mmHg in capillary)
 Mixed Venous blood P V O 2 = 40mm Hg Sat. 75% Cell Mitochondria PO 2 7 – 37 mmHg Pasteur point – The critical level for aerobic metab. to continue (PO mmHg in mitochondria, 22mmHg in capillary).")
11
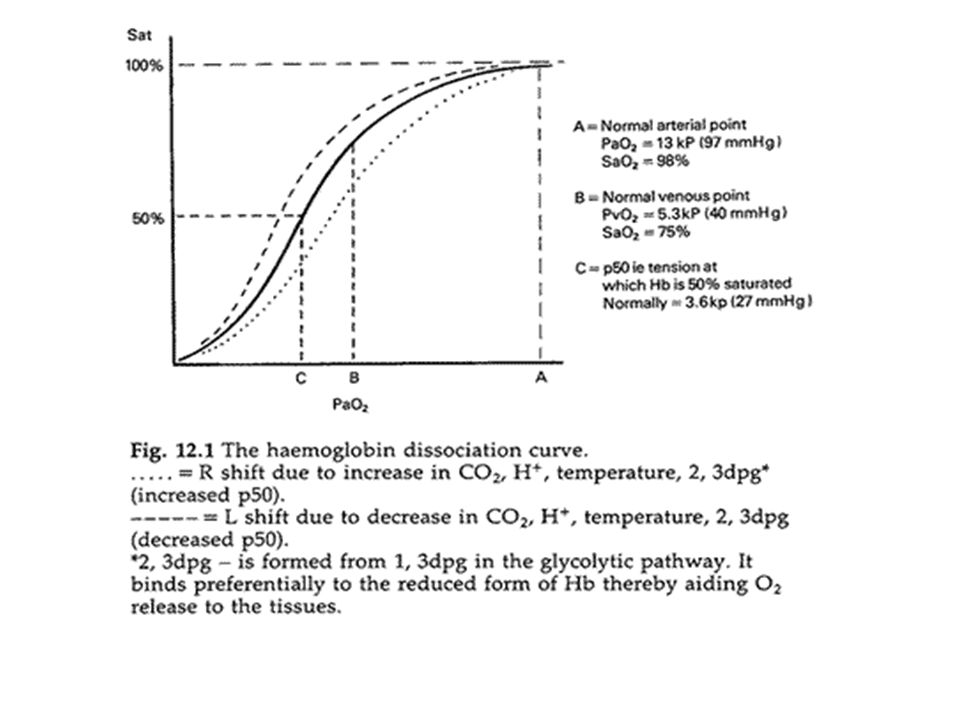
Blood Oxygen Content and Dissociation Curve ODC relates the saturation of the hemoglobin to the PO2. It is a sigmoid in shape.

13
Arterial oxygen content: O2.CONT=HbX1.34XSaO2 + PaO2 X.0034 = 15 x 1.34 x 0.98 = 20 ml 100 ml-1 of blood (ignoring that dissolved in plasma) or = 200 ml l-1
 or = 200 ml l-1")
14
Dissolved O 2 in plasma Breathing Air (P a O 2 100mm Hg) 0.3ml / 100ml of blood Breathing 100% O 2 (P a O 2 600mm Hg) 1.8ml / 100ml of blood Breathing 100% O2 at 3 Atm. Pressure 5.4ml / 100ml of blood

15
Oxygen delivery/Flux It is amount of oxygen carried by arterial blood per minute. Overall oxygen delivery = arterial oxygen content x cardiac output Oxygen delivery = 5 x 200 = 1000 ml min-1

