Download presentation
Presentation is loading. Please wait.

1
Update on the Medical Treatment of Crohn’s Disease Dahlia Awais, MD, MS Division of Gastroenterology University Hospitals Case Medical Center

2
Outline of Topics IBD background –UC vs Crohn’s –Pathogenesis Treatment –Risks/Benefits Current Questions –Evolving goals and treatment paradigms Future Directions

3
Inflammatory Bowel Disease IBD – chronic intestinal inflammation Ulcerative Colitis Crohn’s Disease

4
Ulcerative Colitis

7
Crohn’s Disease

11
Crohn’s Symptoms Active Crohn’s –Chronic or nocturnal diarrhea –Rectal bleeding –Abdominal pain –Weight loss –Fever –Fatigue –Extraintestinal Manifestations Skin/eyes/joints

12
Crohn’s Disease Characterized by flares alternating with remission –<20% unremitting –10% prolonged remission More than 80% lifetime risk of surgery Vermeire et al APT 2007; 25:3-12 Peyrin-Biroulet et al AJG 2010; 105: 289-297

13
Risk for 1 st Surgery Dhillon et al. AJG 2005; 100: S305

14
Crohn’s Disease Previous disease activity predicts future disease activity –Full year of remission followed by 80% chance of remission in following year –Disease flare followed by 30% chance of remission in the following year Vermeire et al APT 2007; 25:3-12

15
IBD Treatment Goals c. 2011 Induce and maintain response/remission Prevent complications –Disease related –Therapy related Improve/maintain quality of life Limit surgery ?Mucosal healing

16
Principles of Treatment Treatment of active disease followed by maintenance of remission One size does not fit all Risks vs benefits

17
Treatment Overview Induction –Sulfasalazine –Mesalamine –Steroids –Azathioprine/6-MP –Methotrexate –Biologics Maintenance –Sulfasalazine –Mesalamine –Azathioprine/6-MP –Methotrexate –Biologics

18
Case Presentation 1 22 yo M –4 week history bloody diarrhea (3-4/day) –Mild abdominal pain Colonoscopy and biopsies –Mild Crohn’s colitis Recommend oral 5-ASA
 –Mild abdominal pain Colonoscopy and biopsies –Mild Crohn’s colitis Recommend oral 5-ASA")
19
Anti-Inflammatory Drugs 5-aminosalicylate (5-ASA) –Sulfasalazine –Mesalamine
 –Sulfasalazine –Mesalamine")
20
5-ASA Sulfasalazine –3-6 g/day –Better than placebo ~43% remission rates compared w/ placebo 30% –Not consistently effective for sb disease Mesalamine –Some trials have shown benefit up to 40-55% remission –Meta-analysis 3 placebo controlled multi-center trials Mesalamine 4g/day Statistically significant but not clinically significant difference –2005 Cochrane analysis maintenance No different than placebo –Widely used in clinical practice Efficacy not clearly demonstrated in trials Summers et al Gastro 1979; 77: 847-869 Lichtenstein et al AJG 2009; 104: 465-483 Akobeng et al Cochrane Database of Systematic Reviews 2009 Hanauer et al CGH 2004; 2: 379-88

21
5-ASA Risks Sulfasalazine –Headache –Nausea/vomiting –Rash –Folate malabsorption –Reversible oligospermia –Pancreatitis –Bone marrow suppression –Paradoxical exacerbation –Interstitial nephritis Mesalamine –Headache –Nausea –Rash –Pancreatitis –Paradoxical exacerbation –Interstial nephritis

