Download presentation
Presentation is loading. Please wait.

1
Dr Mohammad Sadrkabir

2
The American Journal of GASTROENTEROLOGY 2011

3
INTRODUCTION 40–100% of adults exhibiting stigmata of past infection. CMV persists in a latent form throughout the lifetime of the infected subject and viral replication can be reactivated in situations of immunosuppression. Conversely, CMV has been implicated in exacerbation of IBD, but its role remains unclear. Retrospective studies reported the presence of CMV in the surgical specimens of patients with ulcerative colitis (UC) who underwent colectomy because of toxic megacolon or steroid resistance. The treatment of CMV infection by ganciclovir improves the clinical outcome of patients, suggesting that CMV infection may influence the evolution of UC by triggering acute flare-ups.
 who underwent colectomy because of toxic megacolon or steroid resistance. The treatment of CMV infection by ganciclovir improves the clinical outcome of patients, suggesting that CMV infection may influence the evolution of UC by triggering acute flare-ups..")
4
Because of the small sample size of the studies and the diversity of situations, no definite conclusions can be drawn from the available data. Another source of bias is the variety of techniques used to characterize CMV infection or disease in these studies. Although histological examination, together with detection of CMV in blood or biopsies, is now recommended, the clinical implications of the detection of CMV genome in bowel tissue are still debated.

5
In this study, the CMV DNA load was quantified by real-time polymerase chain reaction (PCR) in biopsy samples of UC patients before the instauration of immunosuppressive therapies. The results were compared with endoscopic and histological findings. Thresholds were defined that could predict resistance to different immunosuppressive regimens in UC.

6
METHODS From January to November 2009, a single-center, prospective, observational study was carried out in 42 adult patients exhibiting moderate to severe acute flare-ups of UC. The clinical activity was assessed by the Lichtiger score: moderate and severe colitis were defined by a score between 7 and 10, and >10, respectively. At inclusion, the patients could receive azathioprine (AZA) or purinethol at stable doses for 3 months, and mesalamine for 1 month. For the 15 patients receiving AZA at inclusion, the rate of 6- thioguanine nucleotide, a marker of treatment efficacy, was above 250 pmol/8×10 8 erythrocytes.
 or purinethol at stable doses for 3 months, and mesalamine for 1 month. For the 15 patients receiving AZA at inclusion, the rate of 6- thioguanine nucleotide, a marker of treatment efficacy, was above 250 pmol/8×10 8 erythrocytes..")
7
Exclusion criteria were as follows: (i) patients who received oral corticosteroids (CS) for >7 days or intravenous (IV) CS before hospitalization; (ii) patients treated by cyclosporine (CsY), methotrexate, infliximab (IFX), or adalimumab; (iii) pregnant women; (iv) patients under 18 or over 75 years of age; (v) patients participating in other clinical or therapeutic trials; (vi) patients exhibiting immunodeficiency (HIV infection, hypogammaglobulinemia, severe malnutrition, etc.); (vii) patients with proctitis; (viii) patients presenting Clostridium difficile infection in stool culture.
 patients who received oral corticosteroids (CS) for >7 days or intravenous (IV) CS before hospitalization; (ii) patients treated by cyclosporine (CsY), methotrexate, infliximab (IFX), or adalimumab; (iii) pregnant women; (iv) patients under 18 or over 75 years of age; (v) patients participating in other clinical or therapeutic trials; (vi) patients exhibiting immunodeficiency (HIV infection, hypogammaglobulinemia, severe malnutrition, etc.); (vii) patients with proctitis; (viii) patients presenting Clostridium difficile infection in stool culture.")
8
General procedures at inclusion All included patients underwent colonoscopy or flexible sigmoidoscopy <24 h after inclusion. The endoscopic score was assessed by a single experienced clinician.A severe colitis was defined by a Mayo score of 3. Endoscopic signs of severe disease (mucosal detachments, deep ulcerations) were recorded. Routine virological studies included the detection of IgM and IgG antibodies to CMV and the measure of CMV DNA load in whole blood using the CMV R-gene kit.
 were recorded. Routine virological studies included the detection of IgM and IgG antibodies to CMV and the measure of CMV DNA load in whole blood using the CMV R-gene kit..")
9
Analyses performed on intestinal biopsy samples Tissues from the mucosal lesions were sampled during endoscopy. A single pathologist screened the biopsies for the presence of inclusion bodies using hematoxylin and eosin staining and for markers of CMV infection by immunohistochemistry (IHC) using anti-CMV monoclonal antibodies (Argene). The quantitative determination of CMV DNA was performed by real-time PCR on frozen biopsy sample fragments using the CMV R-gene kit (Argene).
 using anti-CMV monoclonal antibodies (Argene). The quantitative determination of CMV DNA was performed by real-time PCR on frozen biopsy sample fragments using the CMV R-gene kit (Argene)..")
10
Therapeutic strategies and clinical follow-up All patients first received IV CS at a dose of 1 mg/kg for 7 days. CS resistance at D7 was then defined by the persistence of a Lichtiger score above 7 days for moderate UC and Lichtiger Index score ≥10 and/or a decrease <3 points of this index score compared with inclusion values for severe UC. A therapy with IV CsY A at a dose of 2 mg/kg/d for 7 days was initiated in those patients naive to AZA; patients already treated with AZA received an infusion of IFX at a dose of 5 mg/kg/d at weeks 0, 2, and 6. If no clinical remission was observed at the end of this second line of treatment, one therapy was switched to the other.