16
Oxygen Therapy Indications

17
Criteria for Ordering Oxygen Therapy PaO 2 at or below 55 mm Hg Saturation O 2 < 88% resting PO 2 <55 mm Hg or < 88% for 5 min. (sleep) A drop in PO 2 10 mm Hg or 5% in O 2 sat. during sleep Symptoms or signs of heart failure (cor pulmonale), pulmonary hypertension, erythrocytosis, “P” pulmonale on EKG PO 2 <55 mm Hg or < 88% during exercise
 A drop in PO 2 10 mm Hg or 5% in O 2 sat. during sleep Symptoms or signs of heart failure (cor pulmonale), pulmonary hypertension, erythrocytosis, P pulmonale on EKG PO 2 <55 mm Hg or < 88% during exercise.")
18
Oxygen Therapy Indications F I O 2 - F I O 2 during anaes. - Rebreathing Barometric Pressure - High altitude PIO2PIO2 PAO2PAO2 O 2 Consumption -convulsions -thyrotoxicosis -shivering -pyrexia (7 % / o C) Alveolar Ventilation -resp. depression -Resp. muscle paresis - resp.effort (trauma) -airway obstruction
 Alveolar Ventilation -resp. depression -Resp. muscle paresis - resp.effort (trauma) -airway obstruction.")
19
Oxygen Therapy Indications Low VA/Q Abn. Pulmonary shunt - pneumonia -lobar atelectasis -ARDS Normal Anat. shunt Abn.extra Pulm. Shunt cong. heart disease (R L ) PaO 2 Cell PO 2 Hb concentration -Anaemia -CO poisoning Perfusion local - PVD, thrombosis gen – shock, Hypovol., card. Failure cardiac arrest Hypoxia
 PaO 2 Cell PO 2 Hb concentration -Anaemia -CO poisoning Perfusion local - PVD, thrombosis gen – shock, Hypovol., card. Failure cardiac arrest Hypoxia.")
20
Hypoxia– lack of adequate oxygen in the blood – 4 types of hypoxia Hypoxic Hypoxia – lack of O2 in air Anemic Hypoxia – decreased hemoglobin (Hgb) level in blood Ischemic (Stagnant) Hypoxia – decreased blood flow (heart) Dysoxic (Tissue) Hypoxia – Cells unable to use O2 in blood – Cyanide poisoning
 level in blood Ischemic (Stagnant) Hypoxia – decreased blood flow (heart) Dysoxic (Tissue) Hypoxia – Cells unable to use O2 in blood – Cyanide poisoning")
21
Benefit of O 2 therapy in Hypoxia Hypoxic hypoxia (gas phase) + + + Anaemic hypoxia (fluid phase – const.) + Stagnant hypoxia (fluid phase – flow) + Histotoxic hypoxia (tissue phase) -
 Anaemic hypoxia (fluid phase – const.) + Stagnant hypoxia (fluid phase – flow) + Histotoxic hypoxia (tissue phase) -")
22
Dark side of oxygen therapy

23
Oxygen induced Free Radical Cell Injury It can occur due to overzealous use of oxygen which produces reactive oxygen species (ROS) as a metabolite. Major ROS are Superoxide (O 2.- ) Hydrogen peroxide (H 2 O 2 ) Hydroxyl radical (HO. )
 Hydrogen peroxide (H 2 O 2 ) Hydroxyl radical (HO. ).")
25
Free Radical Mediation of Cell Injury Free Radical Injury Mechanisms –Lipid peroxidation of membranes double bonds in polyunsaturated lipids –Lesions in DNA reactions with thymine with single-strand breaks –Cross-linking of proteins Leading to denaturation

26
Cellular defenses against ROS (Antioxidants ) Enzymatic –SOD, catalase, GPX Non-enzymatic –Vitamins A, C, E –Glutathione – selenium –Ceruloplsmin and transferrin
 Enzymatic –SOD, catalase, GPX Non-enzymatic –Vitamins A, C, E –Glutathione – selenium –Ceruloplsmin and transferrin")
27
OXYGEN THERAPY APPARATUS AND DEVICES