22
Interstitial Nephritis Medicolegal Case reports (rare) –First report 1989 –UK GPRD 130 of 19,020 5-ASA users w/ IBD 0.17 cases per 100 patients per year Ref cohort.08 cases per 100 patients per year Idiosyncratic (mechanism unknown) Inform patient prior to starting “Monitoring” recommended package insert –Cr –?effective, ?cost-effective Gisbert et al IBD 2007; 13: 629-38 Van Staa et al Gastroenterology 2004; 126: 1733-9
 –First report 1989 –UK GPRD 130 of 19,020 5-ASA users w/ IBD 0.17 cases per 100 patients per year Ref cohort.08 cases per 100 patients per year Idiosyncratic (mechanism unknown) Inform patient prior to starting Monitoring recommended package insert –Cr – effective, cost-effective Gisbert et al IBD 2007; 13: Van Staa et al Gastroenterology 2004; 126:")
23
Case Presentation 2 33 yo M w/ 1 yr hx Crohn’s –Previously treated w/ steroids and mesalamine –Abdominal pain, diarrhea controlled on steroids Colonoscopy –Inflammation and ulcers in TI and colon –Biopsies c/w ileo-colonic Crohn’s MRI-e –No stricture/fistula/abscess Recommend azathioprine

24
Corticosteroids IV: hydrocortisone, methylprednisolone Oral: prednisolone, prednisone, budesonide Budesonide –Topically active glucocorticoid –Limited systemic bioavailability Less toxicity –Ileal and right sided colonic disease –Short term efficacy less than conventional steroids (~15%) –Best combination of short term efficacy and safety Seow et al Cochrane Database of Systematic Reviews 2005
 –Best combination of short term efficacy and safety Seow et al Cochrane Database of Systematic Reviews 2005")
25
Corticosteroids Very effective at inducing remission –30d pop based study Placebo controlled trials –50-70% remission over 8-17wks pred 40 Not for maintenance 58%26%16% Complete Remission Partial Response No Response Pred 40- 60 mg Faubion et al Gastro 2001; 121: 255-260 Lichtenstein et al AJG 2009; 104: 465-483 Steinhart et al Cochrane Database 2003

26
Corticosteroids Risks CataractsGlaucomaDiabetes Weight gain HypertensionOsteopenia/OsteoporosisAcne Mood/sleep disturbances Infection

27
Immunomodulator Drugs Azathioprine/6-MP

28
Azathioprine/6-MP Perfontaine et al,Cochrane Database of Systematic Reviews 2010 54 33 65 36

29
Azathioprine Risks BM – Leukopenia (2- 5%) Hepatotoxicity (rare) Pancreatitis (3%) Drug intolerance (10- 15%) –Fatigue –Nausea –Flu-like –Hypersensitivity rxn Infection (2-3:1) –Viral- HSV, CMV, EBV Lymphoma (~4x)
 Hepatotoxicity (rare) Pancreatitis (3%) Drug intolerance (10- 15%) –Fatigue –Nausea –Flu-like –Hypersensitivity rxn Infection (2-3:1) –Viral- HSV, CMV, EBV Lymphoma (~4x)")
30
Lymphoma Non-Hodgkins lymphoma –US annual incidence 2/10,000 –Lymphoma risk increases with age Number needed on Azathioprine to cause 1 add’l lymphoma/year –Age 20 : NNH ~4300 –Age 70: NNH ~350 Hepatosplenic T cell lymphoma –Young males –16 cases with 6MP/AZA alone –20 cases with 6MP/AZA + anti-TNF –>99.99% will not have this complication Kandiel et al Gut 2005; 54: 1121-5 Kotlyar et al AJG 2010; 105: 2299

31
Methotrexate Methotrexate –Well documented effectiveness in steroid dependent Crohn’s Induction: MTX 25mg IM/week x16wks –39% vs 19% (placebo) in clinical remission Maintenance: MTX 15 mg IM/week –65% vs 39% maintenance of steroid free remission at 40wks Feagan et al NEJM 1995 Feagan et al NEJM 2000
 in clinical remission Maintenance: MTX 15 mg IM/week –65% vs 39% maintenance of steroid free remission at 40wks Feagan et al NEJM 1995 Feagan et al NEJM 2000")
32
MTX Risks Methotrexate –Nausea –Fatigue/malaise –Hepatotoxicity Abnl LFT’s ~25% Fibrosis/cirrhosis rare –BM suppression –Hypersensitivity pneumonitis 1% of patients –Teratogen –Increased risk of infection –Lymphoma risk is rare

