Download presentation
Presentation is loading. Please wait.

1
Luigi Oltrona Visconti Divisione di Cardiologia IRCCS Fondazione Policlinico S. Matteo Pavia Sindromi coronariche acute nei pazienti con fibrillazione atriale : possiamo utilizzare in associazione NAO ed inibitori P 2 Y 12 ? Sindromi coronariche acute nei pazienti con fibrillazione atriale : possiamo utilizzare in associazione NAO ed inibitori P 2 Y 12 ? Heartline 2014 Genova 14 – 15 Novembre 2014 Heartline 2014 Genova 14 – 15 Novembre 2014

2
ACS Stented patients Coronary Ischemic events Stent thrombosis DAPT better than VKA 1 – 6 – 12 months AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration
 valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration")
3
ESC Guidelines DAPT ConditionDrugsDuration 1 year 1 month 6 months 1 year 1 month 6 months Recommandation / Evidence Level I A I A (B) I A I A (B) Year 2011 2012 2014 2011 2012 2014 VKA NOACS VKA NOACS Lifelong I A 2012 DAPT NSTEMI STEMI Elective BMS Elective DES NSTEMI STEMI Elective BMS Elective DES AF LOV 2014
 I A I A (B) Year VKA NOACS VKA NOACS Lifelong I A 2012 DAPT NSTEMI STEMI Elective BMS Elective DES NSTEMI STEMI Elective BMS Elective DES AF LOV 2014")
4
However …. Up to 30% of AF patients on VKA have CAD and are potential candidates to DAPT Between 5% to 10% of pts undergoing stent implantation necessitate anticoagulant treatment LOV 2014

5
What to do ? LOV 2014 Heartline 2014 Genova 14 – 15 Novembre 2014 Heartline 2014 Genova 14 – 15 Novembre 2014

6
VKA + antiplatelets Reduces the risk of thrombotic events but increases bleeding risk up to 3-5 fold Thrombotic riskHaemorragic risk

15
VKA + antiplatelets No definitive data are available LOV 2014 Heartline 2014 Genova 14 – 15 Novembre 2014 Heartline 2014 Genova 14 – 15 Novembre 2014