11
Other than patients having received AZA before steroid treatment,those presenting a contraindication for CsY, and in whom the Lichtiger score was still >10 under IFX (5 mg/kg by infusion), the IFX dose was increased to 10 mg/kg (IFX2). An emergency colectomy was undertaken following the occurrence of a complication (colectasia, hemorrhage, perforation) or in case of failure of the immunomodulatory treatment. During the follow-up of patients found positive for CMV infection, a second endoscopy was performed to analyze the evolution of the Mayo endoscopic score and (for 15 of them) to document the histological score and the CMV DNA load in the intestinal biopsy samples.
 or in case of failure of the immunomodulatory treatment. During the follow-up of patients found positive for CMV infection, a second endoscopy was performed to analyze the evolution of the Mayo endoscopic score and (for 15 of them) to document the histological score and the CMV DNA load in the intestinal biopsy samples..")
12
RESULTS

13
From a total of 42 patients enrolled in the study, 15 were under AZA treatment at the time of inclusion and 22 were under mesalazine treatment. The mean number of previous flare-ups of UC was 3 (0–6) and 35 patients had received CS during the previous 2 years. The Mayo score corresponded to stages 2 and 3 in 20 and 22 cases, respectively. In 10 of them, the endoscopic examination identified severe lesions, including deep ulcers and mucosal detachment.
 and 35 patients had received CS during the previous 2 years. The Mayo score corresponded to stages 2 and 3 in 20 and 22 cases, respectively. In 10 of them, the endoscopic examination identified severe lesions, including deep ulcers and mucosal detachment..")
14
Markers of CMV infection at baseline IgG antibodies to CMV were present in 25 of 42 patients (59.5%). CMV DNA at the rate of 10 copies/mg was detected in inflamed tissue of 16 patients (38.0%), 8 with a histological score of 2 and 8 with a score of 3. Biopsy specimens sampled in endoscopically normal regions were available for 18 patients; none of them was found to be positive for CMV DNA, including those (n=8) with a positive signal in inflamed tissue. All the patients with CMV DNA in inflamed tissue were seropositive for CMV (IgG, not IgM). Histological markers of CMV infection, analyzed by both hematoxylin and eosin staining and IHC, were detected in none of the biopsy samples from the 42 patients. CMV DNA was detectable in the blood of only three patients.
, 8 with a histological score of 2 and 8 with a score of 3. Biopsy specimens sampled in endoscopically normal regions were available for 18 patients; none of them was found to be positive for CMV DNA, including those (n=8) with a positive signal in inflamed tissue. All the patients with CMV DNA in inflamed tissue were seropositive for CMV (IgG, not IgM). Histological markers of CMV infection, analyzed by both hematoxylin and eosin staining and IHC, were detected in none of the biopsy samples from the 42 patients. CMV DNA was detectable in the blood of only three patients..")
15
Therapeutic evolution : 26 patients without colonic CMV DNA