28
Oxygen sources and delivery There are three typical sources of oxygen used therapeutically: Liquid oxygen is contained in thermally insulating tanks. The liquid has to boil changing into a gas for breathing. Large tanks are used by hospitals. Small tanks can be used domestically. Liquid oxygen tanks are refilled by liquid oxygen suppliers.Liquid oxygentanks Cylinders contain compressed gaseous oxygen. Small cylinders are used for first aid and for home oxygen patients when mobility is required. Cylinders are refilled by a gas supplier.Cylinders

30
Oxygen concentrators are electrically powered devices which remove nitrogen from air.Oxygen concentratorsnitrogenair They are most commonly used in a domestic situation, because they do not need refilling. FIO 2 is never 100% The higher the liter flow setting the lower the FIO 2

31
O 2 Delivery systems Ambient pressure –Variable performance devices –Fixed performance devices Positive pressure ventilation –Non invasive (BIPAP, CPAP) –Invasive ECMO
 –Invasive ECMO")
32
O 2 Delivery systems Ambient pressure –Variable performance devices (Pt. dependent) low flow No capacity system – no rebreathing nasal catheter / cannulae Capacity system – chance of rebreathing –Small – (mass shell only) –Large – (with reservoir bag) –Fixed performance devices (Pt. independent) high flow HAFOE (ventimask) Anaesthesia circuits
 low flow No capacity system – no rebreathing nasal catheter / cannulae Capacity system – chance of rebreathing –Small – (mass shell only) –Large – (with reservoir bag) –Fixed performance devices (Pt. independent) high flow HAFOE (ventimask) Anaesthesia circuits.")
33
Nasal Catheter simplest, most common appliance Approximate FiO2’s: – 1 L/m O2 = 20% + 4% – assume patient is breathing “normally” Liter flow not to exceed 6 L/m – not well tolerated by patients – FiO2 doesn’t increase over 6 L/m

34
Nasal Catheter Merits Easy to fix Keeps hands free Not much interference with further airway care Small but definite rise in FiO 2 (dose not critical) Demerits Mucosal irritation (uncomfortable) Gastric dilatation (especially with high flows)
 Demerits Mucosal irritation (uncomfortable) Gastric dilatation (especially with high flows)")
35
Simple face mask “Extension” of anatomic reservoir to provide higher FiO2’s Flow: 6-10 L/m – Ensure flush of CO2 FiO2: 35-60% Dependent on: – oxygen flow – mask seal to face – ventilatory pattern exhale air through side holes

36
Face Masks Merits Higher Oxygen Conc. Demerits Proper fitting is required Rebreathing (if O 2 flow is inadequate) Interfere with further airway care Uncomfortable (sweating, spitting)
 Interfere with further airway care Uncomfortable (sweating, spitting).")
37
Partial Rebreather Uses bag as additional reservoir Exhaled air mixed with 100% O2 in bag – 1st 1/3 of exhaled air is anatomic dead space gas with very little CO2 Bag fills, directs remaining 2/3 of exhaled air out the vent holes

38
Non-Rebreather No exhaled gas is rebreathed Flap covers vent hole One-way valve between bag and mask Can achieve 90+% FiO2 Flow adjusted same as partial RB

39
Venturi mask The venturi mask, also known as an air- entrainment mask, is a medical device to deliver a known oxygen concentration to patients on controlled oxygen therapy. The mechanism of action depends on the venturi effect.

40
The Venturi effect is the fluid pressure that results when an incompressible fluid flows through a constricted section of pipe. The Venturi effect may be derived from a Bernoulli's principle. Bernoulli's principle The fluid velocity must increase through the constriction while its pressure must decrease due to conservation of energy: the gain in kinetic energy is supplied by a drop in pressure or a pressure gradient force.velocityconservation of energykinetic energy pressure gradient force

43
The color of the device reflects the delivered oxygen concentrationfor blue = 24%; white = 28%; orange = 31%; yellow = 35%; red = 40%; green = 60%.

44
Entrainment ratio = Entrained flow/driving flow As 9 to 1 ratio indicates that there are 9lit/min being entrained by a driving gas of 1 lit/min.

