Download presentation
Presentation is loading. Please wait.

1
Congestive Heart Failure and Cardiomyopathy
Mark Bromley PGY-1

2
Case 1 A 63-year-old male presents with breathlessness x 3 days.
?Approach, ?Hx PMHx: MI 3 years ago 4-vessel CABG asymptomatic since surgery with no complaints of CP HPI: Over the last 3 months, the patient notes onset of shortness of breath while unloading groceries, and walking stairs. 2 weeks ago, he was unable to complete his daily one-mile walk at the high school track. He noted swelling in his feet and ankles. 4 days ago he woke at 2 am short of breath and had to sleep in his recliner the rest of the night. He has been unable to lay flat in bed at night since then and has slept on 3 pillows. Yesterday, he became breathless walking from one room to another He presents today with extreme shortness of breath He denies chest pain

3
BP 108/52 P 140, irreg. R 30 and labored Temp 99°F Ht: 5'8" Wt: 210.
General: Breathless, moderately obese male in acute distress sitting upright complaining "I am going to die. Please help me." Chest: Scattered rhonchi throughout, rales bilateral one third lower bases. Cough is productive and frothy. CVS: Tachycardia and irreg. Grade 3/6 systolic murmur at LSB, S3 gallop noted. JVP to jaw Abd: Liver palpable three centimeters below right costal margin. HJR. Extremities: 4+ pitting edema of lower extremities to the knees. Pulses intact.

4
Organization of CHF Importance Pathophysiology Diagnosis Etiologies – Decompensation Management Cardiomyopathy

5
Importance Increasing burden
Aging population Improved survival (Hypertension/CAD) Nationwide, heart failure affects more than Canadians1 (10% of those >75) > new cases are diagnosed /yr1
 Nationwide, heart failure affects more than Canadians1. (10% of those >75) > new cases are diagnosed /yr1.")
6
Bad Disease Mortality ED visits 1 year – 10-20% 6 year – 60-80%
20% new diagnosis 80% repeat visit (decompensation)
")
7
Definition CHF Pulmonary Edema
Inability of the heart to maintain adequate vital organ perfusion at normal filling pressures Decreased exercise capacity Associated neurohumoral-endocrine changes, initially compensatory but ultimately maladaptive Pulmonary Edema A condition associated with increased loss of fluid from the pulmonary capillaries into the pulmonary interstitium and alveoli

8
The heart is a pump that works together with the lungs
The heart is a pump that works together with the lungs. It pumps blood in 2 ways It pumps blood from the heart to the lungs to pick up oxygen. The oxygenated blood returns to the heart It then pumps blood out into the circulatory system of blood vessels that carry blood through the body

9
In HF the pumping action of the heart becomes less and less efficient/powerful
The heart does not pump blood as well as it should When this happens, blood does not move efficiently through the circulatory system It starts to back up, increasing the pressure in the blood vessels, forcing fluid from the blood vessels into body tissues.

11
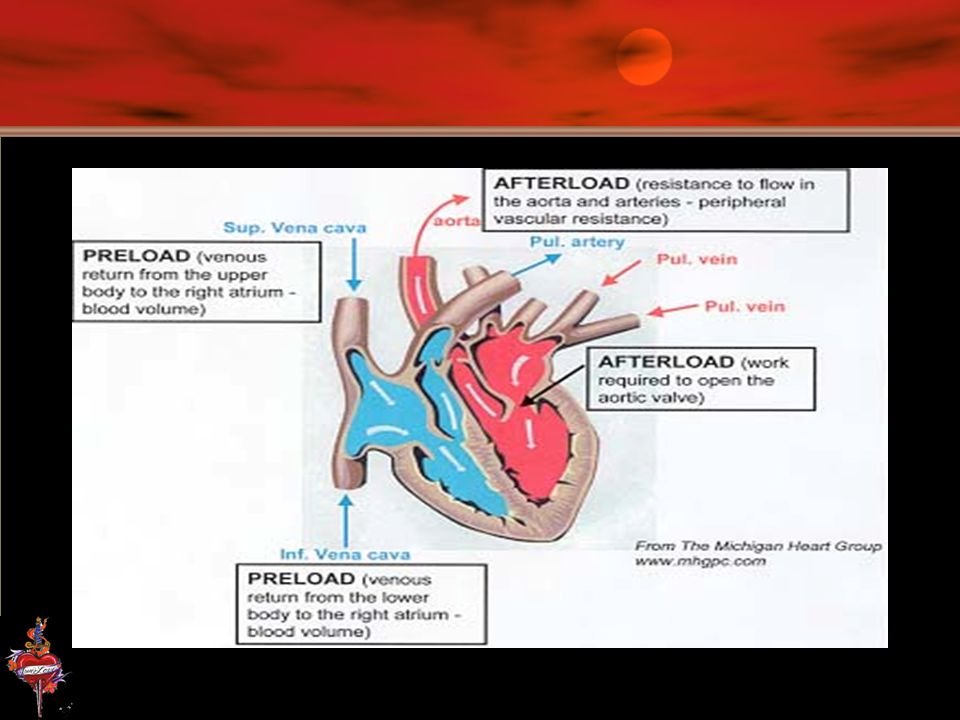
Physiology ↓ CO = HR X Stroke Volume
SV = preload + contractility - afterload

