Download presentation
Presentation is loading. Please wait.

1
Fungal Empyema

2
History 57 Male X smoker (20 pack) Admitted D6 with 1 week H/O: SOBE, Cough, minimal sputum SOBE, Cough, minimal sputum ? Fever & night sweating ? Fever & night sweating Being treated as CAP as outpatient with amoxicillin for 5 days No response to RX

3
History PMH : MDS April /02 AML Aug/02 Treated with {Cytarabine & Doxorubicin} Back to MDS oct/02 AML Aug /03 Treated with {Ara-c & Mixotracine} Sep/03

4
History No symptoms Of COPD NO IHD risk factor NO previous pneumonias No VTE No contact with TB No travel, occupational exposure,pets Systemic review unremarkable

5
History Medications: gatifluxacine Hydrxyurea Hydrxyurea allopurinol allopurinol Palliative case {transfusion dependent} No plans for further Chemo Nor BMT No plans for further Chemo Nor BMT

6
Examination Afebrile BP 120/70 HR 90 RR 18 Sat 86% RA 93% 5L O2 Chest :absent breath sounds Rt 2/3 Post dull percussion dull percussion CVS: S1+S2 +0 Abdomen : Hepatosplenomegaly LL: no edema or size difference

7
Investigations CBC : WBC 32000 {premature cells } Blasts 10000 Poly 550 Blasts 10000 Poly 550 Hb 77 Plt 22 PTT & INR N Hb 77 Plt 22 PTT & INR N BUN & Creat & Lytes N Alk Phos 162 LDH 420 Albumen 26 TP 86 ABG PH 7.45 PCO2 38 PO2 51 HCO3 27 PO2 51 HCO3 27 Sat 86% RA Sat 86% RA CXR & CT

8
Investigations Pleural Fluid Bloody Protein 68 LDH 1958 Glucose 1.4 Protein 68 LDH 1958 Glucose 1.4 WBC 9500 24% Poly 40% Blast WBC 9500 24% Poly 40% Blast RBC 2000 RBC 2000 GS +2 Poly & no organism GS +2 Poly & no organism C/S –ve C/S –ve Cytology AML with YEAST Cytology AML with YEAST

9
Investigations Cytology finding similar (Fungal element) Both on Oct 8 th {diagnostic} Both on Oct 8 th {diagnostic} & Oct 10 th {therapeutic} & Oct 10 th {therapeutic} -ve Fungal stain & C/S Being treated with Ampho B since Oct 8 th 3 rd tapping Oct 16 th -ve C/S -ve C/S
 Both on Oct 8 th {diagnostic} Both on Oct 8 th {diagnostic} & Oct 10 th {therapeutic} & Oct 10 th {therapeutic} -ve Fungal stain & C/S Being treated with Ampho B since Oct 8 th 3 rd tapping Oct 16 th -ve C/S -ve C/S")
10
Fungal Empyema Limited data Increasing incidence of fungal infections CDC report 1980 1990 Candida emerged as the 6 th most common nosocomial pathogen 7.2% Candida emerged as the 6 th most common nosocomial pathogen 7.2% More immunocompromised patients Increased use of broad spectrum Abx Increased Central Venous Catheters

11
Fungal Empyema Retrospective study Jan 1990 Dec1997 University Hospital Taiwan To analyze clinical spectrum, pathogenesis, treatment,outcomes & prognostic factors Shian-Chin Ko et al Shian-Chin Ko et al Chest June 2000 Chest June 2000

12
Fungal Empyema Fungal empyema Diagnosed by: * Isolation of Fungus from pleural fluid * Isolation of Fungus from pleural fluid (minimum 2 occasions) (minimum 2 occasions) * Signs of infection fever,leucocytosis * Signs of infection fever,leucocytosis * Isolation of the same fungus from other * Isolation of the same fungus from other specimens {blood, sputum, surgical wound} specimens {blood, sputum, surgical wound} or more than once from the pleural fluid or more than once from the pleural fluid Shian-Chin Ko et al Shian-Chin Ko et al Chest June 2000 Chest June 2000
 (minimum 2 occasions) * Signs of infection fever,leucocytosis * Signs of infection fever,leucocytosis * Isolation of the same fungus from other * Isolation of the same fungus from other specimens {blood, sputum, surgical wound} specimens {blood, sputum, surgical wound} or more than once from the pleural fluid or more than once from the pleural fluid Shian-Chin Ko et al Shian-Chin Ko et al Chest June 2000 Chest June 2000")
13
Fungal Empyema Considered Hospital acquired if developed 48 hours after admission Coexisting pneumonia if symptoms or CXR finding +ve Most patients were treated with standard chest tubes or pigtail Fibrinolytics, open drainage or decortication loculated effusion or clinical worsening loculated effusion or clinical worsening Shian-Chin Ko et al Shian-Chin Ko et al Chest June 2000 Chest June 2000