45
HIGH FLOW DEVICE (venturi principle) FiO2% O2 flow l/m 244 286 318 3510 4012 5015 O2:air Totalflowl/m 1:25 105 1:10 68 1:7.0 63 1:4.6 56 1:3.2 50 1:1.67 32
 FiO2% O2 flow l/m O2:air Totalflowl/m 1: : : : : :")
46
Paediatric oxygen therapy

47
Incubator Small infants – not on ventilator Works on venturi principle Complete air change – 10 times / hour Control of humidity & temperature O 2 conc. falls rapidly when access ports are open

48
Oxygen hood Used for infants. Made up of transparent plexiglass box. Placed over infant head and neck to ensure adequate FiO2. Oxygen flow should be three times of the minute ventilation to prevent CO2 accumulation.

49
O 2 tents For children – not tolerating mask / catheter Large capacity system Upto 50% O 2 concentration Flush tent with high flow of oxygen and maintain @8-10 lit/min. Large tent cap. and leak port – limited CO 2 build up. Disadvantage –Limited access –Risk of fire –Conflict in O 2 therapy / nursing care

50
Bag – Valve – Mask assembly (Ambu Resuscitator) Delivers O 2 during BOTH spont. & artf. Vent O 2 concentration –30 – 50% (without reservoir) –80 – 100% (with reservoir) To deliver 100% O 2 –Reservoir – as large as bag vol –O 2 flow rate > minute volume (10 l/m) Drawback – keeps rescuer’s hands engaged
 –80 – 100% (with reservoir) To deliver 100% O 2 –Reservoir – as large as bag vol –O 2 flow rate > minute volume (10 l/m) Drawback – keeps rescuer’s hands engaged.")
51
HELIOX Helium 79% with 21% oxygen Low density helium decreases turbulence at narrow airway and also reduces pressure drop turbulent flow depends proportionally to pressure drop, density,velocity Useful in croup, tracheal stenosis, laryngeal, tracheal tumors (large airway obstruction)
")
52
Extra-corporeal membrane oxygenation ECMO which is Extra-corporeal membrane oxygenation, is a temporary life support system used for patients who have failed traditional mechanical ventilation.

53
Used in severe lung injury where high PEEP or PIP causes further lung damage; eg: pneumonia,ARDS 2 techniques : veno-venous blood (central venous circ – oxygenator –right atrium) lung not bypassed, ventilated to maintain ABG. veno-arterial : central venous circ – oxygenator – systemic circulation lung completely rested,or static inflation

54
INTRAVASCULAR OXYGENATION IVOX : long bundle of hollow microporous polypropylene fibres with double lumen gas tube for passing oxygen. Placed in IVC thru femoral vein Gas exchange depends on pr. Gradient 40 – 70 ml/min O2 and CO2 In ARDS, helps to reduce the intensity of lung ventilation. DISADV : blood loss, thrombotic event, infection, dec. venous return, vasc. injury

55
Hyperbaric oxygen Is a treatment in which a patient breathes 100% oxygen intermittently while pressure of the treatment chamber increased to a point higher than sea level pressure HBO was proved to cause hyperoxygenation of normal tissue and of tissue with poor blood perfusion by increasing the dissolved fraction of oxygen in plasma

56
At sea level the plasma oxygen concentration is 3 ml/l. At a pressure of 3 atmospheres dissolved oxygen approaches 54 ml/l of plasma, which is almost sufficient to supply the resting total oxygen requirement of many tissues without a contribution from oxygen bound to haemoglobin.