13
Preload initial stretching of the cardiac myocytes prior to contraction

14
Afterload the "load" that the heart must eject blood against
Aortic pressure Hypertrophy is a mechanism that allows more muscle fibers to share the work Stroke Volume

15
Contractility ability of a cardiac muscle fiber to contract at a given fiber length catecholamines (norepi and epi) sympathetic stimulation Ca++

16
Neurohormonal Activation
Jackson, G et al. BMJ 2000;320: Copyright ©2000 BMJ Publishing Group Ltd.

17
[Nor-epi] and Mortality
Jackson, G et al. BMJ 2000;320: Copyright ©2000 BMJ Publishing Group Ltd.
![[Nor-epi] and Mortality](http://slideplayer.com/slide/3908827/13/images/17/%5BNor-epi%5D+and+Mortality.jpg "Jackson, G et al. BMJ 2000;320: Copyright ©2000 BMJ Publishing Group Ltd.")
18
Sympathetic Activation
Jackson, G et al. BMJ 2000;320: Copyright ©2000 BMJ Publishing Group Ltd.

19
Remodelling Post MI Jackson, G et al. BMJ 2000;320:167-170
Copyright ©2000 BMJ Publishing Group Ltd.

20
Classification of Heart Failure
Low Output Cardiac output is low, but demand for blood flow is normal The heart is unable to meet this demand and fails Dx: IHD, HTN, dilated cardiomyopathy, valvular and pericardial dz High Output High-output heart failure Cardiac output is normal or a little bit high Demand for blood flow is abnormally high (hyperthyroidism, anemia, severe infections) The heart is unable to deliver the increased amount of blood and fails Dx: hyperthyroidism, anemia, pregnancy, AV fistulas, beriberi, & Paget’s Rx: ↓volume overload and correct the underlying disorder
 The heart is unable to deliver the increased amount of blood and fails. Dx: hyperthyroidism, anemia, pregnancy, AV fistulas, beriberi, & Paget’s. Rx: ↓volume overload and correct the underlying disorder.")
21
Classification of Heart Failure
Acute MI, Acute Valve Dysfunction largely systolic sudden reduction in cardiac output often results in systemic hypotension without peripheral edema Chronic Cardiomyopathy arterial pressure tends to be well maintained until very late in the course there is often accumulation of peripheral edema Chordae Tendonae Rupture. Large enough area of ischemia.