14
Fungal Empyema 111 cases identified 44 excluded because of: Fluid was transudate Fluid was transudate Patients were asymptomatic Patients were asymptomatic Single isolated fungal growth in the Single isolated fungal growth in the pleural fluid pleural fluid Isolation through prior chest tube Isolation through prior chest tube Shian-Chin Ko et al Shian-Chin Ko et al Chest June 2000 Chest June 2000

17
Fungal Empyema 60% received Abx 1 week before empyema 41% loculated effusion Mean Protein 3.5 LDH 3198 LDH 3198 Glucose 27 Glucose 27 69% Poly predominance

19
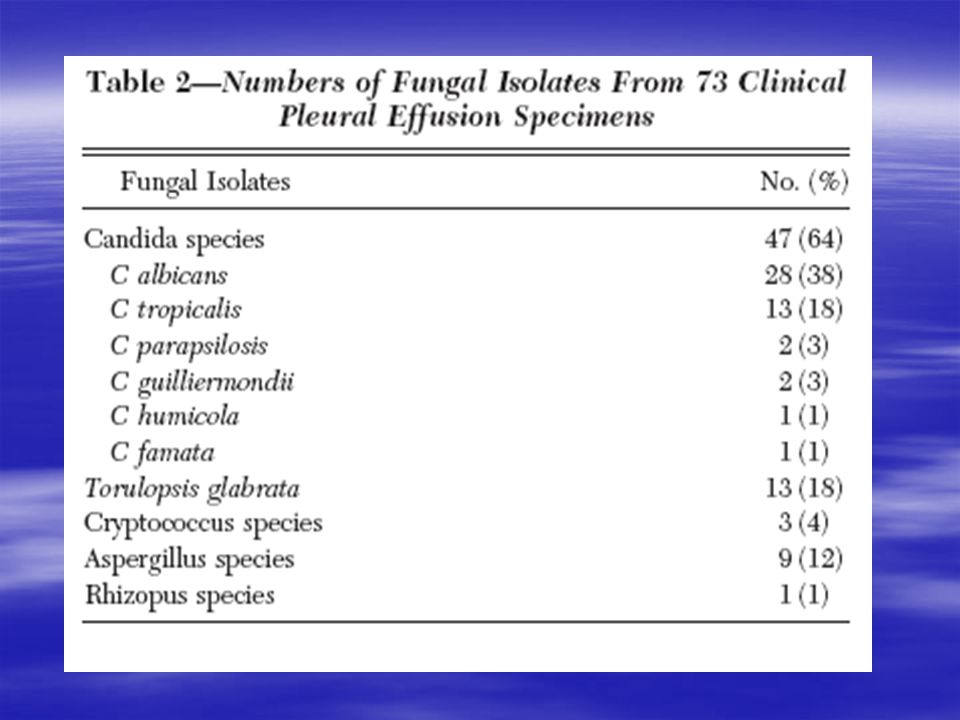
Fungal Empyema 28% Fungemia Candida 60% Vs Torulopsis 30% Candida 60% Vs Torulopsis 30% 24% bacterial empyema G-ve bacilli (45%) Pesudomonas G-ve bacilli (45%) Pesudomonas G+ve Enterococci & Staph G+ve Enterococci & Staph 28% bacteremia No significant correlation with increased mortality 28% bacteremia No significant correlation with increased mortality
 Pesudomonas G-ve bacilli (45%) Pesudomonas G+ve Enterococci & Staph G+ve Enterococci & Staph 28% bacteremia No significant correlation with increased mortality 28% bacteremia No significant correlation with increased mortality")
20
Fungal Empyema 49/67 died (73%) 43/49 (88%) immunocompromised All Torulopsis & more than one fungal isolate patients died Antifungal Rx : Fluconazole (33%) Fluconazole (33%) Ampho B (12%) Ampho B (12%) Combined (28%) Combined (28%)
 43/49 (88%) immunocompromised All Torulopsis & more than one fungal isolate patients died Antifungal Rx : Fluconazole (33%) Fluconazole (33%) Ampho B (12%) Ampho B (12%) Combined (28%) Combined (28%)")
21
Fungal Empyema 29/44 who had chest drainage died (66%) 20/23 who didn’t have drainage died (87%) All surgical intervention Pt 6 survived 4/6 Aspergillous lung abscess 4/6 Aspergillous lung abscess 2/6 Candida with poor response to antifungal 2/6 Candida with poor response to antifungal Multivariate analysis Immunosuppression, Lack of antifungal Rx & respiratory failure were independent risk factor for death
 20/23 who didn’t have drainage died (87%) All surgical intervention Pt 6 survived 4/6 Aspergillous lung abscess 4/6 Aspergillous lung abscess 2/6 Candida with poor response to antifungal 2/6 Candida with poor response to antifungal Multivariate analysis Immunosuppression, Lack of antifungal Rx & respiratory failure were independent risk factor for death")
Similar presentations