Download presentation
Presentation is loading. Please wait.

1
Nurse’s role In Comprehensive Sepsis Management
Kathleen M. Vollman RN, MSN, CCNS, FCCM Clinical Nurse Specialist/Educator/Consultant ADVANCING NURSING Northville, Michigan © Vollman 2009

2
Overview Significance of the Problem Defining the continuum
Brief overview of Pathophysiologic derangements Prevention Early Recognition & Resuscitation

3
Severe Sepsis: A Significant Healthcare Challenge
Major cause of morbidity and mortality worldwide Leading cause of death in noncoronary ICU (US)1 10th leading cause of death overall (US)2* More than 750,000 cases of severe sepsis in the US annually3 In the US, more than 500 patients die of severe sepsis daily3† Sepsis is a major worldwide cause of morbidity and mortality. Sands et al described the epidemiology of sepsis in eight academic medical centers in the United States. They reported that sepsis is the leading cause of death in patients admitted to noncoronary intensive care units. The National Vital Statistics Report indicates that sepsis is the 11th leading cause of death in the United States, based on data for septicemia. Angus et al studied the age-specific incidence and outcomes of severe sepsis in the United States. Their investigation indicates that there are more than 750,000 cases of severe sepsis (sepsis with acute organ dysfunction) each year in the United States. Based on data from Angus et al, more than 500 Americans die of severe sepsis daily. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome and associated costs of care. Crit Care Med 2001;29: Murphy SL. Deaths: final data for National Vital Statistics Reports Web site. Available at: Accessed January 2001. Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA 1997;278: * Based on data for septicemia †Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction 1 Sands KE, et al. JAMA 1997;278: 2 National Vital Statistics Reports 3 Angus DC, et al. Crit Care Med 2001;29:
1. 10th leading cause of death overall (US)2* More than 750,000 cases of severe sepsis in the US annually3. In the US, more than 500 patients die of severe sepsis daily3† Sepsis is a major worldwide cause of morbidity and mortality. Sands et al described the epidemiology of sepsis in eight academic medical centers in the United States. They reported that sepsis is the leading cause of death in patients admitted to noncoronary intensive care units. The National Vital Statistics Report indicates that sepsis is the 11th leading cause of death in the United States, based on data for septicemia. Angus et al studied the age-specific incidence and outcomes of severe sepsis in the United States. Their investigation indicates that there are more than 750,000 cases of severe sepsis (sepsis with acute organ dysfunction) each year in the United States. Based on data from Angus et al, more than 500 Americans die of severe sepsis daily. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome and associated costs of care. Crit Care Med 2001;29: Murphy SL. Deaths: final data for National Vital Statistics Reports Web site. Available at: Accessed January Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA 1997;278: * Based on data for septicemia. †Reflects hospital-wide cases of severe sepsis as defined by infection in the presence of organ dysfunction. 1 Sands KE, et al. JAMA 1997;278: National Vital Statistics Reports Angus DC, et al. Crit Care Med 2001;29:")
4
Severe Sepsis Is Common
1 in 10 patients admitted to the ICU has severe sepsis.* 2.26% of total hospital discharges nationally Incidence is expected to increase by nearly 17% by 2014. So – let’s start by looking at the size/scope of the problem. Just how common is severe sepsis? One out of every ten patients admitted to an ICU has severe sepsis, resulting in occurrence of 2.26% of all hospital discharges nationally. By 2014, the incidence of severe sepsis is expected to increase by nearly 17%. This increase is largely driven by the “graying” of America (increasing population of elderly). Additional drivers of the increased incidence includes antibiotic resistance, increasing invasive procedures, increasing incidence of immunosuppression for organ transplants and disease states (e.g., AIDS), etc. All analyses were performed using the 2000 MEDPAR Hospital Discharge Database. The information presented represents national averages, and similar analyses performed at an individual institution may provide different results. 1. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29(7): Data of file, Eli Lilly and Company: XIG b.
. Additional drivers of the increased incidence includes antibiotic resistance, increasing invasive procedures, increasing incidence of immunosuppression for organ transplants and disease states (e.g., AIDS), etc. All analyses were performed using the 2000 MEDPAR Hospital Discharge Database. The information presented represents national averages, and similar analyses performed at an individual institution may provide different results. 1. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29(7): Data of file, Eli Lilly and Company: XIG b.")
5
Severe Sepsis Is Common
Severe sepsis is more common than AIDS, colon cancer, and breast cancer combined. Incidence Cases/100,000 Angus et al studied the incidence, cost, and outcome of severe sepsis in the United States. In a study based on 1995 state hospital discharge records from 7 large states with population and hospital data from the US Census, Centers for Disease Control, HCFA, and the American Hospital Association, the investigators generated national sepsis data. In this study, they report that the incidence of severe sepsis is 300 cases/100,000 population. As shown on the slide, this is significantly greater than the incidence of other well recognized diseases as reported by the American Heart Association. AIDS1 Colon Cancer2 Breast Cancer2 CHF3 Severe Sepsis4 1. National Center for Health Statistics, American Cancer Society, American Heart Association Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29(7):
:")
6
Begin Proven Care Strategies
Early appropriate antibiotic use EGDT: Early Goal-Directed Therapy Low-tidal volume ventilation/ARDS/ALI Xigris if not contraindicated Tight glycemic control Low-dose steroid administration for refractory septic shock particularly in patients with relative adrenal insufficiency Implementation Through Proven Change Strategies

7
IHI/VHA Change Strategy
Care Bundles Grouping of care elements for particular symptoms, procedures or treatments Strong science, good methodology, poor process Bundle characteristics Solid evidence Relatively easy & inexpensive Individual components defined well Process not defined well

8
How Does Severe Sepsis Compare to Your Current Care Priorities?
Quality Projects US Incidence # of Deaths Mortality Rate AMI1 895,000 171,000 19% Stroke1 700,000 157,800 23% Pneumonia2 1,300,000 61,800 4.8% Severe Sepsis3 751,000 215,000 29% Why do you think that severe sepsis has not received the same focus as these other common disease states? 1. American Heart Association. Heart Disease and Stroke Statistics 2006 Update. 2. National Center for Health Statistics. Available at: Accessed February 4, Angus DC, et al. Crit Care Med 2001;29(7):
:")
9
4-Tier Process for Severe Sepsis Program Implementation
Measuring Success Implementation of the Sepsis Bundle Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively

10
National-All Hospital, Medicare Reporting-3670
Severe Sepsis Report National-All Hospital, Medicare Reporting-3670 Top Ten Severe Sepsis Diagnosis-Related Groups *† (53.5% of all cases with severe sepsis fell within 10 DRGs) Severe Sepsis Cases (average) All Others Mortality 27% 7% Ventilator Use 30% 2% Hospital Length of Stay 11.1 days 7.2 days ICU Length of Stay 6.5 days 4.2 days Cost per Case‡ $22,000 $12,000 Payment-to-Cost Ratio -24% 8% Background Information The data and analyses contained within this presentation have been compiled from fiscal years 2004 through 2006 MEDPAR Hospital Discharge Databases. These databases are a compilation of all hospital discharges between October 2003 and September 2006 in the United States for patients covered by Medicare (predominantly patients 65 and older). These databases do not contain information on patients from Private Payers (MCO, PPO, etc.). Information is presented using Diagnosis Related Groups (DRGs). The DRGs presented represent the top 10 DRGs by severe sepsis incidence. Severe sepsis cases were identified by looking for combinations of ICD-9-CM codes indicating infection and new onset of acute organ failure following ACCP/SCCM guidelines as described in Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29(7): Further, only those cases which included an ICU stay are included in this analysis. (costs exceeds payment) * All analyses were performed using the 2004 through 2006 MEDPAR Hospital Discharge Databases. Cost and charge data are reported in year-appropriate US Dollars. † Severe sepsis patients were identified by looking for combinations of ICD-9-CM codes indicating infection and new onset of acute organ failure following SCCM/ACCP guidelines as described in Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29 (7): ‡ Average total hospital costs for patients treated in the ICU. Copyright © 2007, Eli Lilly and Company. All rights reserved
 Severe Sepsis Cases. (average) All Others. Mortality. 27% 7% Ventilator Use. 30% 2% Hospital Length of Stay days. 7.2 days. ICU Length of Stay. 6.5 days. 4.2 days. Cost per Case‡ $22,000. $12,000. Payment-to-Cost Ratio. -24% 8% Background Information. The data and analyses contained within this presentation have been compiled from fiscal years 2004 through 2006 MEDPAR Hospital Discharge Databases. These databases are a compilation of all hospital discharges between October 2003 and September 2006 in the United States for patients covered by Medicare (predominantly patients 65 and older). These databases do not contain information on patients from Private Payers (MCO, PPO, etc.). Information is presented using Diagnosis Related Groups (DRGs). The DRGs presented represent the top 10 DRGs by severe sepsis incidence. Severe sepsis cases were identified by looking for combinations of ICD-9-CM codes indicating infection and new onset of acute organ failure following ACCP/SCCM guidelines as described in Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29(7): Further, only those cases which included an ICU stay are included in this analysis. (costs exceeds payment) * All analyses were performed using the 2004 through 2006 MEDPAR Hospital Discharge Databases. Cost and charge data are reported in year-appropriate US Dollars. † Severe sepsis patients were identified by looking for combinations of ICD-9-CM codes indicating infection and new onset of acute organ failure following SCCM/ACCP guidelines as described in Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Crit Care Med. 2001;29 (7): ‡ Average total hospital costs for patients treated in the ICU. Copyright © 2007, Eli Lilly and Company. All rights reserved.")
11
Organization Support Executive management at hospital actively supports the program Managing severe sepsis is aligned with hospital ‘s current year goals Willingness to align resources with program Understanding that this is a 2-3+ year program to make this the standard of practice for this patient population Existing culture that supports change Successfully implemented other major change programs—eg: vent bundle, tight glucose control, CR-BSI Established team in place with ICU physician and nurse champion, ED physician and nurse champion that are respected by staff

12
Building a Severe Sepsis Tool Kit: Project Team Charter
Severe Sepsis is Common and Deadly Problem Statement: Team Members ED, ICU, Patient Care Unit Representatives, Administration, Medical Staff, Nursing, Pharmacy, Performance Improvement, Case Management, Laboratory Goals Reduce severe sepsis mortality (make the goal specific and measurable) Business Case In comparison to other ICU patients, severe sepsis patients have a higher mortality rate, increased LOS, and an increased need for a ventilator Scope Severe sepsis patients in the ED, ICU, and patient care units Benefits Potential to improve outcomes Milestones Implementation of tiers 1, 2, 3, and 4
 Business Case. In comparison to other ICU patients, severe sepsis patients have a higher mortality rate, increased LOS, and an increased need for a ventilator. Scope. Severe sepsis patients in the ED, ICU, and patient care units. Benefits. Potential to improve outcomes. Milestones. Implementation of tiers 1, 2, 3, and 4.")
13
The Team is KEY!! Can Be Major Barrier If Not Functioning Well
Must have nurse and physician champions from ED and ICU (need at least one physician at all meetings) Must be linked in the organization’s quality or operational structure Must meet at least 2 times per month Team members must be well educated on the evidence and armed with tools and knowledge to change behavior at the bedside MUST have bedside nurses on team—provide reality check and best knowledge of barriers
 Must be linked in the organization’s quality or operational structure. Must meet at least 2 times per month. Team members must be well educated on the evidence and armed with tools and knowledge to change behavior at the bedside. MUST have bedside nurses on team—provide reality check and best knowledge of barriers.")
14
Severe Sepsis: Defining a Disease Continuum
Infection or Trauma Sepsis Severe Sepsis SIRS Sepsis with 1 sign of organ dysfunction, hypoperfusion or hypotension. Examples: Cardiovascular (refractory hypotension) Renal Respiratory Hepatic Hematologic CNS Unexplained metabolic acidosis Adult Criteria A clinical response arising from a nonspecific insult, including ≥ 2 of the following: Temperature:> 38°C or < 36°C Heart Rate: > 90 beats/min Respiration: > 20/min WBC count: > 12,000/mm3, or < 4,000/mm3, or > 10% immature neutrophils SIRS with a presumed or confirmed infectious process Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis Shock SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101:
 Renal. Respiratory. Hepatic. Hematologic. CNS. Unexplained metabolic acidosis. Adult Criteria. A clinical response arising from a nonspecific insult, including ≥ 2 of the following: Temperature:> 38°C or < 36°C. Heart Rate: > 90 beats/min. Respiration: > 20/min. WBC count: > 12,000/mm3, or < 4,000/mm3, or > 10% immature neutrophils. SIRS with a presumed or confirmed infectious process. Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis. Shock. SIRS = Systemic Inflammatory Response Syndrome. Bone et al. Chest.1992;101:")
15
Severe Sepsis: Defining a Disease Continuum
Infection or Trauma SIRS Sepsis Severe Sepsis Adult Criteria A clinical response arising from a nonspecific insult, including ≥ 2 of the following: Temperature:> 38°C or < 36°C Heart Rate: > 90 beats/min Respiration: > 20/min WBC count: > 12,000/mm3, or < 4,000/mm3, or > 10% immature neutrophils Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101:
 of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis. SIRS = Systemic Inflammatory Response Syndrome. Bone et al. Chest.1992;101:")
16
Signs & Symptoms of Sepsis
31 Platelets Bands Skin perfusion Urine output Skin mottling Poor capillary refill Hyperglycemia Purpura/petechia Chills Alteration in LOC Tachypnea Unexplained metabolic acidosis Heart rate Altered blood pressure Levy M, et al. Crit Care Med 2003;31:

17
Severe Sepsis: Defining a Disease Continuum
Infection or Trauma SIRS Sepsis Severe Sepsis SIRS with a presumed or confirmed infectious process Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101:
 of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis. SIRS = Systemic Inflammatory Response Syndrome. Bone et al. Chest.1992;101:")
18
Severe Sepsis: Defining a Disease Continuum
Infection or Trauma SIRS Sepsis Severe Sepsis Sepsis with 1 sign of organ dysfunction, hypoperfusion or hypotension . Examples: Cardiovascular (refractory hypotension) Renal Respiratory Hepatic Hematologic CNS Unexplained metabolic acidosis Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis Shock SIRS = Systemic Inflammatory Response Syndrome Bone et al. Chest.1992;101:
 Renal. Respiratory. Hepatic. Hematologic. CNS. Unexplained metabolic acidosis. Beyond the basic definition, it is helpful to think of sepsis as a continuum: Beginning with a localized infection that triggers a systemic response, called SIRS. SIRS due to infection is sepsis. Once the patient experiences organ dysfunction due to sepsis, that patient has the clinical diagnosis of severe sepsis. Any acute organ dysfunction qualifies the patient for the diagnosis of severe sepsis. Several examples of potential organ systems are listed on the slide. If the cardiovascular organ dysfunction deteriorates into shock, then this is commonly referred to as septic shock. Septic shock is a form (subgroup) of severe sepsis. Infection + SIRS + Organ Dysfunction = Severe Sepsis. Shock. SIRS = Systemic Inflammatory Response Syndrome. Bone et al. Chest.1992;101:")
19
Identifying Acute Organ Dysfunction as a Marker of Severe Sepsis
Cardiovascular Respiratory Tachycardia SBP<90mmHg MAP < 70mmHg (despite fluid) Need for Vasopressors PaO2/FiO2 200 if lung only dysfunction/site of infection PaO2/FiO2 250 with other organ dysfunction/lung not site of infection Renal UO <0.5 ml/kg per hr (despite fluid) Metabolic Following identification of a patient with sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure Kidney: oliguria, anuria, increased creatinine Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimers Unexplained metabolic acidosis Lactate > 1.5 times upper normal Hematologic Platelets <80,000/mm3 Decline in platelet count of 50% over 3 days
 Need for Vasopressors. PaO2/FiO2 200 if lung only dysfunction/site of infection. PaO2/FiO2 250 with other organ dysfunction/lung not site of infection. Renal. UO <0.5 ml/kg per hr. (despite fluid) Metabolic. Following identification of a patient with sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium. Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen. Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time. Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure. Kidney: oliguria, anuria, increased creatinine. Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimers. Unexplained metabolic acidosis. Lactate > 1.5 times upper normal. Hematologic. Platelets <80,000/mm3. Decline in platelet count of 50% over 3 days.")
20
Tachycardia generally compensatory mechanism for tissue hypoxia and can be caused by many factors:
Hypovolemia Shock Fever Pain / Agitation Absence of tachycardia may be caused by other factors: Spinal cord injury Beta blocker therapy Clinical signs of a dysfunctional cardiovascular system include: tachycardia (which is a SIRS criteria), hypotension, altered CVP and/or PAOP, and poor capillary refill (evidence of poor tissue perfusion). Symptoms are frequently related to subsequent hypoperfusion/cellular hypoxemia. Confusion is a very early symptom but not very specific. Whenever a patient has a change in level of consciousness the patient should be carefully evaluated for the cause of the change (early severe sepsis should be included in the differential diagnosis). If a patient’s BP is normalized with vasopressors, this is cardiovascular dysfunction despite a normal BP. The BP number may be comforting; however, a good BP does not equate to good blood flow/tissue perfusion. The check-box criteria at the bottom of the slide brings you back to some simple, measurable criteria to keep in mind when assessing for organ dysfunction.
, hypotension, altered CVP and/or PAOP, and poor capillary refill (evidence of poor tissue perfusion). Symptoms are frequently related to subsequent hypoperfusion/cellular hypoxemia. Confusion is a very early symptom but not very specific. Whenever a patient has a change in level of consciousness the patient should be carefully evaluated for the cause of the change (early severe sepsis should be included in the differential diagnosis). If a patient’s BP is normalized with vasopressors, this is cardiovascular dysfunction despite a normal BP. The BP number may be comforting; however, a good BP does not equate to good blood flow/tissue perfusion. The check-box criteria at the bottom of the slide brings you back to some simple, measurable criteria to keep in mind when assessing for organ dysfunction.")
21
Deterioration of Cardiovascular Function on Day 1 was Associated with Increased Mortality in Placebo Patients Change in Vasopressor Dose on Day 1*† 70 P<0.0001 60 50 % Mortality 40 30 20 n=294 n=41 n=36 n=46 No Vasopressor No Vasopressor to Low Dose No Vasopressor to High Dose CV SOFA Increased by 1 * 28-day mortality for standard therapy patients enrolled in PROWESS and a Phase II study of an investigational anti-sepsis drug. † Vasopressor requirement at study entry through day 1. Based on the Sequential Organ Failure Assessment (SOFA) score, low dose was defined as dopamine 6-15 µg/kg/min, epinephrine 0.1 µg/kg/min, or norepinephrine 0.1 µg/kg/min. High dose was defined as dopamine > 15 µg/kg/min, epinephrine > 0.1 µg/kg/min, or norepinephrine >0.1 µg/kg/min. Levy, M., Macias, W., Vincent, J., et al. Early changes in organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8.
 score, low dose was defined as dopamine 6-15 µg/kg/min, epinephrine 0.1 µg/kg/min, or norepinephrine 0.1 µg/kg/min. High dose was defined as dopamine > 15 µg/kg/min, epinephrine > 0.1 µg/kg/min, or norepinephrine >0.1 µg/kg/min. Levy, M., Macias, W., Vincent, J., et al. Early changes in organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8.")
22
Signs of respiratory organ dysfunction include the very early and sometimes subtle development of tachypnea (also a SIRS criteria). This may be a compensatory mechanism for hypoxemia. Additional assessments such as a P/F ratio, chest xray or ABG may be evaluated for abnormalities. Once again symptoms of cyanosis (appears late), difficult breathing or change in LOC should be carefully evaluated for cause and development of organ dysfunction. The illustration helps understand a potential cause of respiratory organ dysfunction. The blood is visualized within the vessels in white, these vessels should be in a connecting pattern. However, areas of black indicate obstruction to blood flow resulting in blood bypassing the alveoli where oxygen/CO2 exchange occurs.

23
PaO2/FiO2 Ratio User friendly tool
Crude assessment of the severity of lung injury May be used in the assessment of Acute Respiratory Dysfunction due to Severe Sepsis Also used in the definition of Acute Lung Injury (ALI) and Acute Respiratory Distress Syndrome (ARDS) PaO2 = 70 torr FiO2 = 60% or .60 P/F Ratio = 70/.60 Answer: 117
 and Acute Respiratory Distress Syndrome (ARDS) PaO2 = 70 torr. FiO2 = 60% or .60. P/F Ratio = 70/.60. Answer: 117.")
24
Respiratory Dysfunction (Mortality by Change in SOFA Score) in Placebo Patients
Severe sepsis mortality predictors (Baseline to Day 1) Population-based outcomes observed in severe sepsis patients p=0.0004 N=355 N=398 N=94 Levy, M., Macias, W., Vincent, J., et al. Early changes in organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8.
 Population-based outcomes observed in severe sepsis patients. p= N=355. N=398. N=94. Levy, M., Macias, W., Vincent, J., et al. Early changes in organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8.")
25
It is very important to assess renal status when a patient has sepsis because the organ is commonly affected and urine output is readily accessible as an assessment parameter. If you are concerned that a patient has renal dysfunction it is important to perform a weight based calculation for assessment of low urine output. The standard usage of 30 cc’s or urine per hour may not be adequate for patients larger than 60 kg. Creatinine is a nonprotein end product of creatine metabolism. Similar to creatine, creatinine appears in serum in amounts proportional to the body’s muscle mass. Unlike creatine; creatinine is easily excreted by the kidneys. Because creatinine levels normally remain constant, elevated levels usually indicate diminished renal function.

26
Renal Dysfunction (Mortality by Change in Serum Creatinine) in Placebo Patients
Severe sepsis mortality predictors (Baseline to Day 1) Population-based outcomes observed in severe sepsis patients In PROWESS, patients with chronic kidney failure on dialysis were excluded. The following was observed in patients with acute kidney dysfunction at baseline (renal SOFA = 2)†‡ CMH Trend Test P<0.0001 61% 35% 19% N=129 N=109 N=38 1.2 TO 1.9 mg/dL TO < 1.2 mg/dL 1.2 TO 1.9 mg/dL TO 1.2 TO 1.9 mg/dL TO > 1.9 mg/dL Levy, M., Macias, W., Vincent, J., et al. Early changes in organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8. Data on file, Eli Lilly and Company: XIG a. † Renal SOFA Score = 2 equivalent to creatinine range mg/dL. ‡ APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please see
 Population-based outcomes observed in severe sepsis patients In PROWESS, patients with chronic kidney failure on dialysis were excluded. The following was observed in patients with acute kidney dysfunction at baseline (renal SOFA = 2)†‡ CMH Trend Test. P< % 35% 19% N=129. N=109. N= TO 1.9 mg/dL. TO. < 1.2 mg/dL. 1.2 TO 1.9 mg/dL. TO. 1.2 TO 1.9 mg/dL. TO. > 1.9 mg/dL. Levy, M., Macias, W., Vincent, J., et al. Early changes in. organ function predict eventual survival in severe sepsis. Crit Care Med. 2005; 33:1-8. Data on file, Eli Lilly and Company: XIG a. † Renal SOFA Score = 2 equivalent to creatinine range mg/dL. ‡ APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please see")
27
Because coagulopathy is part of the underlying disease process in severe sepsis, it is important to assess a patient for hematologic dysfunction if severe sepsis is suspected. Markers for the disease state/organ dysfunction are listed on the slide. Remember that coagulation times will increase secondary to consumption of clotting factors, among other factors. Numerous factors may interfere with the aPTT measure (eg, drugs such as heparin), thus PT or INR may be the better parameters to evaluate disease state status. Platelets are important to monitor because as they decrease in number a patient not only is at increased risk for bleeding but they also may be increasing their risk of death. Thrombocytopenia should be evaluated carefully for cause, it may signify the development of acute organ dysfunction and the onset of severe sepsis.

28
Because coagulopathy is part of the underlying disease process in severe sepsis, it is important to assess a patient for hematologic dysfunction if severe sepsis is suspected. Markers for the disease state/organ dysfunction are listed on the slide. Remember that coagulation times will increase secondary to consumption of clotting factors, among other factors. Numerous factors may interfere with the aPTT measure (eg, drugs such as heparin), thus PT or INR may be the better parameters to evaluate disease state status. Platelets are important to monitor because as they decrease in number a patient not only is at increased risk for bleeding but they also may be increasing their risk of death. Thrombocytopenia should be evaluated carefully for cause, it may signify the development of acute organ dysfunction and the onset of severe sepsis.

29
When making a diagnosis of severe sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances, laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen (p/f ratio= paO2 divided by FiO2) Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure Kidney: oliguria, anuria, increased creatinine Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:
 Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time. Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure. Kidney: oliguria, anuria, increased creatinine. Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer. Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:")
30
When making a diagnosis of severe sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances, laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen (p/f ratio= paO2 divided by FiO2) Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure Kidney: oliguria, anuria, increased creatinine Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:
 Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time. Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure. Kidney: oliguria, anuria, increased creatinine. Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer. Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:")
31
When making a diagnosis of severe sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances, laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen (p/f ratio= paO2 divided by FiO2) Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure Kidney: oliguria, anuria, increased creatinine Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:
 Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time. Cardiovascular: tachycardia, hypotension, altered central venous pressure, altered pulmonary artery occlusive pressure. Kidney: oliguria, anuria, increased creatinine. Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimer. Balk RA. Pathogenesis and management of multiple organ dysfunction or failure in severe sepsis and septic shock. Crit Care Clin 2000;16:")
32
Homeostasis Is Unbalanced in Severe Sepsis
FIBRINOLYSIS COAGULATION INFLAMMATION In simplified terms, sepsis can be conceptualized as a dysfunction of opposing mechanisms of coagulation/inflammation and fibrinolysis. In normal patients, homeostasis is maintained because these mechanisms balance each other. Patients with severe sepsis have increased coagulation and increased inflammation. Manifestations of these include: Circulating proinflammatory mediators Endothelial injury Expression of tissue factor by monocytes and possibly a subset of endothelial cells Thrombin generation Patients with severe sepsis also have decreased fibrinolysis. Manifestations of these include: Increased levels of PAI-1 Increased levels of TAFI Carvalho AC, Freeman NJ. How coagulation defects alter outcome in sepsis: survival may depend on reversing procoagulant conditions. J Crit Illness 1994;9:51-75. Kidokoro A, Iba T, Fukunaga M, et al. Alterations in coagulation and fibrinolysis during sepsis. Shock 1996;5:223-8. Vervloet MG, Thijs LG, Hack CE. Derangements of coagulation and fibrinolysis in critically ill patients with sepsis and septic shock. Semin Thromb Hemost 1998;24:33-44. Homeostasis Carvalho AC, Freeman NJ. J Crit Illness 1994;9:51-75. Kidokoro A, et al. Shock 1996;5:223-8. Vervloet MG, et al. Semin Thromb Hemost 1998;24:33-44.