33
Case Presentation 3 26 yo F w/ 2 yr hx Crohn’s –Previously treated with steroids and AZA –Abdominal pain, diarrhea, perianal fistula Colonoscopy –Inflammation and ulcers in colon and TI MRI-e –No stricture, no abscess Recommend anti-TNF

34
Anti-TNF’s InfliximabAdalimumabCertolizumab ● FDA approved 1998 ● Mouse chimeric monoclonal Ab ● IV (0, 2, 6, then q8wk) ● 5 mg/kg ● FDA approved 2007 ● Fully human monoclonal Ab ● SQ q2wks (loading 4 pens, then 2 pens, then 1 pen) ● Each pen 40 mg ● FDA approved 2008 ● Pegylated humanized Fab fragment ● SQ (0, 2, 4, then q4wk) ● 400 mg
 ● 5 mg/kg ● FDA approved 2007 ● Fully human monoclonal Ab ● SQ q2wks (loading 4 pens, then 2 pens, then 1 pen) ● Each pen 40 mg ● FDA approved 2008 ● Pegylated humanized Fab fragment ● SQ (0, 2, 4, then q4wk) ● 400 mg")
35
Anti-TNF Therapies 58 39 21 ACCENT I Infliximab Wk 2 Response Wk 30 Remission Wk 30 Remission Placebo Patients % Wk 4 Response Wk 26 Remission Wk 26 Remission Placebo CHARM Adalimumab 40 17 58 Patients % 64 48 29 Wk 6 Response Wk 26 Remission Wk 26 Remission Placebo Precise 2 Certolizumab Hanauer et al Lancet 2002; 359:1541-49 Colombel et al Gastroenterology 2007; 132: 52-65 Schreiber et al NEJM 2007; 357: 239-50 Patients % P<.001 P<.003 P<.001

36
Benefits Steroid free remission Improved quality of life Decreased hospitalizations Decreased need for surgeries Improved mucosal healing Lichtenstein et al Gastroenterology 2005; 128: 862-9

37
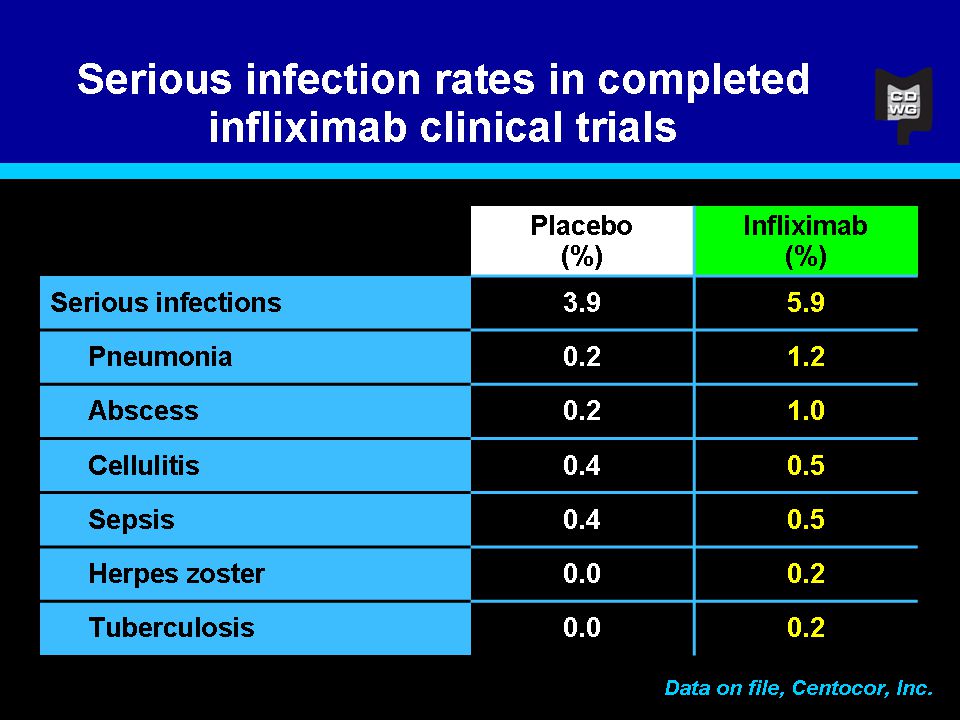
Risks of Anti-TNF’s Infusion Reaction (5%) Infection –Reactivation TB, HBV –Sepsis –OI’s Lymphoma Demyelinating d/o (rare) Hepatotoxicity (rare) Drug induced lupus (<1%)
 Infection –Reactivation TB, HBV –Sepsis –OI’s Lymphoma Demyelinating d/o (rare) Hepatotoxicity (rare) Drug induced lupus (<1%)")
39
Natalizumab Natalizumab is a fully humanized antibody against alpha- 4 integrin Prevents inflammatory white blood cells from migrating into tissue Can be used when patient has failed at least one anti- TNF medication Cannot be combined with other immunosuppressants –Must taper off steroids within 6 months Administered intravenously Given every 4 weeks Dose is 300 mg