22
Classification of Heart Failure
Right Sided (right ventricle) (pulmonic stenosis or pulmonary hypertension) When the right side of the heart starts to fail, fluid collects in the feet and lower legs As the heart failure becomes worse, the legs swell and eventually the abdomen collects fluid (ascites, hepatic congestion) Weight gain accompanies the fluid retention and is an excellent measure of how much fluid is being retained. Left Sided (left ventricle) left ventricle is mechanically overloaded (aortic stenosis) or weakened (post MI) When the left side of the heart starts to fail, fluid collects in the lungs (Orthopnea/PND) Breathing becomes more difficult, and the patient may feel short of breath, particularly with activity or lying down This extra fluid in the lungs makes it more difficult for the airways to expand on inhalation ↓O2 diffusion However, when heart failure has existed for months or years, biventricular failure usually results. For example, patients with long standing aortic valve disease or systemic hypertension may have ankle edema, congestive hepatomegaly, and systemic venous distention late in the course of their disease, even though the abnormal hemodynamic burden initially was placed on the left ventricle.
 (pulmonic stenosis or pulmonary hypertension) When the right side of the heart starts to fail, fluid collects in the feet and lower legs. As the heart failure becomes worse, the legs swell and eventually the abdomen collects fluid (ascites, hepatic congestion) Weight gain accompanies the fluid retention and is an excellent measure of how much fluid is being retained. Left Sided (left ventricle) left ventricle is mechanically overloaded (aortic stenosis) or weakened (post MI) When the left side of the heart starts to fail, fluid collects in the lungs (Orthopnea/PND) Breathing becomes more difficult, and the patient may feel short of breath, particularly with activity or lying down. This extra fluid in the lungs makes it more difficult for the airways to expand on inhalation. ↓O2 diffusion. However, when heart failure has existed for months or years, biventricular failure usually results. For example, patients with long standing aortic valve disease or systemic hypertension may have ankle edema, congestive hepatomegaly, and systemic venous distention late in the course of their disease, even though the abnormal hemodynamic burden initially was placed on the left ventricle.")
23
Classification of Heart Failure
Systolic The heart has difficulty contracting and pumping out enough blood weakness, fatigue and decreased ability to exercise ↓Ejection fraction = (stroke volume)/(end diastolic volume) A normal ejection fraction is greater than 50% Systolic heart failure has a ↓EF < 50%. Diastolic The heart is unable to fill properly during diastole ↑ filling pressure This impedes blood filling into the heart → backup into the lungs → CHF symptoms ↑ in patients > 75 years; women; HTN Ejection fraction is normal
/(end diastolic volume) A normal ejection fraction is greater than 50% Systolic heart failure has a ↓EF < 50%. Diastolic. The heart is unable to fill properly during diastole. ↑ filling pressure. This impedes blood filling into the heart → backup into the lungs → CHF symptoms. ↑ in patients > 75 years; women; HTN. Ejection fraction is normal.")
24
Classification of Heart Failure
Directional Heart Failure Backwards heart failure The ventricle is not pumping out all the blood that comes into it. ↑ ventricular filling pressure and systemic or pulmonary edema In fact, the heart can only meet the needs of the body if the ventricular filling pressure is high Forward heart failure The heart is not pumping out enough blood to meet the needs of the body ↓ blood reaches the kidneys, they conserve salt and water, which contributes to excess fluid retention and edema Forward failure also decreases the blood flow to various organs, causing weakness and fatigue

26
Diagnosis History Phsyical EKG CXR

27
History Prior Heart Dz, Dyspnea, PND, Orthopnea, Fatigue, Cough, Bloating, Angina, ↑Wt/↑Girth, Nocturia Precipitants ↑salt, non-compliance, new meds, NSAIDs, palpitations, angina Comorbidities (COPD, Renal Dz, DM)
")
28
PE ↑HR ↑RR JVP HJR Precordial exam: Lungs: Peripheral Edema
Apical impulse Location, Size, Sustained (45’ LLD position – exp) Loud P2 S3 (ventricular vibration with rapid filling) Low pitched (bell) 45’ LLD position Lungs: Cracks / Wheezes Peripheral Edema Beware of AP films and poor inspiration (FP)
 Loud P2. S3 (ventricular vibration with rapid filling) Low pitched (bell) 45’ LLD position. Lungs: Cracks / Wheezes. Peripheral Edema. Beware of AP films and poor inspiration (FP)")
29
Precision improves with further training (i. e
Precision improves with further training (i.e. Medical students<Residents<Staff<Cardiologists)
")
30
Precision improves with further training (i. e
Precision improves with further training (i.e. Medical students<Residents<Staff<Cardiologists)
")
31
Case 2 58 F with known Idiopathic Dilated Cardiomyopathy
Cardiac Cath (05): N coronaries LVEF 35% Meds: ACE-I, Diuretics, Digoxin ↑SOBOE x 3weeks OE: Displaced MPI Soft S3 Pre-sacral edema
: N coronaries LVEF 35% Meds: ACE-I, Diuretics, Digoxin. ↑SOBOE x 3weeks. OE: Displaced MPI. Soft S3. Pre-sacral edema.")
32
Case 3 70 M – Obese SOBOE and fatigue x 3 months No Orthopnea/PND
PMHx: Smoke x 40 pack-years, HTN (poorly controlled) DMII OE: BP 180/100 Sustained MPI Bilateral Rales Mild/Moderate Pretib Edema
 DMII. OE: BP 180/100. Sustained MPI. Bilateral Rales. Mild/Moderate Pretib Edema.")
33
X-ray Cardiomegally Redistribution (cephalization)
↑LV or hypertrophied ventricular wall Cardiothoracic Ratio > 50% Redistribution (cephalization) Systolic dys-fxn → ↑filling pressure Upper lobe vessels > Lower lobe vessels Blunting of costophrenic Angle Peribronchial cuffing Kerly-B lines
 Systolic dys-fxn → ↑filling pressure. Upper lobe vessels > Lower lobe vessels. Blunting of costophrenic Angle. Peribronchial cuffing. Kerly-B lines.")
34
Peri-Bronchial Cuffing