33
SEVERE SEPSIS PATHOPHYSIOLOGY
The initial inflammation of severe sepsis effects the microvasculature through multiple pathways. The white blood cells become activated and release mediators which in part activate systemic coagulation and the formation of clots in the microvasculature. Severe sepsis also leads to decreased fibrinolysis, thus reducing the body’s innate ability to lyse clots. The clots accumulate, leading to hypoperfusion and cellular hypoxia. Additionally the white blood cells migrate through the endothelial walls which contributes to the endothelial dysfunction of severe sepsis. Organ dysfunction may result from either global tissue hypoxia and/or direct damage to the organ cells/tissue. The drawing visually depicts what is likely occurring inside the microvasculature. Microvascular dysfunction Inflammation Coagulation Fibrinolysis Hypoperfusion/hypoxia Microvascular thrombosis Endothelial dysfunction Organ dysfunction Global tissue hypoxia Direct tissue damage

34
Inflammation, Coagulation and Impaired Fibrinolysis In Severe Sepsis
Endothelium COAGULATION CASCADE Tissue Factor Neutrophil Monocyte IL-6 IL-1 TNF- Factor VIIIa PAI-1 Suppressed fibrinolysis Factor Va THROMBIN Fibrin Fibrin clot Tissue Factor Inflammatory Response to Infection Thrombotic Response to Infection Fibrinolytic Response to Infection Adapted from Bernard GR, et al. N Engl J Med. 2001;344:

35
The Role Of Endogenous Activated Protein C In Severe Sepsis
Inactivation Endothelium COAGULATION CASCADE Tissue Factor Neutrophil Monocyte IL-6 Factor VIIIa PAI-1 Inactivation Activated Protein C Organisms Factor Va Activated Protein C Reduction of Rolling Inhibition Suppressed fibrinolysis THROMBIN Fibrin Fibrin clot Tissue Factor Inflammatory Response to Infection Thrombotic Response to Infection Fibrinolytic Response to Infection Adapted from Bernard GR, et al. N Engl J Med. 2001;344:

36
Pathophysiologic Characteristics in Severe Sepsis
Maldistribution of blood flow Imbalance of oxygen supply & demand Metabolic alterations & activation of the stress response © Vollman 2001

37
Maldistribution of Blood Flow
Mechanical obstruction Micro-emboli Increased blood viscosity Compression Systemic & local mediator & ion influence Constriction vs. dilation Loss of regulatory activities/endothelial cell injury Reactive hyperemia Anticoagulation © Vollman 2001

38
Imbalance of Oxygen Supply & Demand
© Vollman 2001

39
OXYGEN SUPPLY/DEMAND DYNAMICS
ScvO2 CVP, CO, CI, SV, SVI

40
O 2 Supply/Demand Compensatory Mechanisms
Improve pulmonary gas exchange Increase oxygen delivery Alter the distribution of blood flow

41
O2 Supply Debt

42
Metabolic Alterations & The Stress Response
Initiation of the Stress Response Sympathetic Nervous System Activation Hypothalamus Activation

43
Metabolic Alterations & The Stress Response
SNS Activation Gut hypothesis BMR Inhibition of insulin secretion Inhibition of glucose uptake by the tissues Hypothalamus Activation Adrenal cortex stimulation Changes in carbohydrate, protein & fat metabolism resulting in glucose concentration

44
Except on few occasions, the patient appears to die from the body's response to infection rather than from it." Sir William Osler – 1904 The Evolution of Modern Medicine

45
The Nurse’s Role Prevention of infection
Early recognition of patients with signs of sepsis Early initiation of evidence-based practice therapies appropriate for your area of practice (antibiotics, fluids/blood, and vasopressors) Swift disposition to care areas where the rest of the bundle can be started
 Swift disposition to care areas where the rest of the bundle can be started.")
46
Prevention of Infection
Ventilator-associated pneumonia Hospital acquired pneumonia Bloodstream infection related to an invasive catheter Are you currently working on strategies to prevent infections?

47
PREVENTING THE INVASION
Handwashing Line care Oral care HOB © Vollman 2001

48
ICU/Additional Evidence
EARLY MANAGEMENT Early Recognition Early Antibiotics Prompt/Aggressive Resuscitation ICU/Additional Evidence Based Therapies

49
2nd-Tier Implementation of Early Screening Tools and Triggers
Screens and triggers developed to ID Severe Sepsis patients in the ED, ICU, and on patient care units Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively

50
Early Recognition: A Screening Process
TIME IS TISSUE!! If you identify patients early then you can intervene and prevent further tissue damage To screen effectively, it must be part of the nurses’ daily routine Must define a process for what to do with the results of the screen If you don’t screen you will miss patients that could have benefited from the interventions

51
Make it Process Dependent
Weave into fabric of current practice Assess for daily Identify strategies for initiation of therapy response once patient is identified

52
“Triggers” for Identifying Severe Sepsis Location/ Trigger Type
Standard Procedure Manual Alert Message Computerized Alert Message Emergency Department Triage: Criteria-Based Early Response Concurrent coder or case manager Upon pharmacy entry of vasopressor/ antibiotic Lactate drawn as a screen Order sheets antibiotic/ vasopressor Upon withdrawal of med from Automated Dispensing Cabinet Change in lactate Change in lab values (lactate) Upon scanning of medication at bedside
 Upon scanning of medication at bedside.")
53
“Triggers” for Identifying Severe Sepsis Location/ Trigger Type
Standard Procedure Manual Alert Message Computerized Alert Message ICU Upon admission From concurrent coder or case manager Upon pharmacy entry of vasopressor/ antibiotic By nurse at shift change Nurse MAR review (for antibiotic/ vasopressor) In note field on computerized MAR Change in lactate During MD, RN, RPh, rounds Change in lab values (lactate) In note field of vasopressor computerized label Criteria-Based Early Response Place on all ICU charts (daily) Upon withdrawal of med from Automated Dispensing Cabinet Upon scanning of medication at bedside
 In note field on computerized MAR. Change in lactate. During MD, RN, RPh, rounds. Change in lab values (lactate) In note field of vasopressor computerized label. Criteria-Based Early Response. Place on all ICU charts (daily) Upon withdrawal of med from Automated Dispensing Cabinet. Upon scanning of medication at bedside.")
56
“Triggers” for Identifying Severe Sepsis Location/ Trigger Type
Standard Procedure Manual Alert Message Computerized Alert Message Patient Care Units Upon admission From concurrent coder or case manager Upon pharmacy entry of antibiotic During MD, RN, RPh, rounds Nurse MAR review for antibiotic In note field on computerized MAR Criteria-Based Early Response teams Change in patient hemodynamics In note field of vasopressor computerized label Need to mobilize MET Upon withdrawal of med from Automated Dispensing Cabinet Change in lab values (e.g., elevated WBC, decreased platelet count) Upon scanning of medication at bedside
 Upon scanning of medication at bedside.")
57
Reaching Outside the ICU: Early Recognition Models
Shock Program Medical Emergency Response Team (MET) Critical Care Nurse Consultant Service
 Critical Care Nurse Consultant Service.")
58
Screening: Barriers/Strategies
Time for nurses to do it (perception vs reality) Screening is not sensitive only for severe sepsis Positive screen is not a diagnosis of severe sepsis Strategies Must assign responsibility and hold them accountable-- Perform audits to measure compliance and identify problems Round on unit and ask nurses how it is going and discuss issues
 Screening is not sensitive only for severe sepsis. Positive screen is not a diagnosis of severe sepsis. Strategies. Must assign responsibility and hold them accountable-- Perform audits to measure compliance and identify problems. Round on unit and ask nurses how it is going and discuss issues.")
59
Screening: Barriers/Strategies
Lesson Learned: Bedside nurse must do screening Education/Simulation/Education Every 6 months Build into orientation Must be part of their documentation structure Practice-Practice-Practice The END RESULT—anytime patient has 2 or more SIRS—will think that this patient might have sepsis and can screen at that time

60
ICU/Additional Evidence
EARLY MANAGEMENT Early Recognition Early Antibiotics Prompt/Aggressive Resuscitation ICU/Additional Evidence Based Therapies

61
3rd-Tier Implementation of Evidence-Based Sepsis Bundles
the Sepsis Bundle with protocol & order sets Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively

62
The Severe Sepsis Bundles: Surviving Sepsis Campaign/IHI
Resuscitation Bundle (To be accomplished as soon as possible and scored over first 6 hours): Serum lactate measured. Blood cultures obtained prior to antibiotics administered. (1C) Perform imaging studies promptly to fine source (1C) From the time of presentation, broad- spectrum antibiotics within 3 hours for ED admissions and 1 hour for non-ED ICU admissions. (1D/1B) For hypotension and/or lactate > 4 mmol/L: Deliver an initial minimum of 20 mL/kg of crystalloid (or colloid equivalent) (1C) Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mmHg. For persistent hypotension despite initial fluid resuscitation (septic shock) and/or lactate > 4 mmol/L: 1C Achieve CVP > 8 mmHg & MAP > 65 mmHg & UO >0.5mL/kg/hr Achieve ScvO2 of > 70% or SvO2 > 65%. if ScvO2 not > 70% blood or dobutamine (2C) Management Bundle (To be accomplished as soon as possible and scored over first 24 hours): Low-dose steroids administered for septic shock in accordance with a standardized ICU policy. (Given to patients who respond poorly to fluids or vasopressors) (2C) Drotrecogin alfa (activated) administered in accordance with a standardized ICU policy. (Given to patients with sepsis induced organ dysfunction at high risk of death (2B) Glucose control maintained to < 150 mg/dL (8.3 mmol/L). (2C) Tidal volume 6 ml/kg (1B) Inspiratory plateau pressures < 30 cmH2O for mechanically ventilated patients. (1C) Adapted from the revised guidelines: CCM 2008;36: Bleeding is the most common adverse effect associated with Xigris therapy. See Important Safety Information in this presentation.
: Serum lactate measured. Blood cultures obtained prior to antibiotics administered. (1C) Perform imaging studies promptly to fine source (1C) From the time of presentation, broad- spectrum antibiotics within 3 hours for ED admissions and 1 hour for non-ED ICU admissions. (1D/1B) For hypotension and/or lactate > 4 mmol/L: Deliver an initial minimum of 20 mL/kg of crystalloid (or colloid equivalent) (1C) Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mmHg. For persistent hypotension despite initial fluid resuscitation (septic shock) and/or lactate > 4 mmol/L: 1C. Achieve CVP > 8 mmHg & MAP > 65 mmHg & UO >0.5mL/kg/hr. Achieve ScvO2 of > 70% or SvO2 > 65%. if ScvO2 not > 70% blood or dobutamine (2C) Management Bundle. (To be accomplished as soon as possible and scored over first 24 hours): Low-dose steroids administered for septic shock in accordance with a standardized ICU policy. (Given to patients who respond poorly to fluids or vasopressors) (2C) Drotrecogin alfa (activated) administered in accordance with a standardized ICU policy. (Given to patients with sepsis induced organ dysfunction at high risk of death (2B) Glucose control maintained to < 150 mg/dL (8.3 mmol/L). (2C) Tidal volume 6 ml/kg (1B) Inspiratory plateau pressures < 30 cmH2O for mechanically ventilated patients. (1C) Adapted from the revised guidelines: CCM 2008;36: Bleeding is the most common adverse effect associated with Xigris therapy. See Important Safety Information in this presentation.")
63
SURVIVING SEPSIS GUIDELINES 2008
The GRADE system is based on a sequential assessment of the quality of evidence, followed by assessment of the balance between benefits versus risks, burden, and cost and, based on the above, development and grading of a management recommendations. Keeping the rating of quality of evidence and strength of recommendation explicitly separate constitutes a crucial and defining feature of the GRADE approach. This system classifies quality of evidence as high (Grade A), moderate (Grade B), low (Grade C), or very low (Grade D). The GRADE system classifies recommendations as strong (Grade 1) or weak (Grade 2). The grade of strong or weak is considered of greater clinical importance than a difference in letter level of quality of evidence. 1. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: Crit Care Med. 2008;36:
, moderate (Grade B), low (Grade C), or very low (Grade D). The GRADE system classifies recommendations as strong (Grade 1) or weak (Grade 2). The grade of strong or weak is considered of greater clinical importance than a difference in letter level of quality of evidence. 1. Dellinger RP, Levy MM, Carlet JM, et al. Surviving Sepsis Campaign: International guidelines for management. of severe sepsis and septic shock: Crit Care Med. 2008;36:")
64
Strength of the Science: Part 1 of Grading System
Grading of Recommendations: Supported by at least two level I investigations Supported by one level I investigation Supported by level II investigations only Supported by at least one level III investigation Supported by level IV or V evidence Recommendations are published in groups by category and not by hierarchy Dellinger RP, et al. Crit Care Med. 2008;36: 64 64

65
New Grading System Quality of the evidence process = no change
Recommendation process = new

66
Which components of the bundle do you believe will encounter the most resistance?

67
PROMPT AGGRESSIVE RESUSCITATION
“Early Goal Directed Therapy”

68
Sepsis Resuscitation Bundle
(To be accomplished as soon as possible over first 6 hours): 1. Serum lactate measured. 2. Blood cultures obtained prior to antibiotic administration. 3. From the time of presentation, broad-spectrum antibiotics administered within 3 hours for ED admissions and 1 hour for non-ED ICU admissions. 4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): a) Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent*). b) Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg. 5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/L (36 mg/dl): a) Achieve central venous pressure (CVP) of > 8 mm Hg. b) Achieve central venous oxygen saturation (ScvO2) of > 70%.**
: 1. Serum lactate measured. 2. Blood cultures obtained prior to antibiotic administration. 3. From the time of presentation, broad-spectrum antibiotics administered within 3 hours for ED admissions and 1 hour for non-ED ICU admissions. 4. In the event of hypotension and/or lactate > 4 mmol/L (36 mg/dl): a) Deliver an initial minimum of 20 ml/kg of crystalloid (or colloid equivalent*). b) Apply vasopressors for hypotension not responding to initial fluid resuscitation to. maintain mean arterial pressure (MAP) > 65 mm Hg. 5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or. lactate > 4 mmol/L (36 mg/dl): a) Achieve central venous pressure (CVP) of > 8 mm Hg. b) Achieve central venous oxygen saturation (ScvO2) of > 70%.**")
69
Early Goal Directed Therapy
Methodology: 263 severe sepsis patients Early Goal-Directed Therapy (EGDT) Continuous ScvO2 monitoring & tx with fluids, blood, inotropes &/or vasoactives to maintain: ScvO2 >70%, SaO2 > 93%, Hct > 30%, CI/VO2 CVP > 8-12 MAP > 65 UO > .5ml/kg/hr Standard Therapy CVP > 8-12 MAP > 65 UO > .5ml/kg/hr Rivers et. al. N Engl J Med. 2001;345;19:
 Continuous ScvO2 monitoring & tx with fluids, blood, inotropes &/or vasoactives to maintain: ScvO2 >70%, SaO2 > 93%, Hct > 30%, CI/VO2. CVP > MAP > 65. UO > .5ml/kg/hr. Standard Therapy. CVP > MAP > 65. UO > .5ml/kg/hr. Rivers et. al. N Engl J Med. 2001;345;19:")
70
Early Goal-Directed Therapy Results
28-day Mortality NNT = 7-8 60 49.2% P = 0.01* 50 40 33.3% 30 20 10 Cause of in-hospital death: --Sudden Cardiovascular collapse Standard Tx= 25/119 (21%) EGDT 12/117 (10.3%) --MODS Standard Tx 26/119(21.8%) EGDT 19/117 (16.2%) P in New England Journal of Medicine Standard Therapy n=133 EGDT n=130 *Key difference was in sudden CV collapse, not MODS Rivers E. N Engl J Med 2001;345:
 EGDT 12/117 (10.3%) --MODS. Standard Tx 26/119(21.8%) EGDT 19/117 (16.2%) P in New England Journal of Medicine. Standard Therapy. n=133. EGDT. n=130. *Key difference was in sudden CV collapse, not MODS. Rivers E. N Engl J Med 2001;345:")
71
Evidence of Early Goal Directed Therapy
First 6 hours of EGDT: 1500cc more fluid 64% received blood products vs. 18.5% 13.7% received inotropes vs. 0.8% No difference in vasopressor use or mechanical ventilation Rivers et. al. N Engl J Med. 2001;345;19:

72
Dellinger, et. al. Crit Care Med 2008, 36:296-327.
Initial Resuscitation (1C) Protocolized resuscitation should begin as soon as sepsis induced tissue hypoperfusion is recognized or Elevated Serum lactate identifies tissue hypoperfusion in patients at risk who are not hypotensive Initial fluid challenges be started at > 1000 mL/kg or mL of colloid over 30 minutes (1C) - “Establishing vascular access and initiating aggressive fluid resuscitation is the first priority when managing patients with severe sepsis or septic shock.” p. 860 Resuscitation should begin as soon as severe sepsis or sepsis-induced tissue hypoperfusion [hypotension or lactic acidosis] is recognized and should not be delayed pending ICU admission. Elevated serum lactate concentration identifies tissue hypoperfusion in patients at risk who are not hypotensive. Lactate measurement lacks precision as a measure of tissue metabolic status. Central venous and mixed venous oxygen saturation are equivalent. In mechanically ventilated patients a higher target central venous pressure mm Hg is recommended to account for the increased intrathoracic pressure. Decrease in pulse is a useful marker of improving intravascular filling. The consensus panel judged central venous (superior vena cava) and mixed venous oxygenation to be equivalent. Rationale for this recommendation is based on Manny River’s protocol published in NEJM. This protocol was associated with an improvement in survival. NOTE: The references listed in the right hand corner of the slide relate to recommendations on the slide. When the slides are viewed in the “show” mode, clicking on the reference will automatically take you to an abstract of the specific study (this is only if your computer is connected to the internet and has access to Pubmed.) Dellinger, et. al. Crit Care Med 2008, 36: Rivers E. N Engl J Med 2001;345:
 Protocolized resuscitation should begin as soon as sepsis induced tissue hypoperfusion is recognized. or. Elevated Serum lactate identifies tissue hypoperfusion in patients at risk who are not hypotensive. Initial fluid challenges be started at > 1000 mL/kg or mL of colloid over 30 minutes (1C) - Establishing vascular access and initiating aggressive fluid resuscitation is the first priority when managing patients with severe sepsis or septic shock. p Resuscitation should begin as soon as severe sepsis or sepsis-induced tissue hypoperfusion [hypotension or lactic acidosis] is recognized and should not be delayed pending ICU admission. Elevated serum lactate concentration identifies tissue hypoperfusion in patients at risk who are not hypotensive. Lactate measurement lacks precision as a measure of tissue metabolic status. Central venous and mixed venous oxygen saturation are equivalent. In mechanically ventilated patients a higher target central venous pressure mm Hg is recommended to account for the increased intrathoracic pressure. Decrease in pulse is a useful marker of improving intravascular filling. The consensus panel judged central venous (superior vena cava) and mixed venous oxygenation to be equivalent. Rationale for this recommendation is based on Manny River’s protocol published in NEJM. This protocol was associated with an improvement in survival. NOTE: The references listed in the right hand corner of the slide relate to recommendations on the slide. When the slides are viewed in the show mode, clicking on the reference will automatically take you to an abstract of the specific study (this is only if your computer is connected to the internet and has access to Pubmed.) Dellinger, et. al. Crit Care Med 2008, 36: Rivers E. N Engl J Med 2001;345:")
73
Early Goal-Directed Therapy: SSC Recommendations
Goals of therapy within first 6 hours are: (1C) Central Venous Pressure mmHg Mean arterial pressure 65 mmHg Urine output 0.5 mL/kg/hr ScvO2 70%; if not achieved with fluid resuscitation during first 6 hours (2C) - Transfuse PRBC to hematocrit >27% and/or - Administer dobutamine (max 20 mcg/kg/min) to goal Dellinger RP, et al. Crit Care Med. 2008;36:
 Central Venous Pressure mmHg. Mean arterial pressure 65 mmHg. Urine output 0.5 mL/kg/hr. ScvO2 70%; if not achieved with fluid resuscitation during first 6 hours (2C) - Transfuse PRBC to hematocrit >27% and/or. - Administer dobutamine (max 20 mcg/kg/min) to goal. Dellinger RP, et al. Crit Care Med. 2008;36:")
74
Potential Emergency Department Challenges
Screening in Triage Drawing lactic acid level with less than one hour turn around time When and who will place the central line? Physician skill level ? Monitoring CVPs and ScvO2-nurses skill level and available resources? When to transfer to ICU? ED-ICU handoff If long ED LOS---does the ED implement both resuscitation and management bundles

75
EGDT: Revisited 20.3% Reduction in Mortality, NNT 5
Outcomes Survey: 12 programs 1,298 patients with severe sepsis and septic shock Treated with EGDT and/or the sepsis bundles Pre implementation mortality: % Post implementation mortality: % 20.3% Reduction in Mortality, NNT 5 Otero RM. et al Chest; 2006:130:

76
EGDT: Revisited Cost Effectiveness of EGDT/Guideline Based Care (ED, ICU or RRT initiated) 23.4% reduction in hospital cost (incorporated additional training, personnel and equipment) Huang et al Crit Care Med 2003:7(suppl S116) Henry Ford Hospital: 4 day Hospital LOS (32.6% reduction) Reduction in hospital charges from $135,199 to $82,233 (39.2% reduction) Trzeciak S et al, Chest 2006:129: Otero RM. et al Chest; 2006:130:
 Huang et al Crit Care Med 2003:7(suppl S116) Henry Ford Hospital: 4 day Hospital LOS (32.6% reduction) Reduction in hospital charges from $135,199 to $82,233 (39.2% reduction) Trzeciak S et al, Chest 2006:129: Otero RM. et al Chest; 2006:130:")
78
Peer Review Publications
Favors No EGDT Favors EGDT Before 1104 After 1175 78 78

79
Abstracts and Publications
3311 Before 3223 After 79 79

80
Abstracts and Publications
1 of every 6 Patients 4125 Before 3328 After 80 80

81
Vasopressors Recommend that MAP be maintain > 65 mmhg (1C)
Ideally adequate fluid resuscitation should be achieved before vasopressors and inotropes are used, but use early in septic shock may need to occur. When it does the goal should be to try and wean with continuing fluid resuscitation. Norepinephrine or dopamine as first choice. (1C) Epinephrine, phenylephrine or vasopression should not be used as the initial vasopressor. (2C) Vasopresion may be added to norepinephrine at 0.03 units/min. Suggest that epinephrine be the first chosen alternative. (2B) Low dose dopamine not be used for renal perfusion. (1A) Dellinger RP, et al. Crit Care Med. 2008;36:
 Epinephrine, phenylephrine or vasopression should not be used as the initial vasopressor. (2C) Vasopresion may be added to norepinephrine at 0.03 units/min. Suggest that epinephrine be the first chosen alternative. (2B) Low dose dopamine not be used for renal perfusion. (1A) Dellinger RP, et al. Crit Care Med. 2008;36:")
82
Vasopressin vs Norepinephrine Infusion in Septic Shock VASST Study
Design: Multicenter, randomized, double-blinded Population: 778 patients with septic shock and were receiving a minimum of 5mcq/min of norephinephrine (or equivalent) for 6 hours (excluded pts with underlying heart disease) Methods: Received either low dose vasopressin ( U per minutes) or norepinephrine in addition to open-label vasopressors End point: 28 day mortality Russell et al NEJM, 2008; Vol. 58, No 9
 for 6 hours (excluded pts with underlying heart disease) Methods: Received either low dose vasopressin ( U per minutes) or norepinephrine in addition to open-label vasopressors. End point: 28 day mortality. Russell et al NEJM, 2008; Vol. 58, No 9.")
83
VASST Study Results No significant difference in 28 day or 90 day mortality between the two groups Among patients who had less severe septic shock(on norepinephrine between 5-15 mcq/min) there was a trend toward improved mortality with vasopressin (hypothesis generating) No significant difference in rates of organ dsyfunction between the two groups No significant difference in overall rates of serious adverse events between the two groups Trend toward higher rate of cardiac arrest in norepinephrine group Trend toward higher rate of digital ischemia in the vasopressin group Russell et al NEJM, 2008; Vol. 58, No 9
 there was a trend toward improved mortality with vasopressin (hypothesis generating) No significant difference in rates of organ dsyfunction between the two groups. No significant difference in overall rates of serious adverse events between the two groups. Trend toward higher rate of cardiac arrest in norepinephrine group. Trend toward higher rate of digital ischemia in the vasopressin group. Russell et al NEJM, 2008; Vol. 58, No 9.")
84
Additional Findings Vasopressin infusion allowed a rapid decrease in the total norepinephrine dose while maintaining mean arterial pressure Overall rates of serious adverse events were approximately 10% each in the vasopressin and norepinephrine groups. The MAP at baseline was 72-73mmHg—essentially making this a study of the effects of low dose vasopressin as a “catecholamine-sparing drug” not an evaluation of vasopressin in patients with catecholamine-unresponsive refractory shock Russell et al NEJM, 2008; Vol. 58, No 9

85
ICU/Additional Evidence
EARLY MANAGEMENT Early Recognition Early Antibiotics Prompt/Aggressive Resuscitation ICU/Additional Evidence Based Therapies

86
Dellinger, et. al. Crit Care Med 2008, 36: 296-327.
Antibiotic Therapy Start intravenous antibiotic therapy within the first hour of recognition of severe sepsis after obtaining appropriate cultures (1D) for Septic shock (1B) Board spectrum: include one or more agents active against likely bacterial/fungal pathogens, & with good penetration into presumed source (1B) Reassess regimen daily to optimize efficacy, prevent resistance, avoid toxicity & minimize costs. (1C) May require additional vascular access ports An empirical antimicrobial regimen should have coverage for all likely pathogens since there is little margin for error in critically ill patients. Failure to initiate appropriate therapy promptly has adverse consequences on outcomes. Once the organism and its susceptibilities have been defined narrowing the spectrum of antibiotics reduces the risk of resistance, superinfections and costs. Due to renal and hepatic dysfunction in severe sepsis patients and due to the altered volume of distribution, it is recommended to involve the ICU pharmacist to ensure serum concentrations are attained that maximize efficacy and minimize toxicity. “Establishing vascular access and initiating aggressive fluid resuscitation is the first priority when managing patients with severe sepsis or septic shock. (p. 860) However, prompt infusion of antimicrobial agents is also a logical strategy and may require additional access ports.” Kreger BE. Am J Med 1980;68: Ibrahim EH. Chest 2000;118: Hatala R. Ann Intern Med 1996; Dellinger, et. al. Crit Care Med 2008, 36:
 for Septic shock (1B) Board spectrum: include one or more agents active against likely bacterial/fungal pathogens, & with good penetration into presumed source (1B) Reassess regimen daily to optimize efficacy, prevent resistance, avoid toxicity & minimize costs. (1C) May require additional vascular access ports. An empirical antimicrobial regimen should have coverage for all likely pathogens since there is little margin for error in critically ill patients. Failure to initiate appropriate therapy promptly has adverse consequences on outcomes. Once the organism and its susceptibilities have been defined narrowing the spectrum of antibiotics reduces the risk of resistance, superinfections and costs. Due to renal and hepatic dysfunction in severe sepsis patients and due to the altered volume of distribution, it is recommended to involve the ICU pharmacist to ensure serum concentrations are attained that maximize efficacy and minimize toxicity. Establishing vascular access and initiating aggressive fluid resuscitation is the first priority when managing patients with severe sepsis or septic shock. (p. 860) However, prompt infusion of antimicrobial agents is also a logical strategy and may require additional access ports. Kreger BE. Am J Med 1980;68: Ibrahim EH. Chest 2000;118: Hatala R. Ann Intern Med 1996; Dellinger, et. al. Crit Care Med 2008, 36:")
87
Mortality as a Function of Adequacy of Empiric Antimicrobial Therapy
Hospital Mortality (%) All causes Infection-related P<0.001 Inadequate Therapy Adequate Therapy 60 50 40 30 20 10 The relationship between inadequate antimicrobial treatment of infections (both community-acquired and nosocomial infections) and hospital mortality for patients requiring ICU admission was studied by Kollef et al in a prospective cohort study of 2000 consecutive patients requiring admission to the medical or surgical ICU. One hundred sixty-nine (8.5%) infected patients received inadequate antimicrobial treatment of their infections. This represented 25.8% of the 655 patients assessed to have either community-acquired or nosocomial infections. The occurrence of inadequate antimicrobial treatment of infection was most common among patients with nosocomial infections. The infection-related mortality rate for infected patients receiving inadequate antimicrobial treatment (42.0%) was significantly greater than the infection-related mortality rate of infected patients receiving adequate antimicrobial treatment (17.7%) (relative risk [RR], 2.37; 95% confidence interval [CI], 1.83 to 3.08; P<0.001). Using a logistic regression model, inadequate antimicrobial treatment of infection was found to be the most important independent determinant of hospital mortality for the entire patient cohort (adjusted odds ratio [OR], 4.27; 95% CI, 3.35 to 5.44; P<0.001). Kollef MH, Sherman G, Ward S, et al. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest 1999;115: Kollef MH, et al. Chest 1999;115:
 All causes. Infection-related. P< Inadequate Therapy. Adequate Therapy The relationship between inadequate antimicrobial treatment of infections (both community-acquired and nosocomial infections) and hospital mortality for patients requiring ICU admission was studied by Kollef et al in a prospective cohort study of 2000 consecutive patients requiring admission to the medical or surgical ICU. One hundred sixty-nine (8.5%) infected patients received inadequate antimicrobial treatment of their infections. This represented 25.8% of the 655 patients assessed to have either community-acquired or nosocomial infections. The occurrence of inadequate antimicrobial treatment of infection was most common among patients with nosocomial infections. The infection-related mortality rate for infected patients receiving inadequate antimicrobial treatment (42.0%) was significantly greater than the infection-related mortality rate of infected patients receiving adequate antimicrobial treatment (17.7%) (relative risk [RR], 2.37; 95% confidence interval [CI], 1.83 to 3.08; P<0.001). Using a logistic regression model, inadequate antimicrobial treatment of infection was found to be the most important independent determinant of hospital mortality for the entire patient cohort (adjusted odds ratio [OR], 4.27; 95% CI, 3.35 to 5.44; P<0.001). Kollef MH, Sherman G, Ward S, et al. Inadequate antimicrobial treatment of infections: a risk factor for hospital mortality among critically ill patients. Chest 1999;115: Kollef MH, et al. Chest 1999;115:")
88
Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock *Effective antimicrobial administration within the 1st hour of documented hypotension was associated with increased survival in patients with septic shock. *Each hour of delay over the next 6 hours was associated with an average decrease in survival of 7.6% (range %) CCM 2006 Vol. 34 No.6
 CCM 2006 Vol. 34 No.6.")
89
Antibiotic Challenges
Appropriate selection – determined based upon consensus guidelines and pathogen sensitivity at your institution Timing issues How? Delivery time challenges of antibiotics Possible solutions