16
16 patients with colonic CMV DNA

17
All 26 patients with a colonic CMV DNA load under 10 copies/mg responded favorably to one to three lines of treatment. By contrast, in the group of 16 patients positive for colonic CMV DNA: only six (37.5%) responded spontaneously to the successive lines of immunosuppressive treatment; two required an emergency colectomy, the other eight were treated with ganciclovir
 responded spontaneously to the successive lines of immunosuppressive treatment; two required an emergency colectomy, the other eight were treated with ganciclovir.")
18
In the latter group of seven patients, five (two with CMV DNA >250 copies/mg and the remaining three with between 10 and 250 copies/mg) were resistant to CS but responded to IFX treatment (+CsY in one case). The CMV DNA load was found to be stable in four cases and under the rate of 10 copies/mg of tissue in the last one. Interestingly, all these patients responded spontaneously to treatment.

19
By contrast, the two remaining patients exhibited high CMV load (>250 copies/mg) in the first biopsy and were resistant to three lines of treatment: one of them required an emergency colectomy and the other a colectomy 2 months later. The only patient for whom the initially positive intestinal viral load was not controlled had an initial DNA load between 10 and 250 copies/mg; this patient responded spontaneously to CsY treatment.

20
Determination of factors associated with CMV detection in intestinal tissue Four factors were evaluated : clinical activity, phenotype, previous treatment by AZA, and resistance to steroids or to three lines of treatment. The sole factor that remained in the model after multivariate analysis was the resistance to steroids or to three lines of treatment (risk ratio: 4.7; 95% confidence interval: 1.2–22.5; P<0.05).
..")
21
The relationship between colonic viral load and response to immunosuppressive therapy A viral load of >250 copies/mg of tissue was predictive of a resistance to three successive lines of treatment with a sensitivity of 100% and a specificity of 66.6% (LR+=4.33; AUROC=0.85; P<0.05). The absence of CMV DNA in tissue was predictive of a favorable response to any treatment with a sensitivity of 100% and a specificity of 50% (LR+=2.21; AUROC=0.65; P<0.05).
..")
22
To complete these findings, four groups of therapeutic outcome were defined: favorable response to steroids (n=10), resistance to steroids but response to the first line of immunomodulatory therapy (n=12), resistance to steroids and to the first line of immunomodulatory therapy (n=12), resistance to steroids and to two lines of immunomodulatory therapy (n=8).
, resistance to steroids but response to the first line of immunomodulatory therapy (n=12), resistance to steroids and to the first line of immunomodulatory therapy (n=12), resistance to steroids and to two lines of immunomodulatory therapy (n=8).")
24
Correlation between the presence of CMV DNA in tissue and the endoscopic and histologic scores No statistically significant correlation was observed between the detection of CMV DNA in bowel tissue and the Mayo endoscopic score, the presence of markers of tissue injury (deep ulcerations lesions, mucosal detachments), the histological score depicted by lymphocyte infiltration, or the presence of intracryptic abscesses.
, the histological score depicted by lymphocyte infiltration, or the presence of intracryptic abscesses.")
25
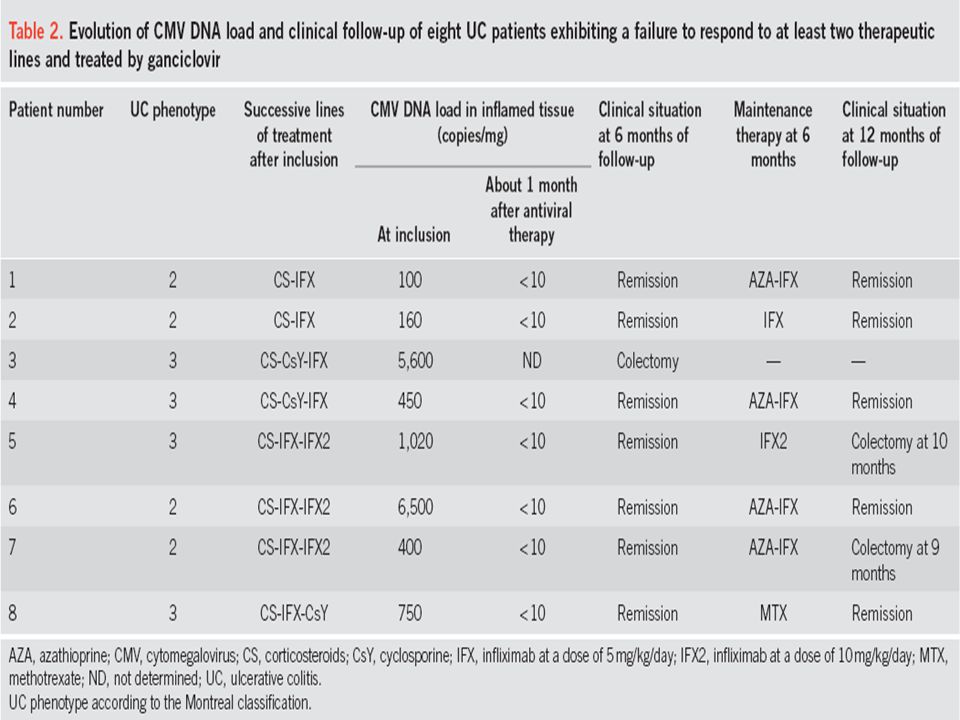
