Download presentation
Presentation is loading. Please wait.

1
ORAL ANTICOAGULANTS IN THE 21 ST CENTURY: A PRACTICAL GUIDE TO USING NEWER AGENTS Katherine Vogel Anderson, Pharm.D., BCACP University of Florida Colleges of Pharmacy and Medicine

2
Disclosures I have nothing to disclose

3
Case BV is a 75 year old white male who has just been diagnosed with a. fib. His past medical history is significant for hypertension (taking chlorthalidone) and seasonal allergies. Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin
 and seasonal allergies. Which oral anticoagulant do you recommend. A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin.")
4
Objectives Identify new oral anticoagulants (OACs) Determine the current place in therapy for OACs Review appropriate transitions between parenteral anticoagulants and OACs (and vice versa) Highlight pharmacotherapy scenarios when changing between OACs Identify OAC options peri-procedure
 Determine the current place in therapy for OACs Review appropriate transitions between parenteral anticoagulants and OACs (and vice versa) Highlight pharmacotherapy scenarios when changing between OACs Identify OAC options peri-procedure")
5
A History Lesson… 1930s heparin 1950s warfarin 1990s LMWH 2001 fondaparinux 2010 dabigatran 2011 rivaroxaban 2012 apixaban

6
2013… What do I choose? *All are FDA approved for stroke prevention secondary to a. fib

7
warfarin rivaroxaban and apixaban dabigatran

8
FDA-Approved Doses ApixabanDabigatranRivaroxabanWarfarin MechanismActivated factor Xa inhibitor Direct thrombin inhbitor Activated factor Xa inhibitor Vitamin K antagonist Dose for stroke prevention secondary to a. fib 5mg twice daily 150mg twice daily 20mg once daily Dosed to achieve an INR between 2 and 3 Renal dose adjustment 2.5mg twice daily 75mg twice daily 15mg once daily Not required Also approved for VTE treatment and prevention

9
If it isn’t broken, why fix it? What’s wrong with warfarin? Monthly monitoring Drug interactions Takes lots of time… New OACs Don’t require monitoring Fewer interactions Quicker onset of action BUT new OACs… Lack antidotes Require renal adjustment Are expensive

10
RE-LY 18,113 patients enrolled, randomized to: dabigatran 150mg twice daily dabigatran 110mg twice daily warfarin, adjusted to an INR between 2 and 3 Atrial fibrillation + one risk factor Primary outcome: Stroke or systemic embolism Connolly SJ et al. NEJM 2009;361: 1139-1151

11
RE-LY Stroke or systemic embolism: 182 patients taking 110mg 134 patients taking 150mg 199 patients taking warfarin 150mg superior, but with same bleeding as warfarin 110mg noninferior, but with less bleeding than warfarin 110mg not approved by FDA Connolly SJ et al. NEJM 2009;361: 1139-1151

12
AVERROES 5599 patients randomized to: apixaban 5mg twice daily OR apixaban 2.5mg twice daily if 80 years old or older, 60Kg or less, and/or SCr > 1.5mg/dL aspirin 81mg – 324mg once daily Atrial fibrillation + one risk factor Patients who were not candidates for warfarin Previous vitamin K antagonist (VKA) was “unsuitable” VKA is expected to be “unsuitable” Connolly SJ et al. NEJM 2011;364: 806-817

13
AVERROES Stroke: 52 taking apixaban 113 taking aspirin Bleeding: 44 major bleeds, apixaban 39 major bleeds, aspirin Connolly SJ et al. NEJM 2011;364: 806-817

14
Wait… Aspirin? CHADS 2 = 0 aspirin is an option CHADS 2 = 1 or higher anticoagulation therapy is preferred Back to BV… 65 year old male with a history of hypertension, diabetes, and seasonal allergies. BV’s CHADS 2 score is 2 You JJ et al. Chest 2012;141(2)(Suppl): e531S-e575S
(Suppl): e531S-e575S.")
15
ARISTOTLE 18,201 patients randomized to: apixaban 5mg twice daily OR apixaban 2.5mg twice daily warfarin, adjusted to an INR between 2 and 3 Atrial fibrillation + one risk factor Primary outcome: ischemic or hemorrhagic stroke, or systemic embolism Granger CB et al. NEJM 2011;365: 981-992

16
ARISTOTLE Stroke: 212 taking apixaban 265 taking warfarin Granger CB et al. NEJM 2011;365: 981-992 Major bleeding: 327 taking apixaban 462 taking warfarin

17
ROCKET-AF 14,264 patients randomized to: rivaroxaban 20mg once daily OR rivaroxaban 15mg once daily for CrCL 30-49ml/min warfarin, adjusted to an INR between 2 and 3 Atrial fibrillation w/moderate-to-high risk of stroke Prior stroke, TIA, or systemic embolism OR two of: CHF, HTN, age 75 and older, DM Patel MR et al. NEJM 2011;365: 883-891