16
ISAR-TRIPLE 600 pts Indication to VKA+DES (ACS or elective) 9-month follow-up Composite endpoint : death, MI, stroke, ST, TIMI-bleeding (http://clinicaltrials.gov/show/NCT00776633)
 9-month follow-up Composite endpoint : death, MI, stroke, ST, TIMI-bleeding (")
17
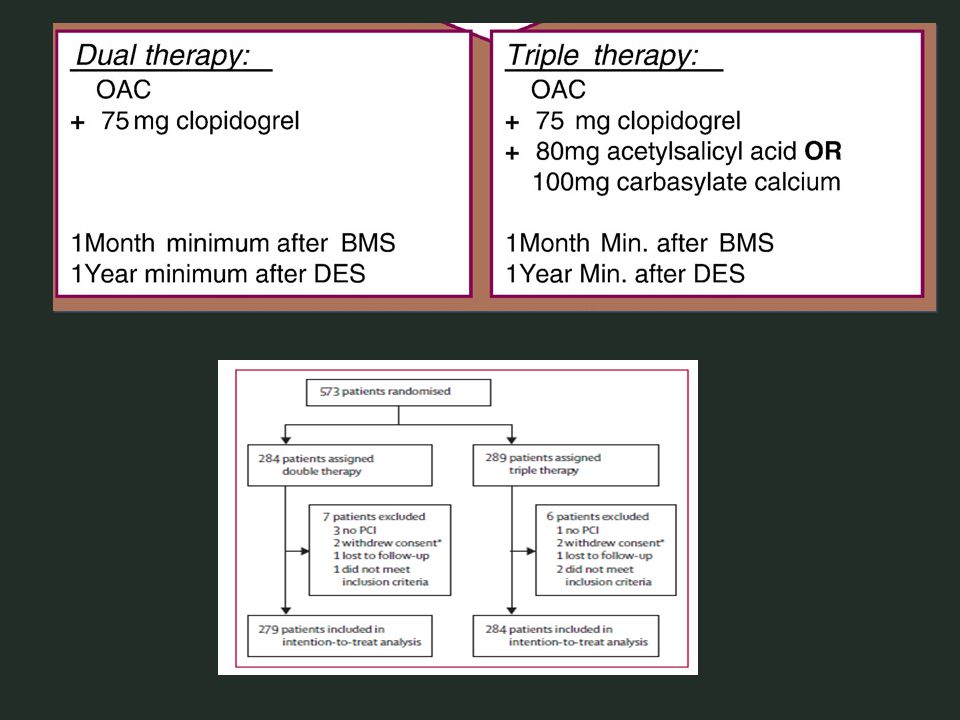
MUSICA-2 (http://clinicaltrials.gov/ct2/show/NCT01141153) 304 pts Indication to VKA + BMS or DES (ACS or elective) CHADS2 score <2 12-month follow-up Composite endpoint : stroke, SE, death, MI, ST, TVR, TIMI- bleeding Triple vs DAPT (ASA + clopidogrel)
 CHADS2 score <2 12-month follow-up Composite endpoint : stroke, SE, death, MI, ST, TVR, TIMI- bleeding Triple vs DAPT (ASA + clopidogrel)")
18
ACS Stented patients Ischemic events Stent thrombosis DAPT DAPT better than VKA 1 – 6 – 12 months ACS Stented patients Ischemic events Stent thrombosis DAPT DAPT better than VKA 1 – 6 – 12 months AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration
 valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration")
19
Complication of the picture (1) : New P2Y12 inhibitors in association with VKA ? LOV 2014
 : New P2Y12 inhibitors in association with VKA LOV 2014")
20
In both PLATO (ticagrelor) and TRITON-TIMI 38 (prasugrel) studies patients were excluded from enrollment if receiving VKA LOV 2014
 and TRITON-TIMI 38 (prasugrel) studies patients were excluded from enrollment if receiving VKA LOV 2014")
22
ACS Stented patients Ischemic events Stent thrombosis DAPT DAPT better than VKA 1 – 6 – 12 months ACS Stented patients Ischemic events Stent thrombosis DAPT DAPT better than VKA 1 – 6 – 12 months AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration
 valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong AF DVT PE LV thrombus (Mechanical) valves Stroke Systemic embolism VKA better than DAPT Sometimes lifelong Condition Aim : Prevention of Evidence Duration")
23
Complication of the picture (2) : NOACS in association with DAPT (aspirin+clopidogrel) ? LOV 2014
 : NOACS in association with DAPT (aspirin+clopidogrel) LOV 2014")
24
In all NOACS trials ( RELY, ROCKET-AF, ARISTOTLE) patients were excluded from enrollment if receiving new P2Y12 LOV 2014
 patients were excluded from enrollment if receiving new P2Y12 LOV 2014")
25
Some data are available in non AF patients LOV 2014 NOACS in association with DAPT (aspirin+clopidogrel) ?
")
27
Primary Outcome CV Death, MI, Ischemic Stroke Apixaban279 (7.5%) Placebo293 (7.9%) HR 0.95; 95% CI 0.80-1.11; p=0.509
 Placebo293 (7.9%) HR 0.95; 95% CI ; p=0.509")
28
TIMI Major Bleeding Apixaban 48 (1.3%) Placebo 18 (0.5%) HR 2.59; 95% CI 1.50–4.46; p=0.001
 Placebo 18 (0.5%) HR 2.59; 95% CI 1.50–4.46; p=0.001")