35
“First, strike for the jugular and let the rest go!”
Oliver W. Holmes Jr.

36
Etiology Dysrhythmia Tachy Brady
↓Diastolic filling time +/- atrial kick ↓CO ↓Coronary perfusion ↑ Myocardial O2 demand Brady ↓HR ↓CO = SV x ↓HR

37
Infection Anemia ↑ systemic met demands Pulm infection = ↓O2
Tachycardia Anemia Isovolumic hemodilution ↑CO meet O2 demands ↓Coronary O2 delivery

38
Acute valvular dysfunction
Pregnancy ↑ demand for CO Acute Myocarditis ↓ contactility Acute valvular dysfunction 2o to MI ↑preload or ↑↑afterload

39
PE Pharmacologic ↓O2 supply ↑ Pulmonary Hypertension
↓ inotropic effects ↑ Na / H2O retention

40
Etiology Decompensation/Causes of exacerbation
FAILURE: Forgot medication Arrhythmia/ Anemia Ischemia/ Infarction/ Infection (Pneumonia) Lifestyle: taken too much salt Up-regulation of CO: pregnancy, hyperthyroidism Renal failure Embolism: pulmonary Inappropriate treatment Failure to seek care 25% 10% 25% Other 10% 10% 20%
 Lifestyle: taken too much salt. Up-regulation of CO: pregnancy, hyperthyroidism Renal failure Embolism: pulmonary. Inappropriate treatment. Failure to seek care. 25% 10% 25% Other 10% 10% 20%")
41
Case 1 Management A 63-year-old male presents with breathlessness x 3 days. ?Approach, ?Hx PMHx: MI 3 years ago 4-vessel CABG asymptomatic since surgery with no complaints of CP HPI: Over the last 3 months, the patient notes onset of shortness of breath while unloading groceries, and walking stairs. 2 weeks ago, he was unable to complete his daily one-mile walk at the high school track. He noted swelling in his feet and ankles. 4 days ago he woke at 2 am short of breath and had to sleep in his recliner the rest of the night. He has been unable to lay flat in bed at night since then and has slept on 3 pillows. Yesterday, he became breathless walking from one room to another He presents today with extreme shortness of breath He denies chest pain

42
Management Treat the maladaptation ? LMNOP ↑ Vascular resistance
↑ Sympathetic tone ↑ Total blood volume ? LMNOP

43
Management Nitrates O2 Ventilation Assist Devices ACE I Diuretics
Morphine Inotropes

44
Airway/Breathing Non-rebreather facemask delivering 100% O2
Once initial therapy has begun, oxygen supplementation can be titrated in order to keep the patient comfortable and arterial oxygen saturation above 90 percent. O2 increases PCWP

45
NIPPV If respiratory distress and/or hypoxia persist, consider non-invasive PPV ↓ preload, ↓ afterload, and ↑ left ventricular performance Meta-analysis of 15 clinical trials: ↓mortality and ↓intubation with NPPV compared to conventional therapy Patients who fail/do not tolerate/have contraindications to NPPV should be intubated Positive end-expiratory pressure is often useful for improving oxygenation

46
Cardiogenic Pulmonary Edema Emergency Department
Multi-centre RCT 130 pts Cardiogenic Pulmonary Edema Emergency Department Medical therapy+O2 (65 pts) non-invasive pressure support ventilation (65 pts) Primary outcome – need for intubation Italian study – 5 departments
 non-invasive pressure support ventilation (65 pts) Primary outcome – need for intubation. Italian study – 5 departments.")
47
Loop Diuretics ↑Na & H2O excretion Useful in volume overload
Rapid onset Mild vasodilator ↑1/2 life in CHF …be careful Depletion of K + and Mg++