90
Case Study Disclaimer: This is intended for education purposes
Judgment of physician/clinician should always be the deciding factor The following case represents individual experience that are specific to these patients and may not reflect the typical course of recovery

91
Clinical Scenario 2 : Early Identification and Intervention
88 year old, 51.6kg,white, female presented to ED at 1345 from ECF History: CAD, COPD, dementia, Alzheimer disease, depression, SVT Chief Complaint: rib pain, chest congestion and SOB Awake, alert and oriented, slight combative (history of combative behavior)
")
92
Case Study 2: Early Identification and Intervention
Initial VS: Temp: F RR: 31 HR: 109, atrial fib with occasional SVT B/P: 79/51 2L of O2, O2 sat of 96% Positive Screen for severe sepsis: SIRS: HR >90; RR> 20; Temp > 38 Organ dysfunction: SBP<90mmHg Early Treatment IV started Received 500cc NS bolus over 30 minutes Labs drawn

93
Advanced Treatment Guidelines Department of Emergency Services
PURPOSE: To provide prompt, consistent nursing interventions for the patient with SIRS or sepsis prior to physician evaluation, to enable rapid diagnosis and slow the progression of illness. IMPLEMENTATION: The nursing staff may implement these interventions for patients who present with all three of the following criteria. The nurse should take into consideration the patient’s baseline vital signs when evaluating as a potential candidate. Also, these interventions should not conflict with the patient/family goals. (i.e. DNR, comfort care) 1. Clinical suspicion of systemic infection 2. At least two of the following: Hyperthermia :Temperature greater than 38 °C (100.4 °F) Hypothermia: Temperature less than < 36 °C (96.8 °F) Tachycardia Pulse > 90 bpm Tachypnea RR > 20 3. SBP < 90 Patients who meet all three criteria will be placed in a room immediately after consultation with charge nurse and/or attending.
 1. Clinical suspicion of systemic infection. 2. At least two of the following: Hyperthermia :Temperature greater than 38 °C (100.4 °F) Hypothermia: Temperature less than < 36 °C (96.8 °F) Tachycardia Pulse > 90 bpm. Tachypnea RR > SBP < 90 Patients who meet all three criteria will be placed in a room immediately after consultation with charge nurse and/or attending.")
94
Advanced Treatment Guidelines Department of Emergency Services
Notify Physician Place Intermittent Infusion Device (large bore catheter) in 2 sites Place on cardiac monitor Continuous pulse oximetry Vital signs every 15 minutes Administer oxygen at 2 L/min per nasal cannula if O2 sat <92% Draw and hold blood cultures x 2, Type & screen Draw tube for serum lactate and place on ice. Collect CCMS urine sample in the non-menstruating patient. Send for Urinalysis and urine culture. Portable CXR Intravenous hydration: Administer 500ml bolus of normal saline over 15 minutes.
 in 2 sites. Place on cardiac monitor. Continuous pulse oximetry. Vital signs every 15 minutes. Administer oxygen at 2 L/min per nasal cannula if O2 sat <92% Draw and hold blood cultures x 2, Type & screen. Draw tube for serum lactate and place on ice. Collect CCMS urine sample in the non-menstruating patient. Send for Urinalysis and urine culture. Portable CXR. Intravenous hydration: Administer 500ml bolus of normal saline over 15 minutes.")
95
Case Study 2: Early Identification and Intervention
Labs: WBC: 11.5 Hgb: 15.8 Hct: 47.4 BUN: 28 Creatinine:1.6 Glucose:158 BNP:78 (moderate CHF); troponin:0.03 Lactic acid: 4.6 U/A: positive for bacteria ScvO2: 49.1% Blood cultures X 2 drawn
; troponin:0.03. Lactic acid: 4.6. U/A: positive for bacteria. ScvO2: 49.1% Blood cultures X 2 drawn.")
96
Case Study 2: Early Identification and Intervention
CXR: RLL consolidation Additional Interventions: Broad spectrum antibiotics given within 3 hours of presentation Lactic acid >4mmol/L so CVP inserted Fluid resuscitation continued Foley inserted Received total of 3 Liters of NS during 3 hour ED stay ED diagnosis: Severe sepsis, Pneumonia , UTI, CHF Transferred to MICU

97
Case Study 2 : Early Identification and Intervention--MICU
Additional Interventions: Day 1 Continued fluid resuscitation—7 L Low dose vasopressor Low dose steroids Remained on 2 L nasal canula Not eligible for Xigris (renal failure resolved and vasopressor weaned off within 12hours after ICU admission) Labs: ScvO2: 72.8 (after resuscitation) Lactic acid: 4 hours after ICU admission: 6.7 12 hours after ICU admission: 3.0 Bleeding is most common adverse effect associated with Xigris therapy, please see important safety information in this presentation
 Labs: ScvO2: 72.8 (after resuscitation) Lactic acid: 4 hours after ICU admission: hours after ICU admission: 3.0. Bleeding is most common adverse effect associated with Xigris therapy, please see important safety information in this presentation.")
98
Case Study 2: Early Identification and Intervention
Day 2: Vasopressor weaned off Lasix to assist with fluid mobilization Lactic acid: 3.0 Day 3: Lactic acid: 1.2 O2 sat 93% on room air Central line discontinued Transferred to intermediate care on Day 3 Discharged from hospital on day 7

99
ICU/Additional Evidence
EARLY MANAGEMENT Early Recognition Early Antibiotics Prompt/Aggressive Resuscitation ICU/Additional Evidence Based Therapies