18
ROCKET-AF Stroke or systemic embolism: 188 taking rivaroxaban 241 taking warfarin Bleeding events: Rivaroxaban caused numerically more major and non-major bleeds BUT, there were less fatal bleeds with rivaroxaban Granger CB et al. NEJM 2011;365: 981-992

19
In a nutshell… Katsnelson M et al. Circulation 2012;125: 1577-1583

20
A wise man once said… “Inferiors revolt in order that they may be equal, and equals that they may be superior. Such is the state of mind, which creates revolutions.” —Aristotle. In: Politics. Book V; Part II; 350 B.C.E. anticoagulation Nedeltchev K. Stroke 2012;43: 922-923

21
Back to our case… Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin

22
Warfarin Pharmacogenomic dosing? Regardless – treat to an INR between 2 and 3 You JJ et al. Chest 2012;141(2)(Suppl): e531S-e575S Coumadin (warfarin) package insert. Princeton, NJ: Bristol-Myers Squibb Company; 2011 Oct.
(Suppl): e531S-e575S Coumadin (warfarin) package insert. Princeton, NJ: Bristol-Myers Squibb Company; 2011 Oct..")
23
But… Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin

24
Prodrug?Yes Food?No effect Drug interactionsP-gp substrate: Verapamil decrease dabigatran dose Dronedarone decrease/don’t use Renal adjustment CrCL < 30ml/min 75mg twice daily Pros the oldest of the new Cons GI intolerance; renal dose not prospectively studied Heidbuchel H et al. Europace 2013;15: 625-651

25
But… Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin

26
Prodrug?No Food?Mandatory Drug interactionsP-gp AND CYP3A4 substrate: Amiodarone, diltiazem, verapamil – caution if CrCL is less than 50ml/min AVOID with strong inhibitors Renal adjustment CrCL 15 – 50ml/min 15mg once daily Pros once daily dosing; renal adjustments Cons once daily dosing; food requirement Heidbuchel H et al. Europace 2013;15: 625-651

27
But… Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin

28
Pros renal dose prospectively studied Cons twice daily dosing; newest of the new Prodrug?No Food?No effect Drug interactionsCYP3A4 substrate: Reduce dose to 2.5mg/avoid with strong CYP3A4 and P-gp inhibitors Renal adjustmentIf SCr is greater than 1.5mg/dl, patient is greater than 80 years old, patient weighs less than 60Kg 2.5mg twice daily Heidbuchel H et al. Europace 2013;15: 625-651

29
Some considerations Although new OACs are substrates for P-gp and CYP, they are not inhibitors PPI use does not have a clinical effect on efficacy Bleeding risk increases with antiplatelet agents Compliance is key effectiveness fades fast 12 – 24 hours after last dose = no anticoagulation

30
The decision is made... … A new OAC will be prescribed for BV So – what’s next? Do we really NOT monitor? What if BV has a procedure? What if BV wants to switch to warfarin?

31
Let’s get started… Heidbuchel H et al. Europace 2013;15: 625-651

32
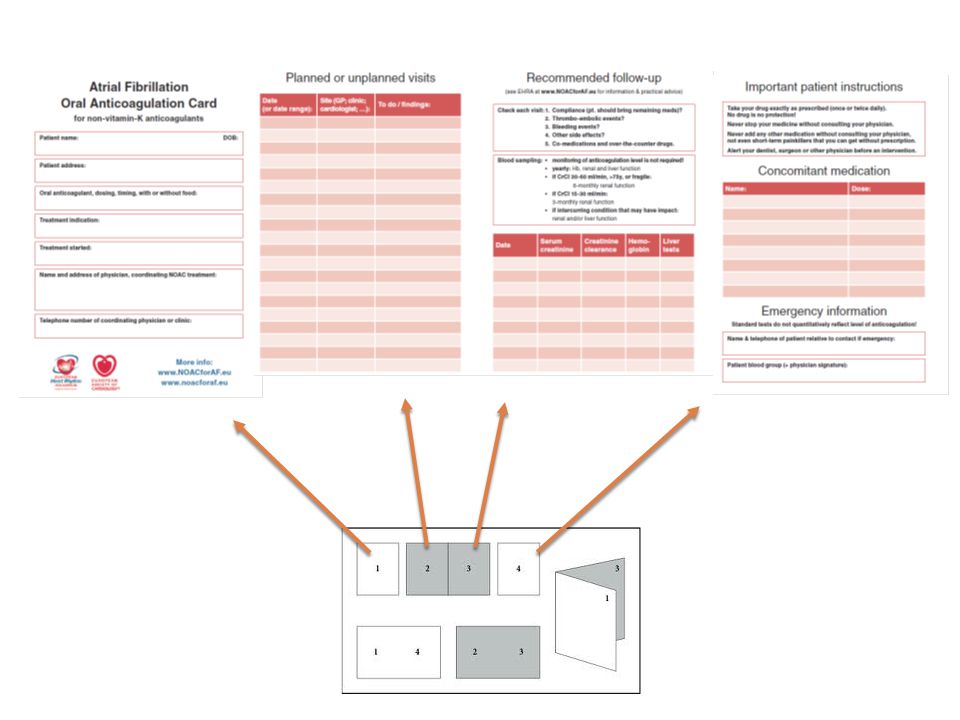
Patient anticoagulation cards: www.noacforaf.euwww.noacforaf.eu PPI: No prospective evidence, but consider a PPI for high risk patients (i.e. history of GI bleed) Follow up visits: Compliance S/Sx thromboembolism and/or bleeding Side effects Medication reconciliation Labs: 3, 6, 12 months and as needed Heidbuchel H et al. Europace 2013;15: 625-651
 Follow up visits: Compliance S/Sx thromboembolism and/or bleeding Side effects Medication reconciliation Labs: 3, 6, 12 months and as needed Heidbuchel H et al. Europace 2013;15:")
34
Coagulation Monitoring DabigatranApixabanRivaroxaban Plasma peak (after ingestion) 2 hours1 – 4 hours2 – 4 hours Plasma trough (after ingestion) 12 – 24 hours 16 – 24 hours PTN/A Prolonged INRIncrease aPTT>2xULN @ trough suggests risk N/A Anti-XaN/ANo data YETQuantitative ECT>3xULN @ trough suggests risk N/A Heidbuchel H et al. Europace 2013;15: 625-651