29
ATLAS ACS 2 TIMI 51 Rivaroxaban 2.5 mg bid n=4825 Rivaroxaban 2.5 mg bid n=4825 Placebo n=4821 Placebo n=4821 Rivaroxaban 5 mg bid n=4827 Rivaroxaban 5 mg bid n=4827 Event-driven study – 1002 events Stratum 2: ASA + thienopyridine (93%) Rivaroxaban 2.5 mg bid n=349 Rivaroxaban 2.5 mg bid n=349 Placebo n=355 Placebo n=355 Rivaroxaban 5 mg bid n=349 Rivaroxaban 5 mg bid n=349 Physician's decision to add thienopyridine or not N=15,526* ASA dose = 75–100 mg/day Stratum 1: ASA alone (7%) Mega et al, 2011 *184 patients were excluded from the efficacy analyses prior to unblinding because of trial misconduct at three sites
 Rivaroxaban 2.5 mg bid n=349 Rivaroxaban 2.5 mg bid n=349 Placebo n=355 Placebo n=355 Rivaroxaban 5 mg bid n=349 Rivaroxaban 5 mg bid n=349 Physician s decision to add thienopyridine or not N=15,526* ASA dose = 75–100 mg/day Stratum 1: ASA alone (7%) Mega et al, 2011 *184 patients were excluded from the efficacy analyses prior to unblinding because of trial misconduct at three sites")
30
Primary efficacy endpoint (CV death/MI/stroke) Both rivaroxaban doses, both strata Number at risk Placebo511343073470266418311079421 Rivaroxaban10,22985026753513735542084831 Months after randomization HR=0.84 (0.74–0.96) ARR=1.7% mITT p=0.008 ITT p=0.002 NNT=56 10.7% 8.9% 2-year Kaplan–Meier estimate Estimated cumulative rate (%) Rivaroxaban Placebo 12 0 0 16 10 8 6 4 2 2012 8 4 24 Mega et al, 2011
 Both rivaroxaban doses, both strata Number at risk Placebo Rivaroxaban10, Months after randomization HR=0.84 (0.74–0.96) ARR=1.7% mITT p=0.008 ITT p=0.002 NNT= % 8.9% 2-year Kaplan–Meier estimate Estimated cumulative rate (%) Rivaroxaban Placebo Mega et al, 2011")
31
Principal safety endpoint Separate rivaroxaban doses, both strata Rivaroxaban 2.5 mg bid (n=5115) Rivaroxaban 5 mg bid (n=5110) Placebo (n=5125) Non-CABG TIMI major bleed K–M estimate at 2 years1.8%2.4%0.6% p value versus placebo<0.001 ICH K–M estimate at 2 years0.4%0.7%0.2% p value versus placebo0.040.005 Fatal bleeding K–M estimate at 2 years0.1%0.4%0.2% p value versus placebo0.450.20 Fatal ICH K–M estimate at 2 years0.1%0.2%0.1% p value versus placebo–– Mega et al, 2011
 Rivaroxaban 5 mg bid (n=5110) Placebo (n=5125) Non-CABG TIMI major bleed K–M estimate at 2 years1.8%2.4%0.6% p value versus placebo<0.001 ICH K–M estimate at 2 years0.4%0.7%0.2% p value versus placebo Fatal bleeding K–M estimate at 2 years0.1%0.4%0.2% p value versus placebo Fatal ICH K–M estimate at 2 years0.1%0.2%0.1% p value versus placebo–– Mega et al, 2011")
32
What is the future ? (in patients requiring DAPT + OAC for AF stroke prevention ) LOV 2014
 LOV 2014")
33
PIONEER AF PCI 2200 patients