48
Loop Diuretics Dosing – not well established
High dose Lasix and low dose Nitro has worse outcomes than low dose Lasix and high dose Nitro

49
Morphine Controversial Weak vasodilator / ↓ Resp Drive
↑ ICU admisssions (OR = 3) Sacchetti ?Anxiolytic
 Sacchetti. Anxiolytic.")
50
Nitrates low dose high dose

51
Nitrates - Route SL/Spray (0.1 - 0.4mg / 5 min) x3
50-100ug/min IV Drip (5-10ug/min) titrate to effect ( ug) Transdermal Peripherally shut down Unreliable absorption Contraindications / Cautions Viagra RV MI Fixed Aortic Lesions
 titrate to effect. ( ug) Transdermal. Peripherally shut down. Unreliable absorption. Contraindications / Cautions. Viagra. RV MI. Fixed Aortic Lesions.")
52
Case 4 67 M ↑SOB Visibly Distressed 96 28 200/110 75% ORA
PMHx: HTN, DM II EKG:

53
Nitroprusside Direct smooth muscle relaxant
Balanced reduction of pre/after load Continuous pressure monitoring – good Avoid hypotension

54
Case 5 67 M ↑SOB Visibly Distressed 96 28 140/90 75% ORA
PMHx: HTN, DM II Meds: Inconsistent

55
Natriuretic Peptide Jackson, G et al. BMJ 2000;320:167-170
Copyright ©2000 BMJ Publishing Group Ltd.

56
Nesiritide Recombinant BNP ↓ Aldosterone ↓ Endothelin
↑ Na & H2O excretion – no reflex tachy Good for Nitro contraindications

57
VMAC Randomized, Double Blind 489 inpatients
IV Nisiritide vs IV Nitrates vs Placebo PCWP and Dyspnea Improvement in PCWP – 2mm 6h No change in Dyspnea Problems: ↓Nitro dosing Prolonged Hypotension Not ED patients Industry sponsored

58
Vosodilator Therapy: Nesiritide
Efficacy Phase 432 patients In the efficacy phase, 127 patients underwent hemodynamic monitoring with a pulmonary artery catheter A six hour infusion of nesiritide (0.015 and 0.03 µg/kg per min) decreased pulmonary capillary wedge pressure (6 and 10 mmHg versus an ↑ of 2 mmHg for placebo) Improved the clinical status in a greater number of patients (60% and 67% versus 14%) Comparative phase 305 patients Randomly assigned to nesiritide or standard vasoactive agents for seven days without hemodynamic monitoring Compared to standard treatment with a single vasoactive agent (dobutamine, milrinone, nitroglycerin, or nitroprusside) nesiritide produced a similar significant improvement in clinical status and reduction in dyspnea and fatigue that persisted during the entire infusion period. Asymptomatic, dose-related hypotension was the most common side effect
 decreased pulmonary capillary wedge pressure. (6 and 10 mmHg versus an ↑ of 2 mmHg for placebo) Improved the clinical status in a greater number of patients (60% and 67% versus 14%) Comparative phase. 305 patients. Randomly assigned to nesiritide or standard vasoactive agents for seven days without hemodynamic monitoring. Compared to standard treatment with a single vasoactive agent (dobutamine, milrinone, nitroglycerin, or nitroprusside) nesiritide produced a similar significant improvement in clinical status and reduction in dyspnea and fatigue that persisted during the entire infusion period. Asymptomatic, dose-related hypotension was the most common side effect.")
59
RR from meta-analysis: 1.74
Death within 30 days tended to occur more often among patients randomized to nesiritide therapy 35 [7.2%] of 485 vs 15 [4.0%] of 377 patients RR from meta-analysis: 1.74 (95% confidence interval [CI], ; P = .059) Hazard ratio after adjusting for study, 1.80 (95% CI, ; P = .057)
 Hazard ratio after adjusting for study, (95% CI, ; P = .057)")
60
Vasodilator Therapy Nitroglycerin: ↓preload ↓afterload
Nitroprusside: ↓ ↓ afterload Nesiritide - BNP

61
ACE Inhibitors Clear longterm benefits
Vasodilate Block Aldosterone Bradykinin System ↓ Remodeling Take longer to work than nitrates (peak effect 45min)
")
62
Effect of ACE-I Jackson, G et al. BMJ 2000;320:167-170
Copyright ©2000 BMJ Publishing Group Ltd.