35
Transitions in Therapy To a new OAC… From heparin upon discontinuation (~2 hours) From low molecular weight heparin (LMWH) when the next dose of LMWH is due From a new OAC… To warfarin similar to “bridging” The new OAC is taken simultaneously with warfarin until the INR is within the appropriate therapeutic range To LMWH when the next dose of OAC is due Heidbuchel H et al. Europace 2013;15: 625-651

36
Transitions in Therapy From warfarin to a new OAC: As soon as the INR is less than 2 If INR is between 2 and 2.5 start the next day For INR greater than 2.5 It depends How high is the INR? Wait and hold Draw a new INR If INR is less than 2.5, proceed as above Heidbuchel H et al. Europace 2013;15: 625-651

37
Peri-procedural management of OAC Evaluate Patient factors = age, renal function, history of bleeding AND Procedure factors No bleeding risk Minor bleeding risk Major bleeding risk When do you stop the new OAC? No need to hold the OAC Heidbuchel H et al. Europace 2013;15: 625-651

38
Peri-procedural management of OAC Hold the OAC 24 hours prior Hold the OAC 48 hours prior Resume OAC 6 – 8 hours after the procedure IF immediate and complete hemostasis is achieved AND re-bleeding risk is minimal. If invasive procedure, resumption of OAC may be deferred for 48 - 72 hours Resume OAC 6 – 8 hours after the procedure IF immediate and complete hemostasis is achieved AND re-bleeding risk is minimal. If invasive procedure, resumption of OAC may be deferred for 48 - 72 hours Heidbuchel H et al. Europace 2013;15: 625-651

39
Management of bleeding Heidbuchel H et al. Europace 2013;15: 625-651

40
Two Clinical Questions What about aspirin? Post-ACS: ASA or clopidogrel + new OAC = increased bleeding apixaban or rivaroxaban may be preferred Within the first year ASA + decreased OAC dose After the first year OAC alone What about valves? NOT for valvular atrial fibrillation NOT for mechanical valve replacement Heidbuchel H et al. Europace 2013;15: 625-651

41
Back to our case… Which oral anticoagulant do you recommend? A. Apixaban B. Dabigatran C. Rivaroxaban D. Warfarin

42
My answer I’m old school… But, if pressed to choose a new one….

43
In closing… Identify new oral anticoagulants (OACs) Determine the current place in therapy for OACs Review appropriate transitions between parenteral anticoagulants and OACs (and vice versa) apixaban, dabigatran, rivaroxaban Stroke prevention secondary to AF IV PO: 2 hours after heparin, at next dose of LMWH PO IV: At time of next OAC dose
 Determine the current place in therapy for OACs Review appropriate transitions between parenteral anticoagulants and OACs (and vice versa) apixaban, dabigatran, rivaroxaban Stroke prevention secondary to AF IV PO: 2 hours after heparin, at next dose of LMWH PO IV: At time of next OAC dose")
44
In closing… Highlight pharmacotherapy scenarios when changing between OACs Identify OAC options peri-procedure New OAC to warfarin: bridge and check INR Warfarin to new OAC: INR should be less than 2.5 Consider patient factors AND procedure factors Resumption of OAC depends on hemostasis

45
Thanks for your attention!

Similar presentations








 Dabigatran and Rivaroxaban for the prevention of stroke and systemic embolism in nonvalvular atrial fibrillation Dr Dipti.>")