40
Natalizumab Response Remission Patients % Targan et al Gastro 2007; 132: 1672- 83 48 32 26 16

41
Risks of Natalizumab Infection PML (1/1000) –Opportunistic, demyelinating brain d/o –Infection of oligodendrocytes by reactivation of JC virus –50% mortality; persistent neurologic damage –Dec 2010 79 cases/75,500 pts Most in MS
 –Opportunistic, demyelinating brain d/o –Infection of oligodendrocytes by reactivation of JC virus –50% mortality; persistent neurologic damage –Dec cases/75,500 pts Most in MS")
42
Historical Perspective Early 1900’s –“slop diets” –“vaccines” 1940 –Sulfasalazine –Penicillin 1950’s –ACTH 1960’s –6-MP 1970’s –Sulfa-free aminosalicylates 1998 –Infliximab –Beginning of the biologic era

43
Current Questions Step Up vs Top Down Mucosal Healing Combination vs Monotherapy

44
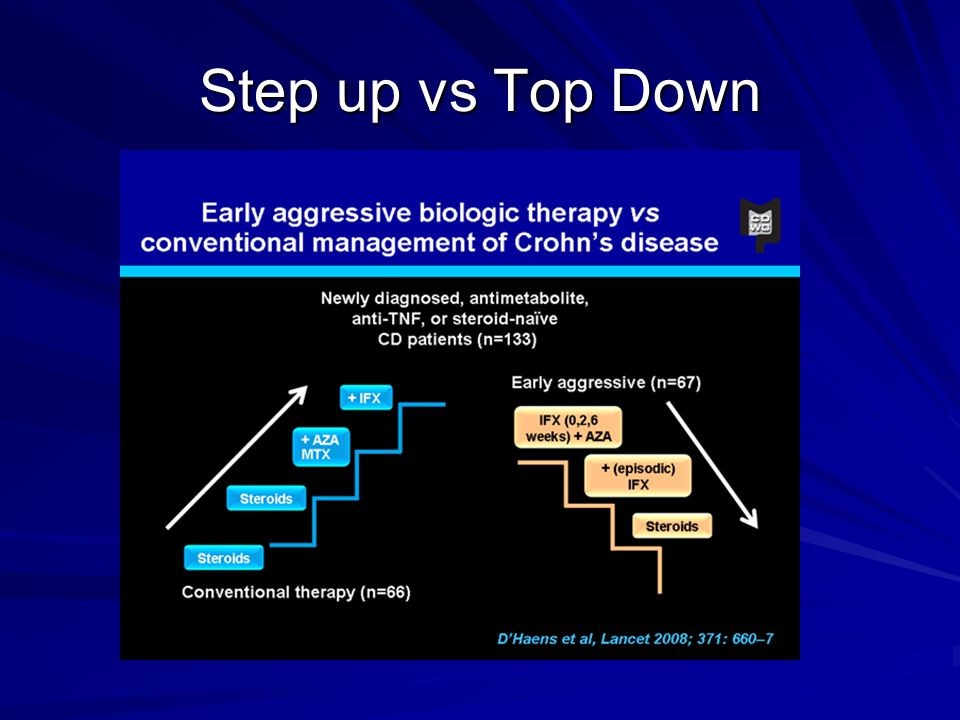
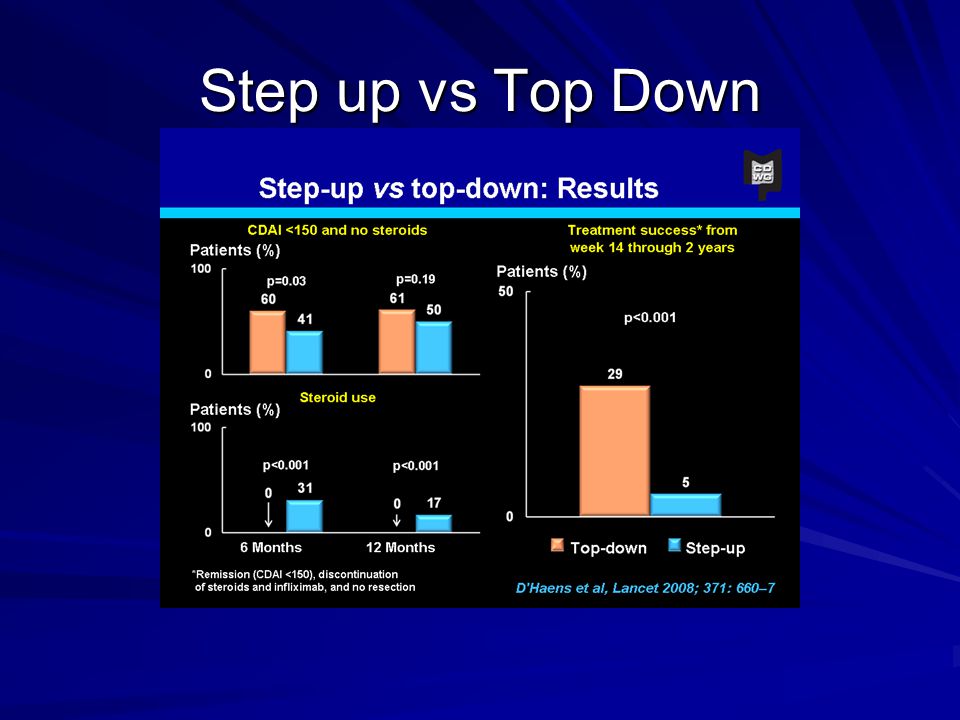
Step up vs Top Down

47
Mucosal Healing ACCENT I substudy –Mucosal healing associated with fewer Crohn’s related hospitalizations Rutgeerts et al GIE 2006; 63:433-42 75 0/9 (0) 3/16 (18.8) 14/50 (28) Healing at both visits Healing at 1 visit No healing Crohn’s Disease Related Hospitalizations
 3/16 (18.8) 14/50 (28) Healing at both visits Healing at 1 visit No healing Crohn’s Disease Related Hospitalizations")
48
Mucosal Healing Baert et al Gastro 2010; 138: 463-8

49
Combination vs Monotherapy Colombel et al NEJM 2010; 362: 1383-95 30 44.4 56.8 Patients % Steroid Free Clinical Remission at week 26

50
Future Goals Predict individual prognosis –Phenotype and risk assessment Treatment based on risk –More aggressive therapy to those with more aggressive

51
Future Directions Need for novel therapies Current biologic therapies have –Decreased hospitalizations and surgeries –Improved QoL But… –Up to one-third do not respond –Many lose response or develop intolerance Safety concerns –Opportunistic infections –Malignancy –PML (Natalizumab)
")
52
Future Directions Oral Less expensive New mechanisms of drug action

Similar presentations