63
placebo-controlled, randomized, double-blind study
Placebo-Controlled, Randomized, Double-Blind Study of Intravenous Enalaprilat Efficacy and Safety in Acute Cardiogenic Pulmonary Edema The purpose of this study was to evaluate the efficacy and safety of a single IV 2-hour infusion of enalaprilat (1 mg) placebo-controlled, randomized, double-blind study 20 CHF patients (NYHA class III or IV) Compared with placebo, enalaprilat ↓ pulmonary capillary wedge pressure (-37% versus -10%, P=.001), ↓ diastolic and mean systemic blood pressures (-21% vs 0%, P=.009, and -18% vs -1%, P=.026) ↓ diastolic and mean pulmonary blood pressures (-21% vs -8%, P=.040; -18% vs -9%, P=.046) ↓ brachial and renal resistances (-44% versus -14%, P=.017, and -22% versus -2%, P=.014) ↑ brachial and renal blood flows (+77% versus +8%, P=.036, and +12% versus 0%, P=.043) ↑ arterial oxygen tension (+2% versus -16%, P=.041) ↑ arterial oxygen saturation (+1% versus -2%, P=.045) Enalaprilat did not affect CO or carotid or hepatosplanchnic hemodynamics Excluded those already on ACE I
 placebo-controlled, randomized, double-blind study. 20 CHF patients (NYHA class III or IV) Compared with placebo, enalaprilat. ↓ pulmonary capillary wedge pressure (-37% versus -10%, P=.001), ↓ diastolic and mean systemic blood pressures (-21% vs 0%, P=.009, and -18% vs -1%, P=.026) ↓ diastolic and mean pulmonary blood pressures (-21% vs -8%, P=.040; -18% vs -9%, P=.046) ↓ brachial and renal resistances (-44% versus -14%, P=.017, and -22% versus -2%, P=.014) ↑ brachial and renal blood flows (+77% versus +8%, P=.036, and +12% versus 0%, P=.043) ↑ arterial oxygen tension (+2% versus -16%, P=.041) ↑ arterial oxygen saturation (+1% versus -2%, P=.045) Enalaprilat did not affect CO or carotid or hepatosplanchnic hemodynamics. Excluded those already on ACE I.")
64
BNP Why do we need another diagnostic test? How uncertain are we?
Diagnostic uncertainty How uncertain are we? How uncertain should we be? ER docs are rarely wrong when they rate the probability of HF as very high or very low2 ER docs are uncertain of the diagnosis in the in-betweeners (30%)2 The degree of clinical certainty (or uncertainty) is determined by comparing the clinical impression with an independent validated criterion (gold) standard. Because there is no validated criterion standard for the diagnosis of HF, previous natriuretic peptide studies have compared the ED diagnosis with a retrospective diagnosis by 2 cardiologists who reviewed the medical records and were blinded to natriuretic peptide results and ED diagnoses. This unvalidated criterion standard has been assumed, although never proven, to be more accurate than the diagnostic impression of physicians in the ED.
2. The degree of clinical certainty (or uncertainty) is determined by comparing the clinical impression with an independent validated criterion (gold) standard. Because there is no validated criterion standard for the diagnosis of HF, previous natriuretic peptide studies have compared the ED diagnosis with a retrospective diagnosis by 2 cardiologists who reviewed the medical records and were blinded to natriuretic peptide results and ED diagnoses. This unvalidated criterion standard has been assumed, although never proven, to be more accurate than the diagnostic impression of physicians in the ED.")
65
BNP ↑Ventricular pressure & ↑Stretch
↑Ventricular pressure & ↑Stretch Pro-BNP → Nt-BNP(↑spec) & BNP(↑sens)
 & BNP(↑sens)")
66
Breathing Not Properly
Prospective, Blinded 1586 pts presenting with acute dyspnea ED Study Bedside assay “Gold Standard” = 2 cardiologists Breathing Not Properly