100
Management Bundle Components

101
Recombinant human Activated Protein C (2B)
Recombinant human Activated Protein C [Drotrecogin alfa (activated)] is recommended in patients at a high risk of death (APACHE II score 25, or Sepsis-induced multiple organ failure) if there are no contraindications. Within 30 days of surgery with the above indications (2C) Drotrecogin alfa (activated) is not indicated in adult patients with severe sepsis and lower risk of death. (1A) Relative contraindications/warnings should be consider “The inflammatory response in severe sepsis is integrally linked to procoagulant activity and endothelial activation.” p. 863. “The inflammatory response in sepsis is procoagulant in the early stages.” P. 863 rhAPC [drotrecogin alfa (activated)] has been shown, in a large, multiple center, randomized, controlled trial to improve survival in patients with sepsis-induced organ dysfunction.” p. 863. “At present, risk assessment is best determined by bedside clinical evaluation and judgment. Given the uncertainty of risk assessment and the potential for rapid deterioration of patients with severe sepsis and septic shock, once a patient has been identified as at high risk of death, treatment should begin as soon as possible.” p. 863 Dellinger, et. al. Crit Care Med 2008, 36:
] is recommended in patients at a high risk of death (APACHE II score 25, or Sepsis-induced multiple organ failure) if there are no contraindications. Within 30 days of surgery with the above indications (2C) Drotrecogin alfa (activated) is not indicated in adult patients with severe sepsis and lower risk of death. (1A) Relative contraindications/warnings should be consider. The inflammatory response in severe sepsis is integrally linked to procoagulant activity and endothelial activation. p The inflammatory response in sepsis is procoagulant in the early stages. P rhAPC [drotrecogin alfa (activated)] has been shown, in a large, multiple center, randomized, controlled trial to improve survival in patients with sepsis-induced organ dysfunction. p At present, risk assessment is best determined by bedside clinical evaluation and judgment. Given the uncertainty of risk assessment and the potential for rapid deterioration of patients with severe sepsis and septic shock, once a patient has been identified as at high risk of death, treatment should begin as soon as possible. p Dellinger, et. al. Crit Care Med 2008, 36:")
102
Drotrecogin Alfa (Activated) In Severe Sepsis: PROWESS Results
PROWESS 28-Day Mortality – High Risk of Death Patients* 29% reduction in relative risk of death with Xigris† Absolute Risk Reduction = 13% Mortality Rate This illustrates mortality differences between placebo and drotrecogin alfa activated groups over a 28 day period. 13% more survivors in the drotrecogin alfa (activated) treatment group at 28 days (absolute risk reduction of 13 %). These data represent the indicated population (those patients with high risk of death severe sepsis. High risk of death as defined by an APACHE II score greater than or equal to 25 at baseline enrollment to the PROWESS study). *as defined by APACHE II 25 †relative risk reduction at 28 days Data on file, Eli Lilly and Company. Placebo Drotrecogin alfa (activated) See important safety information in this presentation.
 treatment group at 28 days (absolute risk reduction of 13 %). These data represent the indicated population (those patients with high risk of death severe sepsis. High risk of death as defined by an APACHE II score greater than or equal to 25 at baseline enrollment to the PROWESS study). *as defined by APACHE II 25. †relative risk reduction at 28 days. Data on file, Eli Lilly and Company. Placebo. Drotrecogin alfa (activated) See important safety information in this presentation.")
103
Survival Benefit Consistent across High-risk Severe Sepsis Patients
Xigris® (drotrecogin alfa [activated]) benefits consistent 28-DAY MORTALITY FAVORS XIGRIS FAVORS PLACEBO TOTAL RELATIVE RISK XIGRIS PLACEBO (CONFIDENCE INTERVAL) APACHE II* ≥ ( ) ORGAN DYSFUNCTION ≥ ( ) CAP WITH APACHE II ≥ ( ) CAP S. PNEUMONIAE ( ) WITH APACHE II ≥ 254 INTRA-ABDOMINAL SURGERY ( ) WITH APACHE II ≥ 251 OVERT DIC ( ) 0.0 Relative Risk of Death (95% CI) The 95% relative risk confidence interval for each subgroup included the point estimate for the overall PROWESS population (0.80). The point estimate of relative risk of death in each subgroup is indicated by a solid circle, and the 95% confidence interval is indicated by the horizontal lines. Note the consistency between the overall trial result and the subgroup analyses. *APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please see †Nonprospectively defined population 1. Barie P, et al. Am J Surg. 2004; 188: Dhainaut JF MD, PhD, et al. For the PROWESS Study Group. Intensive Care Med. 2003;29(6): Laterre P-F et al. Crit Care Med. 2005;33(5): Data on file, Eli Lilly and Company. 6. Dhainaut JF, Yan SB, Joyce DE, et al. J Thromb Haemost 2004; 2: See Important Safety Information in this presentation. 6
 benefits consistent. 28-DAY MORTALITY. FAVORS XIGRIS FAVORS PLACEBO TOTAL RELATIVE RISK XIGRIS PLACEBO (CONFIDENCE INTERVAL) APACHE II* ≥ ( ) ORGAN DYSFUNCTION ≥ ( ) CAP WITH APACHE II ≥ ( ) CAP S. PNEUMONIAE ( ) WITH APACHE II ≥ 254. INTRA-ABDOMINAL SURGERY ( ) WITH APACHE II ≥ 251. OVERT DIC ( ) Relative Risk of Death (95% CI) The 95% relative risk confidence interval for each subgroup included the point estimate for the overall PROWESS population (0.80). The point estimate of relative risk of death in each subgroup is indicated by a solid circle, and the 95% confidence interval is indicated by the horizontal lines. Note the consistency between the overall trial result and the subgroup analyses. *APACHE (Acute Physiology And Chronic Health Evaluation). For more information on using the APACHE II scoring system, please see †Nonprospectively defined population 1. Barie P, et al. Am J Surg. 2004; 188: Dhainaut JF MD, PhD, et al. For the PROWESS Study Group. Intensive Care Med. 2003;29(6): Laterre P-F et al. Crit Care Med. 2005;33(5): Data on file, Eli Lilly and Company. 6. Dhainaut JF, Yan SB, Joyce DE, et al. J Thromb Haemost 2004; 2: See Important Safety Information in this presentation. 6.")
104
RESPOND Targeted Enrollment = 500 Enrollment started in Nov. 2006
Fine-Tuning Xigris Therapy in Adult High-Risk Severe Sepsis Patients Right Patient, Right Drug, Right Time New: Clinical trials to help advance care of adult patients with severe sepsis at high risk of death: RESPOND Targeted Enrollment = Enrollment started in Nov. 2006 Phase 2 trial investigating a biomarker (Protein C) to help guide Xigris therapy in adult patients with severe sepsis at high risk of death. NEW Placebo Controlled Trial in Adult High-Risk Severe Sepsis Help clinicians better identify patients who are most likely to benefit from Xigris, as well as to further clarify the benefit/risk profile of the drug. Lilly is committed to helping clinicians answer the important question of what patient type will most benefit from Xigris therapy. To that end, Lilly is undertaking 2 additional clinical trials to help advance the care of adult patients with severe sepsis at high risk of death and are intended to bring precision to the clinician’s use of Xigris within the indicated (adult patients with severe sepsis at high risk of death) population. RESPOND, which was initiated in November 2006, is a phase 2 trial investigating a biomarker (Protein C) to help clinicians tailor Xigris therapy in adult patients with severe sepsis at high risk of death. The new placebo-controlled trial will help clinicians better identify patients who are most likely to benefit from Xigris, as well as to further clarify the benefit/risk profile of the drug. The placebo-controlled trial will have a primary endpoint of 28-day all-cause mortality. It is currently being designed and may begin enrollment in early 2008. You may contact LILLY-RX to receive additional information upon request. Contact LILLY-RX for more information. Bleeding is the most common adverse effect associated with Xigris therapy. Please see Important Safety Information in this presentation and accompanying full Prescribing Information.
 to help guide Xigris therapy in adult patients with severe sepsis at high risk of death. NEW Placebo Controlled Trial in Adult High-Risk Severe Sepsis. Help clinicians better identify patients who are most likely to benefit from Xigris, as well as to further clarify the benefit/risk profile of the drug. Lilly is committed to helping clinicians answer the important question of what patient type will most benefit from Xigris therapy. To that end, Lilly is undertaking 2 additional clinical trials to help advance the care of adult patients with severe sepsis at high risk of death and are intended to bring precision to the clinician’s use of Xigris within the indicated (adult patients with severe sepsis at high risk of death) population. RESPOND, which was initiated in November 2006, is a phase 2 trial investigating a biomarker (Protein C) to help clinicians tailor Xigris therapy in adult patients with severe sepsis at high risk of death. The new placebo-controlled trial will help clinicians better identify patients who are most likely to benefit from Xigris, as well as to further clarify the benefit/risk profile of the drug. The placebo-controlled trial will have a primary endpoint of 28-day all-cause mortality. It is currently being designed and may begin enrollment in early You may contact LILLY-RX to receive additional information upon request. Contact LILLY-RX for more information. Bleeding is the most common adverse effect associated with Xigris therapy. Please see Important Safety Information in this presentation and accompanying full Prescribing Information.")
105
What are the Challenges to Appropriate Screening and Administration of Xigris® (drotrecogin alfa [activated])? Concerns about risk of bleeding Restrictive order set Inconsistent screening process Cost issues
![What are the Challenges to Appropriate Screening and Administration of Xigris® (drotrecogin alfa [activated])](http://slideplayer.com/slide/4002936/13/images/105/What+are+the+Challenges+to+Appropriate+Screening+and+Administration+of+Xigris%C2%AE+%28drotrecogin+alfa+%5Bactivated%5D%29.jpg "Concerns about risk of bleeding. Restrictive order set. Inconsistent screening process. Cost issues.")
106
Safety Profile Low incidence of serious bleeding events*
Rate of serious bleeding events during infusion in high-risk patients: PROWESS: 2.2% (9 of 414) in drotrecogin alfa (activated) patients vs 0.7% (3 of 403) in standard therapy patients Rate of ICH in high-risk patients during infusion: PROWESS: 0.2% (1 of 414) in drotrecogin alfa (activated) patients Associated with severe thrombocytopenia (platelet count < 30,000/mm3)† Not associated with other adverse events *Serious bleeding events were defined as any intracranial hemorrhage, any life-threatening bleeding, any bleeding event requiring the administration of ≥3 units of packed red blood cells per day for 2 consecutive days, or any bleeding event assessed as a serious adverse event. †At the time of enrollment in the PROWESS study, the patient had a platelet count above 30,000/mm3. The patient’s platelet count fell to less than 30,000/mm3 after drotrecogin alfa (activated) therapy was initiated. Data on file, Eli Lilly and Company See important safety information and full prescribing information in this presentation.
 in drotrecogin alfa (activated) patients vs 0.7% (3 of 403) in standard therapy patients. Rate of ICH in high-risk patients during infusion: PROWESS: 0.2% (1 of 414) in drotrecogin alfa (activated) patients. Associated with severe thrombocytopenia (platelet count < 30,000/mm3)† Not associated with other adverse events. *Serious bleeding events were defined as any intracranial hemorrhage, any life-threatening bleeding, any bleeding event requiring the administration of ≥3 units of packed red blood cells per day for 2 consecutive days, or any bleeding event assessed as a serious adverse event. †At the time of enrollment in the PROWESS study, the patient had a platelet count above 30,000/mm3. The patient’s platelet count fell to less than 30,000/mm3 after drotrecogin alfa (activated) therapy was initiated. Data on file, Eli Lilly and Company. See important safety information and full prescribing information in this presentation.")
107
Drotrecogin Alfa (Activated) Has a Favorable Risk/Benefit Profile
8 times more likely to save an additional life than observe an additional serious bleeding event * • Rate of serious bleeding events attributable to Xigris during infusion was limited to 1.5%. • This increase, compared against the mortality reduction, means that physicians were 8 times more likely to save an additional life than observe an additional serious bleeding event. * Based on a 13% 28-day survival benefit and a serious bleeding rate during infusion attributable to Xigris of 1.5% (13% ÷ 1.5% = 8.7) in patients with an APACHE II score > 25. Data on file, Eli Lilly and Company.
 in patients with an APACHE II score > 25. Data on file, Eli Lilly and Company.")
108
Important Safety Information
CONTRAINDICATIONS Drotrecogin alfa (activated) increases the risk of bleeding. Drotrecogin alfa (activated) is contraindicated in patients with the following clinical situations in which bleeding could be associated with a high risk of death or significant morbidity. Active internal bleeding Recent (within 3 months) hemorrhagic stroke Recent (within 2 months) intracranial or intraspinal surgery, or severe head trauma Trauma with an increased risk of life-threatening bleeding Presence of an epidural catheter Intracranial neoplasm or mass lesion or evidence of cerebral herniation Drotrecogin alfa (activated) is contraindicated in patients with known hypersensitivity to drotrecogin alfa (activated) or any component of this product. See full Prescribing Information available at this presentation.
 increases the risk of bleeding. Drotrecogin alfa (activated) is contraindicated in patients with the following clinical situations in which bleeding could be associated with a high risk of death or significant morbidity. Active internal bleeding. Recent (within 3 months) hemorrhagic stroke. Recent (within 2 months) intracranial or intraspinal surgery, or severe head trauma. Trauma with an increased risk of life-threatening bleeding. Presence of an epidural catheter. Intracranial neoplasm or mass lesion or evidence of cerebral herniation. Drotrecogin alfa (activated) is contraindicated in patients with known hypersensitivity to drotrecogin alfa (activated) or any component of this product. See full Prescribing Information available at this presentation.")
109
Important Safety Information WARNINGS
Bleeding Bleeding is the most common serious adverse effect associated with drotrecogin alfa (activated) therapy. Each patient being considered for therapy with drotrecogin alfa (activated) should be carefully evaluated and anticipated benefits weighed against potential risks associated with therapy Certain conditions, many of which led to exclusion from the Phase 3 trial, are likely to increase the risk of bleeding with drotrecogin alfa (activated) therapy. For individuals with one or more of the following conditions, the increased risk of bleeding should be carefully considered when deciding whether to use drotrecogin alfa (activated) therapy: Concurrent therapeutic dosing of heparin to treat an active thrombotic or embolic event Platelet count < 30,000 x 106/L, even if the platelet count is increased after transfusions Prothrombin time-INR > 3.0 Recent (within 6 weeks) gastrointestinal bleeding Recent administration (within 3 days) of thrombolytic therapy Recent administration (within 7 days) of oral anticoagulants or glycoprotein IIb/IIIa inhibitors Recent administration (within 7 days) of aspirin > 650 mg per day or other platelet inhibitors Recent (within 3 months) ischemic stroke Intracranial arteriovenous malformation or aneurysm Known bleeding diathesis Chronic severe hepatic disease Any other condition in which bleeding constitutes a significant hazard or would be particularly difficult to manage because of its location See full Prescribing Information available at this presentation.
 therapy. Each patient being considered for therapy with drotrecogin alfa (activated) should be carefully evaluated and anticipated benefits weighed against potential risks associated with therapy. Certain conditions, many of which led to exclusion from the Phase 3 trial, are likely to increase the risk of bleeding with drotrecogin alfa (activated) therapy. For individuals with one or more of the following conditions, the increased risk of bleeding should be carefully considered when deciding whether to use drotrecogin alfa (activated) therapy: Concurrent therapeutic dosing of heparin to treat an active thrombotic or embolic event. Platelet count < 30,000 x 106/L, even if the platelet count is increased after transfusions. Prothrombin time-INR > 3.0. Recent (within 6 weeks) gastrointestinal bleeding. Recent administration (within 3 days) of thrombolytic therapy. Recent administration (within 7 days) of oral anticoagulants or glycoprotein IIb/IIIa inhibitors. Recent administration (within 7 days) of aspirin > 650 mg per day or other platelet inhibitors. Recent (within 3 months) ischemic stroke. Intracranial arteriovenous malformation or aneurysm. Known bleeding diathesis. Chronic severe hepatic disease. Any other condition in which bleeding constitutes a significant hazard or would be particularly difficult to manage because of its location. See full Prescribing Information available at this presentation.")
110
Additional Management Bundle Components

111
Low Tidal Volume Ventilation: SSC Recommendations
Target tidal volumes to < 6 mL/kg (predicted body weight) in patients with ALI/ARDS (1B) Initial upper limit goal for plateau pressures in a passively inflated patient be < 30 cm H2O (1C) Hypercapnia can be tolerated in patients with ALI/ARDS if required to minimize plateau pressures and tidal volumes (1C) Recommend that positive end expiratory pressure be set as to avoid extensive lung collapse at end- expiration (1C) Suggest prone positioning in ARDS patients requiring potentially injurious levels of FiO2 or plateau pressures in facilities that have experience with the practice (2C) Dellinger RP, et al. Crit Care Med. 2008;36;
 in patients with ALI/ARDS (1B) Initial upper limit goal for plateau pressures in a passively inflated patient be < 30 cm H2O (1C) Hypercapnia can be tolerated in patients with ALI/ARDS if required to minimize plateau pressures and tidal volumes (1C) Recommend that positive end expiratory pressure be set as to avoid extensive lung collapse at end- expiration (1C) Suggest prone positioning in ARDS patients requiring potentially injurious levels of FiO2 or plateau pressures in facilities that have experience with the practice (2C) Dellinger RP, et al. Crit Care Med. 2008;36;")
112
ARDS Network ALI/ARDS Ventilator Study
Methodology: Inclusion criteria: p/f ratio < 300, bilateral infiltrates, no cardiac cause, receiving mechanical ventilation Outcomes: mortality/VFD 841 patients randomized 12 ml/kg TV group – Plat < 50 cm H2O 6 ml/kg TV group - Plat < 30 cm H2O ARDS Network, N Engl J Med 2000;342:

113
ARDS Network ALI/ARDS Ventilator Study
Results: PEEP: no difference in average amount used Mortality: 31% ( 6 ml/kg TV) vs. 40% (12 ml/kg TV) p=0.007 VFD: vs (p=0.007) Greater organ failure free days in protective group Reduction in IL-6 levels by day 3 Difficulty with agitation/high rates in the 6 ml/kg group ARDS Network, N Engl J Med 2000;342:
 vs. 40% (12 ml/kg TV) p= VFD: vs (p=0.007) Greater organ failure free days in protective group. Reduction in IL-6 levels by day 3. Difficulty with agitation/high rates in the 6 ml/kg group. ARDS Network, N Engl J Med 2000;342:")
114
Additional Mechanical Ventilation Recommendations
Unless contraindicated, maintain HOB elevated to limit aspiration and prevent VAP (1B). Elevation should be 30 to 45 degrees (2C) Non-invasive mask ventilation only be considered in that minority of mild to moderate hypoxemic respiratory failure patients who are able to protect their airway & are hemodynamically stable. A low threshold for intubation should be maintain (2B) Dellinger RP, et al. Crit Care Med. 2008;36;
. Elevation should be 30 to 45 degrees (2C) Non-invasive mask ventilation only be considered in that minority of mild to moderate hypoxemic respiratory failure patients who are able to protect their airway & are hemodynamically stable. A low threshold for intubation should be maintain (2B) Dellinger RP, et al. Crit Care Med. 2008;36;")
115
Additional Mechanical Ventilation Recommendations
Weaning protocol in place where patients undergo SBT if the satisfy criteria (1A) Recommend against the routine use of PA catheters (1A) Recommend a conservative fluid strategy for patients with established ALI/ARDS who do not have evidence of tissue hypoperfusion (1C) Dellinger RP, et al. Crit Care Med. 2008;36;
 Recommend against the routine use of PA catheters (1A) Recommend a conservative fluid strategy for patients with established ALI/ARDS who do not have evidence of tissue hypoperfusion (1C) Dellinger RP, et al. Crit Care Med. 2008;36;")
116
Corticosteroids In Septic Shock: SSC Recommendations (2C)
Intravenous corticosteroids should only be given to adult septic shock patients after it has been confirmed that their blood pressure is poorly responsive to fluid resuscitation and vasopressor therapy Suggest that the ACTH stimulation test should NOT BE used to identify the subset of adult with septic shock who should receive hydrocortisone. (2B) We suggest that patients with septic shock should not receive dexamethasone if hydrocortisone is available. (2B) Administer intravenous hydrocortisone <300 mg daily (1A) Fludrocortisone is optional if hydrocortisone is used (2C) Dellinger RP, et al. Crit Care Med. 2008;36:
 We suggest that patients with septic shock should not receive dexamethasone if hydrocortisone is available. (2B) Administer intravenous hydrocortisone <300 mg daily (1A) Fludrocortisone is optional if hydrocortisone is used (2C) Dellinger RP, et al. Crit Care Med. 2008;36:")
117
Hydrocortisone Therapy for Patients with Septic Shock
Design: Multicenter, randomized, double-blind, placebo-controlled trial Population: 499 patients with septic shock—BP<90 systolic despite adequate fluid replacement or vasopressors for at least one hour (onset of shock within previous 72 hrs) Method: 2 groups: one group received 50mg hydrocortisone every 6 hrs for 5 days, then tapered; other group received a placebo. End Point: 28 day mortality Sprung, NEJM,2008; Vol 358 No 2
 Method: 2 groups: one group received 50mg hydrocortisone every 6 hrs for 5 days, then tapered; other group received a placebo. End Point: 28 day mortality. Sprung, NEJM,2008; Vol 358 No 2.")
118
Hydrocortisone Therapy for Patients with Septic Shock--Results
No significant difference between 2 study groups in rate of death at 28 days (no matter if responded or not to corticotropin) Duration of time to reversal of shock was significantly shorter among all pts receiving hydrocortisone (3.3 days vs 5.8 days; p<0.001) Pts in this study who has a SBP of< 90mmHg at 1 day after fluid and vasopressor resuscitation had mortality of 56% if received placebo and mortality of 44.9 if received hydrocortisone (difference of 11.4%)—similar to Annane et al results. In hydrocortisone group there was an increased incidence of superinfections, including new episodes of septic shock Sprung, NEJM,2008; Vol 358 No 2
 Duration of time to reversal of shock was significantly shorter among all pts receiving hydrocortisone (3.3 days vs 5.8 days; p<0.001) Pts in this study who has a SBP of< 90mmHg at 1 day after fluid and vasopressor resuscitation had mortality of 56% if received placebo and mortality of 44.9 if received hydrocortisone (difference of 11.4%)—similar to Annane et al results. In hydrocortisone group there was an increased incidence of superinfections, including new episodes of septic shock. Sprung, NEJM,2008; Vol 358 No 2.")
119
Glucose Control: SSC Recommendations
Initial stabilization of patients with severe sepsis and hyperglycemia who are admitted to the ICU receive IV insulin therapy to reduce blood glucose levels. (1B) Use of a validated protocol and target glucose levels to < 150 mg/dL range. (2C) All patients receiving IV insulin should receive a glucose calorie source and blood glucose values should be initially assesses every 1-2 hrs, then q 4 hours after stabilization. (1C) Low glucose levels obtained by Point of Care testing should be interpreted with caution (1B) Dellinger RP, et al. Crit Care Med. 2008;36:
 Use of a validated protocol and target glucose levels to < 150 mg/dL range. (2C) All patients receiving IV insulin should receive a glucose calorie source and blood glucose values should be initially assesses every 1-2 hrs, then q 4 hours after stabilization. (1C) Low glucose levels obtained by Point of Care testing should be interpreted with caution (1B) Dellinger RP, et al. Crit Care Med. 2008;36:")
120
NICE Study 6104 Critically Ill Patients within 24 hrs of admission to ICU randomized Data evaluated on 3010 pts in intensive control group (target mg/dL) & 3012 pts to conventional group (target < 180 mg/dL) Similar characteristics at baseline Results: Conventional group has significantly lower number of deaths Severe hypoglycemia (blood glucose < 40mg per dL greater in intensive control group (6.8% vs. .5% (p<0.001 Both groups used IV insulin, patient expected to be in the ICU > 3 days, randomization was done unblinded using operative non-operative process. If in conventional group BG < 144, infusion stopped, insulin administration done by algorithm. Discontinued if eating or d/c from ICU and resumed if readmitted to the ICU. Use arterial blood glucose samples/ measure POC, ABG or lab. If hypo/confirmed with lab draw before decision, feed equally and the amount of cal by enteral 2/3 parenetal 1/3..no diff 27.5% vs. 24.9% (p =0.02) NICE-SUGAR Investigators, N Engl J Med;2009:
 & 3012 pts to conventional group (target < 180 mg/dL) Similar characteristics at baseline. Results: Conventional group has significantly lower number of deaths. Severe hypoglycemia (blood glucose < 40mg per dL greater in intensive control group (6.8% vs. .5% (p< Both groups used IV insulin, patient expected to be in the ICU > 3 days, randomization was done unblinded using operative non-operative process. If in conventional group BG < 144, infusion stopped, insulin administration done by algorithm. Discontinued if eating or d/c from ICU and resumed if readmitted to the ICU. Use arterial blood glucose samples/ measure POC, ABG or lab. If hypo/confirmed with lab draw before decision, feed equally and the amount of cal by enteral 2/3 parenetal 1/3..no diff. 27.5% vs. 24.9% (p =0.02) NICE-SUGAR Investigators, N Engl J Med;2009:")
121
Procedure or Population Breakdown
NICE-SUGAR Investigators, N Engl J Med;2009:

122
Do NOT Return to Sliding Scale
What to Do Now? Continue to Optimize Management of Glucose to Prevent Hyperglycemic & Hypoglycemic Events…range target to < 180 mg/dL, stop infusion at 140 mg/dL Do NOT Return to Sliding Scale Inzucchi SE, Siegel MD. N Engl J Med;2009;360(13):
:")
123
Additional Management Bundle Components Barriers
TGC: Lack of tested nomogram What target range to pick? Evaluating success Increase nursing time Not enough monitors Low TV ventilation Lack of knowledge of research by physicians, RT and nursing No defined policy Lack of accountability Identifying patients who have ALI or ARDS?

124
Sepsis Evidence Implementation
Making it a Reality Sepsis Bundle

125
Screen for Severe Sepsis Management Sepsis Bundle (24 hour)
Sepsis Bundles Screen for Severe Sepsis Yes No Standard care Resuscitation Sepsis Bundle (6-Hour) Obtain Cultures before antibiotic administration Lactate Level In the event of hypotension (SBP < 90, MAP < 70) or lactate > 4 mmol/L, begin initial fluid resuscitation with ml of crystalloid (or colloid equivalent) per estimated kg of body weight Vasopressors employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid resuscitation Board spectrum antibiotics administered Within 3 hours of presentation In the event of septic shock or lactate > 4 mmol/L, CVP and ScvO2 or SVO2 measured. In the event of septic shock or lactate > 4 mmol/L, CVP maintained 8-12 mmhg Inotropes (and/or PRBC’s if hematocrit <= 30 percent) delivered for ScvO2 < 70 percent or SVO2 < 65 percent if CVP >= 8 mmhg If on Antibiotic, then Monitor Q24H FL Monitor Per shift ICU Management Sepsis Bundle (24 hour) Maintain serum glucose levels on average < 150 mg/dl. (8.3 mmol/L ) Drotrecogin alfa (activated) administered in accordance with hospital guidelines Steroids given for septic shock requiring continued use of vasopressors for equal to or greater than 6 hours Adoption of a lung protective strategy (tidal volumes < 6ml/kg) with plateau pressures of 30 cm H2O for mechanically ventilated patients
 Obtain Cultures before antibiotic administration. Lactate Level. In the event of hypotension (SBP < 90, MAP < 70) or lactate > 4 mmol/L, begin initial fluid resuscitation with ml of crystalloid (or colloid equivalent) per estimated kg of body weight. Vasopressors employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid resuscitation. Board spectrum antibiotics administered Within 3 hours of presentation. In the event of septic shock or lactate > 4 mmol/L, CVP and ScvO2 or SVO2 measured. In the event of septic shock or lactate > 4 mmol/L, CVP maintained 8-12 mmhg. Inotropes (and/or PRBC’s if hematocrit <= 30 percent) delivered for ScvO2 < 70 percent or SVO2 < 65 percent if CVP >= 8 mmhg. If on Antibiotic, then Monitor Q24H FL Monitor Per shift ICU. Management Sepsis Bundle (24 hour) Maintain serum glucose levels on average < 150 mg/dl. (8.3 mmol/L ) Drotrecogin alfa (activated) administered in accordance with hospital guidelines. Steroids given for septic shock requiring continued use of vasopressors for equal to or greater than 6 hours. Adoption of a lung protective strategy (tidal volumes < 6ml/kg) with plateau pressures of 30 cm H2O for mechanically ventilated patients.")
126
Develop Protocols & Order Sets to Implement Resuscitation in Medical-Surgical Area
Draw blood Lactate Level Obtain blood cultures before administration of antibiotic In the event of hypotension (SBP < 90, MAP < 70) or lactate > 4 mmol/L, begin initial fluid resuscitation with ml of crystalloid (or colloid equivalent) per estimated kg of body weight Vasopressors employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid resuscitation Broad spectrum antibiotics administered within three hours of presentation
 or lactate > 4 mmol/L, begin initial fluid resuscitation with ml of crystalloid (or colloid equivalent) per estimated kg of body weight. Vasopressors employed for hypotension ((MAP) Less than 65 mm Hg) during and after initial fluid resuscitation. Broad spectrum antibiotics administered within three hours of presentation.")
127
Within 6 hrs (Transport to the ICU is Key)
In the event of septic shock or lactate > 4 mmol/L, CVP and ScvO2 or SVO2 measured. (line inserted) In the event of septic shock or lactate > 4 mmol/L, CVP maintained 8-12 mmhg Inotropes (and/or PRBC’s if hematocrit <= 30 percent) delivered for ScvO2 < 70 percent or SVO2 < 65 percent if CVP >= 8 mmhg
 In the event of septic shock or lactate > 4 mmol/L, CVP maintained 8-12 mmhg. Inotropes (and/or PRBC’s if hematocrit <= 30 percent) delivered for ScvO2 < 70 percent or SVO2 < 65 percent if CVP >= 8 mmhg.")
128
Develop Protocols & Order Sets to Implement Management 24-Hour Severe Sepsis Bundles
Adoption of a lung protective strategy (tidal volumes < 6ml/kg) with plateau pressures of 30 cm H2O for mechanically ventilated patients with ALI/ARDS Drotrecogin alfa (activated) administered in accordance with hospital guidelines Maintain serum glucose levels on average < 150 mg/dl. (8.3 mmol/L) Consider steroids given for septic shock requiring continued use of vasopressors and fluid resuscitation and remains unstable This index list also provides a means to quickly link to the specific slides related to the topic. Click on the subject when the slide is in the “show” mode and the slides automatically advances to the first slide of that specific guideline.
 with plateau pressures of 30 cm H2O for mechanically ventilated patients with ALI/ARDS. Drotrecogin alfa (activated) administered in accordance with hospital guidelines. Maintain serum glucose levels on average < 150 mg/dl. (8.3 mmol/L) Consider steroids given for septic shock requiring continued use of vasopressors and fluid resuscitation and remains unstable. This index list also provides a means to quickly link to the specific slides related to the topic. Click on the subject when the slide is in the show mode and the slides automatically advances to the first slide of that specific guideline.")
129
Fourth Tier: Measuring Process and Outcomes Changes
Success Implementation of the Sepsis Bundle Early Screening with Tools and Triggers Organizational Consensus that Severe Sepsis Must be Managed Early and Aggressively

130
Sepsis Measurement tool found at www.ihi.org & www.survivingsepsis.org

131
Data Collection Outcome Process Mortality (ICU and Hosp) Hosp LOS
Cost per case (total and direct) Process SSC database Data elements that measure implementation of resuscitation and management bundle
 Process. SSC database. Data elements that measure implementation of resuscitation and management bundle.")
132
Role of Data Outcome data Process data
Share with staff and administration to keep momentum going Helps convince/move skeptics Process data Celebrate small successes Helps identify where opportunities for improvement still exist

133
Implementation Hospital resources often focused on planning phase and then back off after implementation. The implementation phase is the most critical Frequent rounds recommended on unit by project champion to support staff and answer questions. Defined resources for bedside nurse-IE: Project champion has pager to be available 24/7 initially Clinical nurse champions identified on each ICU unit and ED to be resources to bedside staff (these staff should be a member of the sepsis team/committee from the beginning)
")
134
Severe Sepsis Bundle Implementation Results
Loma Linda, California England Germany St. Louis, Missouri

135
Surviving Sepsis Campaign
252 hospitals in 18 countries Data from January 2005-March 2008 Observational; time series Baseline is first quarter data was collected Use of standardized screening tool Excluded site if less than 20 patients or less than 3 months of results M Levy, presented at SCCM 02/2009 Nashville

136
Surviving Sepsis Campaign Results
Final Sample Size: 15,022 patients from 166 sites (95% of total) North America: 58% Europe: 31% South America: 10% M Levy, presented at SCCM 02/2009 Nashville
 North America: 58% Europe: 31% South America: 10% M Levy, presented at SCCM 02/2009 Nashville.")
137
Surviving Sepsis Campaign Results
Entry Point Subjects Mortality (hosp) ED 52% 27.6 ICU 12.8% 41.3 Ward 34.8% 46.8 Hospital mortality went from 37% to 30% 7% ARR; 19% RRR; p< 0.007 M Levy, presented at SCCM 02/2009 Nashville
 ED. 52% ICU. 12.8% Ward. 34.8% Hospital mortality went from 37% to 30% 7% ARR; 19% RRR; p< M Levy, presented at SCCM 02/2009 Nashville.")
138
Surviving Sepsis Campaign Bundle Compliance
Baseline 2 year Resuscitation 10.9 % 31.3 % Management 18 % 36 % Risk Adjusted Hospital Mortality decreased by 5.4% 20 % improvement in compliance with bundles M Levy, presented at SCCM 02/2009 Nashville

139
The Multi-Center Severe Sepsis & Septic Shock Collaborative Group
A Prospective Multi-Center Collaborative Study Before and After Implementation of an Early Sepsis Initiative The Multi-Center Severe Sepsis & Septic Shock Collaborative Group Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/09

140
Methods Pre-implementation analysis occurred from with post-implementation observation from 11 centers ranging from community (N=6) to academic tertiary care (N=5) settings were included in the study. In this intention-to-treat evaluation, all patients including DNR were examined. Needs work; Need to divide into 2 slides Consider adding How patients were identified Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/09 140
 to academic tertiary care (N=5) settings were included in the study. In this intention-to-treat evaluation, all patients including DNR were examined. Needs work; Need to divide into 2 slides. Consider adding How patients were identified. Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/")
141
Should we include here or not? At the End

143
Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/09

144
In-Hospital Mortality: M SS/SS C vs. SSC
PRE % POST % ARR % RRR % M SS/SS C 39.1 28.9 10.2 26.0 1st Q Last Q SSC 37.0 30.0 7.0 19.0 Use slide if some asks question comparing to SSC Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/09