57
Approved Indications for HBO2 Air or gas embolism Carbon monoxide poisoning and smoke inhalation, carbon monoxide complicated with cyanide poisoning Clostridial myonecrosis (gas gangrene) Crush injuries, compartment syndrome and other acute traumatic ischemias Decompressed sickness Enhancement of healing in selected problem wounds Anaemia Necrotizing soft tissue infections Osteomyelitis (refractory) Osteoradionecrosis (ORN),soft tissue radionecrosis,radiation tissue damage Skin grafts and flaps failure Thermal burns
 Crush injuries, compartment syndrome and other acute traumatic ischemias Decompressed sickness Enhancement of healing in selected problem wounds Anaemia Necrotizing soft tissue infections Osteomyelitis (refractory) Osteoradionecrosis (ORN),soft tissue radionecrosis,radiation tissue damage Skin grafts and flaps failure Thermal burns")
58
Cellular and biochemical benefits of hyperbaric oxygen - Promotes angiogenesis, fibroblast activation and wound healing - Kills certain anaerobes - Prevents growth of species such as Pseudomonas - Prevents production of clostridial alpha toxin - Causes up regulation of growth factors, down regulation of inflammatory cytokines - Restores neutrophil mediated bacterial killing in previously hypoxic tissues

59
Method of administration Monoplace chamber (accomodates only a single person and pressurized to about 2-2.5 ATA with 100% oxygen Multiplace chamber (can accommodate several patients and/or health care peronnel, patients breath 100% oxygen through head tent, face mask or endotracheal tube. In either case the arterial PO2 will approach 1500 mm Hg (Normal = 90-95 mm Hg).
..")
60
Role in CO poisoning CO is colorless odorless and tasteless. Compete with oxygen for hemoglobin and form COHb. Level of COHb does not correlate severity of poisoning. Interfere with oxygen delivery and utilization by shifting ODC to left and inhibiting cytochrome oxidase respectively.

61
CO elimination is based on FiO2 Individual metabolism Duration of exposure Minute ventilation

62
Half life of COHb Breathing room air- 4-6 hrs Normobaric 100% O2 40-80min Hyperbaric O2 @ 2.8 ATA 15-30 min

63
HAZARDS OF OXYGEN THERAPY Retinopathy of Prematurity (neonates) – PaO2 > 80 – 100 torr – opaque, fibrotic tissue forms behind lens of eye – retina detachment; blindness
 – PaO2 > 80 – 100 torr – opaque, fibrotic tissue forms behind lens of eye – retina detachment; blindness")
64
Oxygen-induced hypoventilation – seen in patients with chronic hypercapnia – knocks out “hypoxic drive” – Intermittent use may, in some patients, cause PaO2 to drop < pre-Rx levels

65
Absorption Atelectasis – N2 comprises 78% of air,maintains alveolar stability – Poorly ventilated alveoli lose oxygen to blood faster than it can be replenished – Alveoli decrease in size; collapse – True shunt; hypoxemia increases

66
Complications of HBO2 Therapy Confinement anxiety Barotraumas Increased gas density leading to turbulent flow and increased heat loss. Oxygen toxicity Reversible myopia Decompression sickness Fire hazards

67
Oxygen Toxicity CNS -Oxygen toxicity seizures Lung -Pulmonary Oxygen Toxicity Eye -Refractory changes (transient)
")
68
CNS Oxygen Toxicity Signs and Symptoms: Convulsion, nausea,dizziness, hiccups, muscle twitching, vision and hearing abnormalities, difficulty breathing, unusual fatigue, anxiety and confusion,dizziness » Time/Dose 2 ATA:4 hrs 3 ATA:2 hrs 4 ATA:15 min 5 ATA:5 min

69
Visual Effects of Oxygen Toxicity Refractive Index changes in patients greater than 40 years old following 2-3 weeks HBO treatment. Transient effect. Cataracts may worsen.

70
Barotrauma Middle Ear Paranasal Sinus Gastrointestinal Tract Lungs Pneumothorax

71
Take home message O2 is a drug commonly prescribed by medical and paramedical staff. It is life saving when correctly administered but it has known side effects. It should be administered in proper dose for a clear indication by a proper delivery system for a duration of time required along with vigilant monitoring.

72
Thank you www.anaesthesia.co.inwww.anaesthesia.co.in anaesthesia.co.in@gmail.comanaesthesia.co.in@gmail.com

Similar presentations










 & CARBONDIOXIDE(CO2)>")