67
Breathing Not Properly
ad

68
Breathing Not Properly

69
Prospective diagnostic test evaluation 7 centers 1586 patients
BNP – blinded Gold Standard – Cardiology Chart Review 97% certainty by ED physician At “80%” EP certainty Sens: 49% Specificity: 96% At 100 pg/ml Sens: 90% Specificity: 73%

70
adf

71
Breathing Not Properly - Analysis
BNP brings us closer to the “gold standard” Low Prob -EP 17% had CHF 90% would have been corrected by BNP High Prob -EP 4% did not have CHF 80% would have been corrected by BNP Uncertain -EP BNP correctly classified 74% Misclassified 7%

72
BNP Levels < 100 pg/ml may prompt clinician to focus on alternative diagnosis (COPD) Reasonable neg pred value Prognostic Value ?Variation with Age/Gender/Kidney fxn

73
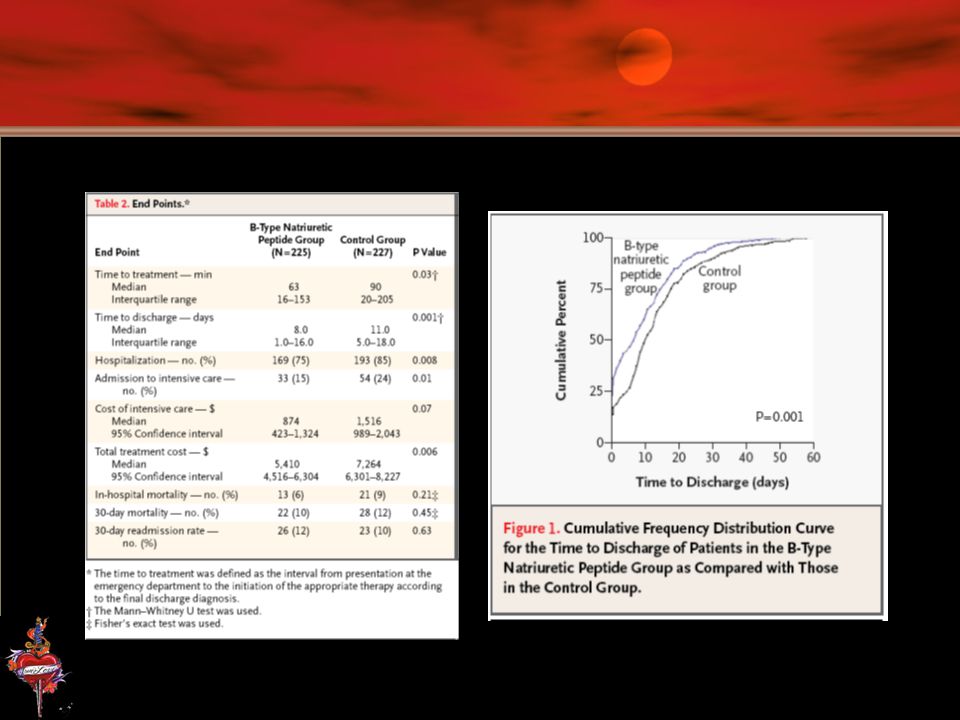
Prospective, Randomized, Controlled
Single blind 452 Pts with dyspnea Diagnostic Strategy (BNP) vrs Standard Assessment Told EP if <100 CHF unlikely, >500 CHF likely, indeterminate End Points: Time to D/C & Total Cost Safety: Similar Conclusion: BNP improved evaluation thereby improving time to D/C and cost – no change in safety
 vrs Standard Assessment. Told EP if <100 CHF unlikely, >500 CHF likely, indeterminate. End Points: Time to D/C & Total Cost. Safety: Similar. Conclusion: BNP improved evaluation thereby improving time to D/C and cost – no change in safety.")
75
BNP strong prognostic indicator in symptomatic and asymptomatic individuals
Death or Cardiac Death Additive to LVEF

76
Cardiomyopathy

77
Case Previously well 10 year old girl presents with 2 weeks of progressive right sided ABD pain. General malaise. Mild fatigue on exertion. Parents report mild lethargy, pallor and decreased PO intake over same period. Shallow rapid breathing, worse when reclining at night. 37.8oC /54 Pale irritable HEENT: MMM. No adenopathy CVS: regular S1S2, no murmer, PPPx4, no edema CHEST: AE=AE slight decrease at bases ABD: palpable liver edge below umbilicus EKG: sinus tach, LAD, flattened T-waves, decreased voltages.