Evolution of the eight patients treated by ganciclovir Eight patients who were found to be positive for colonic CMV DNA, and who failed to respond to at least two lines of treatment, were treated with ganciclovir infusions (5 mg/kg twice a day for 10 days) followed by valganciclovir 900 mg/d for 15 days, in addition to their ongoing immunosuppressive therapy.
 followed by valganciclovir 900 mg/d for 15 days, in addition to their ongoing immunosuppressive therapy.")
27
Patient 3 in exhibited no clinical remission despite the antiviral treatment, and underwent an emergency colectomy. For the seven other patients (87.5%), no CMV DNA was found in the biopsy specimens obtained 30±5 days after the beginning of antiviral treatment, and a clinical remission was obtained with a sustained response to the last therapeutic line after a follow-up of 6 months. For all of these seven patients, a step-down therapeutic strategy of treatment was undertaken at 1 month with notably the replacement of steroids by a 2-month regimen of CsY followed by AZA alone. two of these patients relapsed at 9 and 10 months (Lichtiger score of 7 and 8, respectively) and justified a delayed colectomy.
, no CMV DNA was found in the biopsy specimens obtained 30±5 days after the beginning of antiviral treatment, and a clinical remission was obtained with a sustained response to the last therapeutic line after a follow-up of 6 months. For all of these seven patients, a step-down therapeutic strategy of treatment was undertaken at 1 month with notably the replacement of steroids by a 2-month regimen of CsY followed by AZA alone. two of these patients relapsed at 9 and 10 months (Lichtiger score of 7 and 8, respectively) and justified a delayed colectomy..")
28
DISCUSSION Several studies have investigated the role of CMV infection in the exacerbation of IBD. However, the definitions used for CMV infection were heterogeneous and there were several methodological limitations (small sample size, no determination of viral load in tissue, no use of validated definition of clinical response or relapse), leading to discrepant results and precluding definitive conclusions regarding the potential contribution of CMV to exacerbation of IBD. Quantification of CMV load in inflamed tissue has been rarely used for the diagnosis of CMV infection in IBD patients, even if the use of tissue PCR is recommended as an alternative to IHC by European Crohn's and Colitis Organization guidelines for the investigation of CMV infection in immunomodulatory refractory cases of IBD.
, leading to discrepant results and precluding definitive conclusions regarding the potential contribution of CMV to exacerbation of IBD. Quantification of CMV load in inflamed tissue has been rarely used for the diagnosis of CMV infection in IBD patients, even if the use of tissue PCR is recommended as an alternative to IHC by European Crohn s and Colitis Organization guidelines for the investigation of CMV infection in immunomodulatory refractory cases of IBD..")
29
By using DNA quantification of CMV at a threshold of 10 copies/mg, stigmata of CMV infection were observed in the inflamed intestinal tissue from 38.0% of the UC patients included in this study but never in their endoscopically normal tissue. Interestingly, this finding was associated neither with markers of CMV infection in blood nor with histological markers of CMV disease in colonic tissue, even when the CMV DNA load was high at the tissue level. Similar discrepancies were observed in three other studies using molecular markers of CMV at the tissue level. For instance, Yoshino et al. detected CMV DNA in the colonic tissue of 60% of their patients, whereas only 6% of them exhibited positive IHC markers.