34
The RE-DUAL PCI™ trial (Randomized Evaluation of Dual Therapy with Dabigatran vs. Triple Therapy Strategy with Warfarin in Patients with NVAF that have undergone PCI with Stenting) Patients undergoing PCI Dabigatran (150 mg or 110 mg twice daily) + single antiplatelet therapy with a P2Y12 protein inhibitor compared to warfarin + two antiplatelet agents to assess clinically relevant bleeding and thrombotic events (combined rate of death, myocardial infarction and stroke)
 Patients undergoing PCI Dabigatran (150 mg or 110 mg twice daily) + single antiplatelet therapy with a P2Y12 protein inhibitor compared to warfarin + two antiplatelet agents to assess clinically relevant bleeding and thrombotic events (combined rate of death, myocardial infarction and stroke).")
35
2014 messages for the daily clinical practice in AF patients requiring DAPT + OAC (1) Indication : DAPT (clopidogrel + ASA) + VKA (= triple) Single APT (clopidogrel or ASA) + VKA (= WOEST) No indication : DAPT (ASA + prasugrel or ticagrelor) + VKA DAPT (ASA + clopidogrel) + NOACs DAPT (ASA + prasugrel or ticagrelor) + NOACs
 Indication : DAPT (clopidogrel + ASA) + VKA (= triple) Single APT (clopidogrel or ASA) + VKA (= WOEST) No indication : DAPT (ASA + prasugrel or ticagrelor) + VKA DAPT (ASA + clopidogrel) + NOACs DAPT (ASA + prasugrel or ticagrelor) + NOACs")
36
? Combination of drugs ? Duration of therapy Reduce intensity of VKA (INR 2.0 - 2.5) Prefer BMS Prefer radial access Evaluate clinical circumstances (ACS, elective stent) Evaluate bleeding risk profile (PPI, BP control, NSAID) 2014 messages for the daily clinical practice in AF patients requiring DAPT + OAC (2)
 Prefer BMS Prefer radial access Evaluate clinical circumstances (ACS, elective stent) Evaluate bleeding risk profile (PPI, BP control, NSAID) 2014 messages for the daily clinical practice in AF patients requiring DAPT + OAC (2).")
40
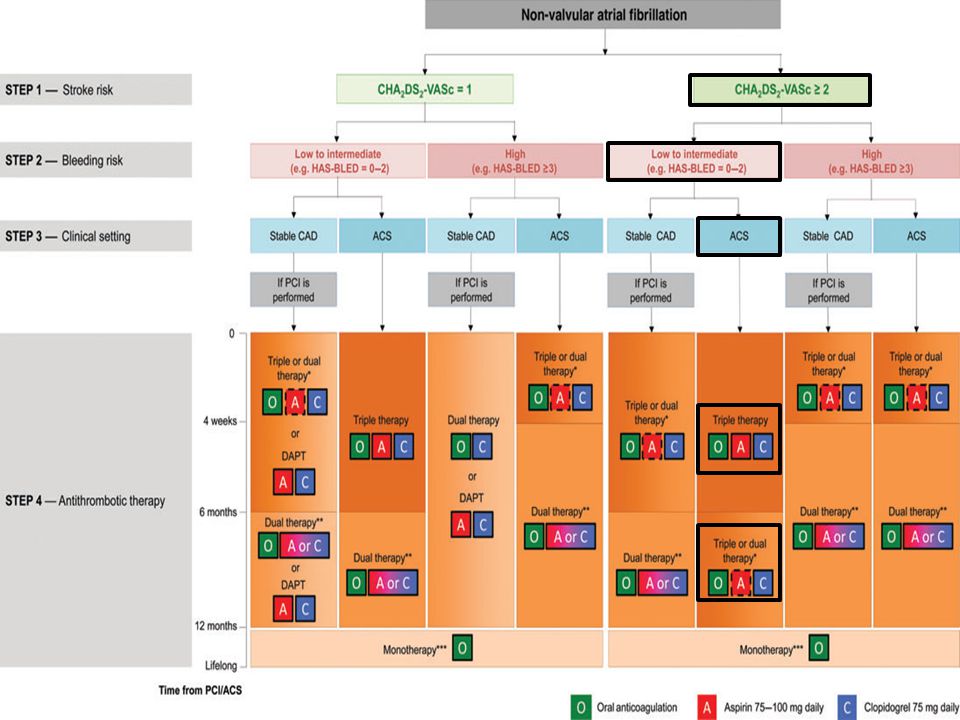
Patients with atrial fibrillation + Stent (ACS or Elective) * = INR 2.0-2.5 In low thrombotic risk DAPT is an alternative
 * = INR In low thrombotic risk DAPT is an alternative")
Similar presentations