78
Post Myocarditis

79
Dilated Cardiomyopathy
Most common CM 30% idiopathic Hereditary X-linked (dystrophin gene) Booze Heavy Metal Drugs Infectious Viral Chagas Post partum Collagen vascular disease Glycogen storage disease Thiamine, PO4, zinc deficiency Amyloidosis Neuromuscular disorders
 Booze. Heavy Metal. Drugs. Infectious. Viral. Chagas. Post partum. Collagen vascular disease. Glycogen storage disease. Thiamine, PO4, zinc deficiency. Amyloidosis. Neuromuscular disorders.")
80
Dilated Cardiomyopathy
Biopsy helpful for etiology Rx same as other CHF MDC (Metoprolol in Dilated CM) 34% reduction in Death Multicenter Myocarditis Treatment Trial no benefit of corticosteroids and azathioprine for Rx of biopsy-proven inflammation in dilated CM
 34% reduction in Death. Multicenter Myocarditis Treatment Trial. no benefit of corticosteroids and azathioprine for Rx of biopsy-proven inflammation in dilated CM.")
81
HCM Inappropriate hypertrophy w/o stimulus Usually asymmetric
4% mortality per year (sudden death)
")
82
HCM 50% familial (Dominant Inheritance) Mechanism Abn Ca++ kinetics
Abn sympathetic stim Abn Coronaries Subendocardial ischemia Structural abn

83
HCM 25% 1st relatives of HCM Usually 3rd decade – not always M>F

84
HCM - Presentation Sudden Death Dysrhythmia CHF Presyncope / Syncope
Angina

85
HCM CHF Sx OE: ↑JVP – prominent “a” wave Double impulse pulse
PMI laterally displaced and increased SEM / HSM Split S2

86
HCM Genetic Studies ECG Echo LV outflow gradient >50mmHg
Diastolic dysfunction HOCM: septum >1.4:1 ratio to post wall

87
HCM – Approach/Mgmt ABCD Normal CHF / CAD Rx Myomectomy
Catheter septal ablation MV replacement ICD B-blockade CCB Anti-arrhythmias

88
Restrictive Least common CM Incidence – likely under diagnosed
Poor prognosis

89
Cardiomyopathy

90
Restrictive Idiopathic restrictive cardiomyopathy
EndoMyocardial Fibrosis Loeffler eosinophilic endomyocardial disease Secondary restrictive cardiomyopathy Radiation Hemochromatosis Amyloidosis Scleroderma Carcinoid heart disease Glycogen storage disease of the heart

91
Diagnosis Chest x-ray Electrocardiogram
Absence of cardiomegaly, normal cardiac silhouette CHF Electrocardiogram LBBB common, RBBB possible Low voltage Nonspecific ST-T changes Various arrhythmias Chamber enlargement

92
Echocardiography Normal to symmetrically thickened walls
Rapid early-diastolic filling, slow late-diastolic filling Normal or slightly reduced ventricular volume and systolic function

93
Cardiac catheterization
Elevated ventricular end-diastolic pressure Dip and plateau configuration of the diastolic portion of the ventricular pressure pulse Normal to slightly decreased ejection fraction Prominent x and y descent

94
Endomyocardial biopsy
May detect typical eosinophil infiltration in the inflammatory stage May detect myocardial fibrosis in later-stage cases Negative findings do not exclude diagnosis

95
Treat underlying cause if possible
Therapy similar for other causes of CHF Consider anticoagulation as prone to stasis thromboembolism

96
Thanks Shawn for the resources!

97
References Kostuk WJ. Congestive heart failure: what can we offer our patients? CMAJ 2001;165(8):1053-5 Schwam E. B-type natriuretic peptide for diagnosis of heart failure in emergency department patients: a critical appraisal. Acad Emerg Med 2004;11:

98
Risk of HF after AMI Jackson, G et al. BMJ 2000;320:167-170
Copyright ©2000 BMJ Publishing Group Ltd.

99
Looked like needed intubation 2 intubated
20 pts Pulmonary Edema Looked like needed intubation 2 intubated Also had COPD Mean Treatment Duration 2 ½ h

Similar presentations











 Class IV: symptoms at rest Class III: symptoms on less-than-ordinary exertion Class.>")





 CPP = aortic diastolic.>")