145
Mortality by Lactate & SBP Subsets
PRE- POST- Lactate > 4 Only 40.4 32.9 SBP < 90 Only 42.4 30.9 Lactate > 4 & SBP < 90 57.3 39.5 Presented by Emanuel Rivers at the World Federation of Critical care Medicine, Florence Italy 08/09

146
Bundle Implementation: Decreased Mortality
Methodology 2 year prospective study in academic tertiary care facility, with majority of care delivered in the ED 330 patient enrolled Measured 5 quality indicators related to management of Severe sepsis & septic shock population. CVP/ScvO2 by 2 hrs, antibiotics by 4 hours, EGDT completed at 6 hours, appropriate steroids, lactate clearance Nguyen et al CCM, Vol 35, No. 4,

147
Bundle Implementation: Decreased Mortality
Results: In hospital mortality in patients who completed the bundle was significantly lower then those who did not complete the bundle (20.8 vs 39.5; p<0.01) 14% of patients that completed the bundle received rhAPC. Completing EGDT in 6 hours was the only quality indicator with a significant odds ratio for decreased mortality using multivariate regression analysis After 2 years, achieved 51% compliance with all five indicators Nguyen et al CCM, Vol 35, No. 4,
 14% of patients that completed the bundle received rhAPC. Completing EGDT in 6 hours was the only quality indicator with a significant odds ratio for decreased mortality using multivariate regression analysis. After 2 years, achieved 51% compliance with all five indicators. Nguyen et al CCM, 2007 Vol 35, No. 4,")
148
Bundle Component Compliance and Impact on Mortality
Nguyen et al CCM, Vol 35, No. 4

149
Prospective External Validation of Effectiveness of EGDT
Prospective interventional study conducted over 2 years Compared 79 patients in pre-intervention year and 77 patients in post intervention year Intervention group received significantly more fluid (2L), less vasopressors Mortality 18% vs. 27% Jones AE, et al. Chest, 2007;132:
, less vasopressors. Mortality 18% vs. 27% Jones AE, et al. Chest, 2007;132:")
150
Sepsis Bundles: Significant Impact on Hospital Outcomes
Two acute National Health Service Trust Teaching Hospitals in England performed a prospective observational study with 101 adult patients with severe sepsis or septic shock Outcomes measures Rate of compliance with 6-hour and 24-hour bundles adapted from 2004 SSC guidelines Hospitality mortality between compliant and noncompliant groups Compliance with Bundles 6-hour bundle 52% 24-hour bundle 30% Bundle Mortality Noncompliant 49% (p=.001) Compliant 23% (p=.001) More than two-fold increase in hospital mortality associated with noncompliant group Assessed compliance as “all or none” for the bundle elements Is a two-fold mortality improvement a possibility in your institution? Source: Gao F, Melody T, Daniels D, et al. The impact of compliance with 6-hour and 24-hour sepsis bundle on hospital mortality in patients with severe sepsis: A prospective observational study. Crit Care Med. 2005;9(6):R764-R770.
 Compliant 23% (p=.001) More than two-fold increase in hospital mortality associated with noncompliant group. Assessed compliance as all or none for the bundle elements. Is a two-fold mortality improvement a possibility in your institution Source: Gao F, Melody T, Daniels D, et al. The impact of compliance with 6-hour and 24-hour sepsis bundle on hospital mortality in patients with severe sepsis: A prospective observational study. Crit Care Med. 2005;9(6):R764-R770.")
151
Compliance with 6hr Bundle Gao F, et al. Critical Care, 2005;9:R764-770
84% 74% 74% 70% 52% What is the compliance of the 6-h sepsis bundle in our patients? There was not a hundred percent compliance, and only 52% of patients were fully bundled with the lowest compliance in the task of lactate measurement. We then compared the fully bundled group with non-fully bundled group.

152
6hr Bundle & Hosp Mortality Gao F, et al
6hr Bundle & Hosp Mortality Gao F, et al. Critical Care, 2005;9:R RR=2.12 ( ) 49% P=0.01 Mortality NNT = 3.9 N=24/49 23% However, the hospital mortality was very different. There was a more than 2-fold increase in hospital mortality in the non-fully bundled group compared with the fully bundled group with 49% vs 23% with risk ratio 2.12 (95%CI 1.2 to 3.8) and P value The number needed to treat to save one life would be 4. N=12/52
 49% P=0.01. Mortality. NNT = 3.9. N=24/49. 23% However, the hospital mortality was very different. There was a more than 2-fold increase in hospital mortality in the non-fully bundled group compared with the fully bundled group with 49% vs 23% with risk ratio 2.12 (95%CI 1.2 to 3.8) and P value The number needed to treat to save one life would be 4. N=12/52.")
153
Compliance with 24hr Bundle Gao F, et al
Compliance with 24hr Bundle Gao F, et al. Critical Care, 2005;9:R 85% 64% 43% Now How about the compliance of 24-h bundle? There was a far from a hundred percent compliance. In fact, there was only 30% of patients fully bundled with the lowest compliance in the task of considering use of APC and use of steroids. 30%

154
24hr Bundle & Hosp Mortality Gao F, et al
24hr Bundle & Hosp Mortality Gao F, et al. Critical Care, 2005;9:R RR=1.75( ) 50% P=0.16 Mortality 29% NNT = 4.8 N=24/48 N=6/21 However, the hospital mortality was 50% in the non-fully bundled group compared with with 29% in the fully bundled group. There was a 75% increase in risk for hospital deaths in this group although this did not reach a statistical significance due to small sample size.
 50% P=0.16. Mortality. 29% NNT = 4.8. N=24/48. N=6/21. However, the hospital mortality was 50% in the non-fully bundled group compared with with 29% in the fully bundled group. There was a 75% increase in risk for hospital deaths in this group although this did not reach a statistical significance due to small sample size.")
155
Severe Sepsis Protocol in Use Germany
Retrospective cohort study in 10 bed mixed ICU in Germany 60 patients (30 consecutive receiving SOP severe sepsis management compared to historical controls) Measured: Primary endpoint 28 day mortality Measured: Secondary endpoints; ABG’s, lactate, glucose, creat, WBC, Plat, time to dx & 7am on day 2 & 4 SOFA scores Results: In SOP group: ↑ use of dobutamine, glucose control, steroids & rhAPC Mortality: Control vs SOP (53% vs. 27% p <.05) Independent predictors of survival: lactate on admission, age, gender, blood glucose < 150 mg/dl, adm of rhAPC & steroids Kortgen A et al. Crit Care Med, 2006:34:
 Measured: Primary endpoint 28 day mortality. Measured: Secondary endpoints; ABG’s, lactate, glucose, creat, WBC, Plat, time to dx & 7am on day 2 & 4 SOFA scores. Results: In SOP group: ↑ use of dobutamine, glucose control, steroids & rhAPC. Mortality: Control vs SOP (53% vs. 27% p <.05) Independent predictors of survival: lactate on admission, age, gender, blood glucose < 150 mg/dl, adm of rhAPC & steroids. Kortgen A et al. Crit Care Med, 2006:34:")
156
Standardized Order Set-Sepsis Bundles St. Louis, Missouri
Before-after study design with prospective consecutive data collection of 120 patients 1,200 bed academic medical center Primary endpoint: 28 day mortality Other measures: hospital LOS, IV fluid intact for shock, appropriate antibiotic Results: after group: received more IV fluids in ED (p=0.002); more likely to receive >20ml/kg of fluid prior to vasopressors; had lower risk of mortality (48.3% vs 30%, p=0.04); lower hospital LOS (12.1 vs 8.9 days, p=0.038) Independent predictors of survival: increased pt age and not receiving >20 ml/kg of IV fluid prior to vasopressors Micek, Scott et al., Critical Care Medicine, 2006; 34:
; more likely to receive >20ml/kg of fluid prior to vasopressors; had lower risk of mortality (48.3% vs 30%, p=0.04); lower hospital LOS (12.1 vs 8.9 days, p=0.038) Independent predictors of survival: increased pt age and not receiving >20 ml/kg of IV fluid prior to vasopressors. Micek, Scott et al., Critical Care Medicine, 2006; 34:")
157
Standardized Order Set-Sepsis Bundles Decreases Cost St
Standardized Order Set-Sepsis Bundles Decreases Cost St. Louis, Missouri Before-after study design with prospective consecutive data collection of 120 patients to determine financial impact of sepsis protocol 1,200 bed academic medical center Primary endpoint: Overall Hospital costs Secondary endpoint: Hospital LOS Results: after group: Hospital costs $16,103 vs. $21,985, p = .008; LOS 5 days less in the protocol group (p= .023) Use of protocol independently associated with less per patient cost. Shorr AF, et al. Critical Care Medicine, 2007; 35:
 Use of protocol independently associated with less per patient cost. Shorr AF, et al. Critical Care Medicine, 2007; 35:")
158
Case Study Disclaimer: This is intended for education purposes
Judgment of physician/clinician should always be the deciding factor The following case represents individual experience that are specific to these patients and may not reflect the typical course of recovery

159
Case Study 3: Early Identification and Intervention
63 year old white female directly admitted to a med-surg floor from a free standing urgent care at 2130 Hx: NIDDM, COPD, HTN Chief complaint: pain right lower sternal border times 2 days, worse with deep breath, SOB. CXR: right pleural effusion Orthostatic hypotension, renal insufficiency (creatinine 3.4—previously 1.2)
")
160
Case Study 3: Early Identification And Intervention
Initial VS: stable BP, HR-102, RR-WNL On 2L nasal cannula, IV at 150/hr Labs: WBC-7.5, plat 197, D-dimer: 273 Resp distress at 0600 next am Transferred to MICU Possible PE—heparin gtt started Broad spectrum antibiotics started

161
Case Study 3: Early Identification And Intervention
ICU course: 2000: BP: 79/34, HR: 123 , WBC: 3.3 Dx of severe sepsis at 2000 2 liter fluid bolus Intubated and ventilated Lactic acid 0.9 Levophed started, heparin gtt d/c’d CVP inserted

162
Case Study 3: Early Identification And Intervention
ICU course-continued: Xigris started at 0600 (still on vasopressors, vent, creat-3.9) 1000: Stopped Xigris for CT guided pleural aspirtation 1200: CT- 2 loculated cavities in right lung; Cardio thoracic surgery consulted OR at 1700 for drainage of empyema Right mini-thorocotomy, empyema drainage, decortication and bronchoscopy. CT (2) inserted
 1000: Stopped Xigris for CT guided pleural aspirtation. 1200: CT- 2 loculated cavities in right lung; Cardio thoracic surgery consulted. OR at 1700 for drainage of empyema. Right mini-thorocotomy, empyema drainage, decortication and bronchoscopy. CT (2) inserted.")
163
Case Study 3: Early Identification And Intervention
Post-op Temp-97, HR: 84, BP-139/69 on levophed and vasopressin and bicarb gtt. Xigris restarted Post-op Day 1 Levophed off at 0400 Bicarb gtt off at 0400 Vasopressin gtt off at 1000 Vent FiO2 decreased to 0800 Full course of Xigris Off vent/extubated in 6 days (hx of COPD) Transfer out of ICU- post-op day 11 Discharge home- post-op day 25
 Transfer out of ICU- post-op day 11. Discharge home- post-op day 25.")
164
The Nurses Role Early recognition of patients with signs of sepsis
Early initiation of evidence based practice therapies appropriate for your area of practice (antibiotics, fluids/blood & pressors) Swift disposition to care areas where the rest of the bundle can be started.
 Swift disposition to care areas where the rest of the bundle can be started.")
Similar presentations

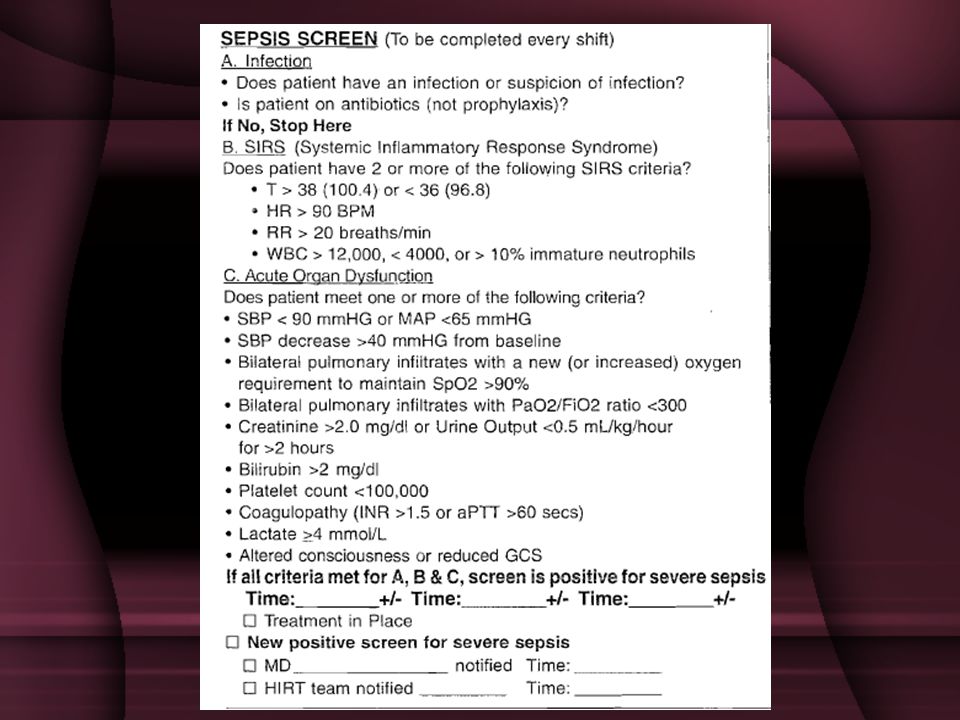


 for severe sepsis and septic shock treatment>")












, Society of Critical Care Medicine (SCCM), and the International Sepsis Forum (ISF) developed.>")



 GORDONR. BERNARD, M.D. et al. The New England Journal of Medicine.>")