30
It is important to recall that the patients included in our study were all naive of IV steroid or CsY treatment, which are known to induce severe CMV reactivation with histological lesions.

31
We found that a CMV viral load >250 copies/mg of tissue was associated with resistance to three successive therapeutic lines, with a sensitivity of 100% and a specificity of 66.6% (AUROC=0.85). When a second biopsy sample was available and the patient received no antiviral treatment, the CMV DNA load was almost stable or increased in the inflamed tissue. This is the first time that a biomarker has been found to be able to predict the failure of immunosuppressive therapy in UC with a high predictive value.

32
One could wonder why four patients, despite a positive initial viral load in the colon, responded to IFX treatment. Similar findings were observed in two patients from another study who exhibited clinical remission despite the persistence of CMV DNA in the colon. It is interesting to note that three of our patients had a low viral load (<250 copies/mg) that probably contributed to the success of the therapy. In addition, it will be interesting to follow the evolution of these patients in order to verify whether they are more prone to exhibit a relapse of their colitis.
 that probably contributed to the success of the therapy. In addition, it will be interesting to follow the evolution of these patients in order to verify whether they are more prone to exhibit a relapse of their colitis..")
33
In this study, eight patients received ganciclovir therapy, leading to the clearance of CMV DNA in the tissue of seven of them. Of importance, in our study, seven of eight patients who responded to antiviral treatment were then treated successfully with immunomodulatory drugs, with no relapse for a follow-up of 6 months. Similarly, in the study of Yoshino et al. 10 of 12 patients who were positive for CMV DNA in colon and who were treated with antiviral drugs went into remission.

34
In accordance with the findings of Yoshino et al. no trace of CMV DNA was detected in the endoscopically normal tissue of eight patients exhibiting CMV DNA in inflamed tissue. Proinflammatory cytokines such as interferon-γ and tumor necrosis factor-α can promote the migration of monocytes to the inflammatory sites of the colon mucosa ; these cells, which are able to differentiate to macrophages in tissue, represent the natural reservoir of CMV. Therefore, CMV reactivation could occur in inflamed tissue but not in healthy mucosa.

35
Conclusion During severe flare-ups of UC, the CMV DNA load in inflamed tissue may be predictive of the occurrence of future resistance to IV steroids or several drug regimens. Determination of CMV load in inflamed tissue, which can be available within 24 h after biopsy sampling, appears to be critical to determine which patients would benefit by initiating antiviral treatment in order to prevent therapeutic resistance to immunomodulatory drugs. These results need to be evaluated further in large independent studies.

36
با تشکر از توجه شما

Similar presentations
















 1 Concordance of HER2 Central Assessment.>")
 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")


