Download presentation
Presentation is loading. Please wait.

1
Spasticity (and dystonia) from Neurology perspective Dr Ram Kumar Consultant Paediatric Neurologist Alder Hey June 2010
 from Neurology perspective Dr Ram Kumar Consultant Paediatric Neurologist Alder Hey June 2010")
2
Summary Spasticity (and dystonia) – what is it? Overview of treatment strategy Medications Botulinum toxin

3
Spasticity and dystonia management Overview of treatment strategy First confirm it is spasticity (or dystonia) Consensus on the appropriate use of ITB in paediatric spasticity. Eur J Paed Neurol 2009

4
“Legs feel stiff” - causes Is it a muscle or joint problem? Is it mainly a muscle pain/fatigue problem? Spasticity or dystonia = hypertonia aka increased muscle tone Neuromuscular conditions with increased tone e.g. myotonia Inflammatory conditions of joints + skin > muscles e.g. rheumatoid arthritis, scleroderma Joint and muscle contractures (due to any of the above, disuse)
.")
5
What is spasticity? One cause of increased muscle tone Resistance to passive muscle stretch at a joint Velocity and joint-angle dependent Has to be palpated – ie you need to lay on hands Other features: clonus, increased reflexes, upgoing plantars

6
Spasticity – classic muscles Classic lower limb muscle groups affected - the pyramidal pattern Ankle plantarflexors and invertors Knee extensors Hamstrings Hip flexors and adductors

7
Spasticity – classic muscles Classic upper limb muscle groups affected: Elbow flexors – biceps, brachialis, brachioradialis Forearm pronators – pronator teres Wrist flexors – Flexor carpi radialis, ulnaris Finger flexors (long) – Flexor Digitorum Superficialis and Profundus Thumb adductors – thenar group and adductor pollicis
 – Flexor Digitorum Superficialis and Profundus Thumb adductors – thenar group and adductor pollicis")
8
Upper limb spasticity pattern

9
Mechanisms of spasticity Additional aspects when spasticity arises in the developing brain and spinal cord Loss of descending fibres from the brain increases reflex fibres coming in at the spinal level

10
Co-existent muscle, tendon, joint, skin issues Muscle weakness i.e. “-paresis” and “-plegia” Lack of selective motor control Dystonia – sustained postures, active movements Fixed contractures Bone and joint deformities Skin problems – abrasions, Raynaud's Treating spasticity can improve, worsen or not change the above. And vice versa.

11
What is dystonia? Sustained postures Involuntary movements Incorrect timing of muscle activations Suggests active rather than passive movements Not usually velocity-dependent Very dependent on mental state: alertness, emotion

12
Types of dystonia Excessive movements: chorea, athetosis, dystonic tremor, myoclonus, “spasms” Decreased movements: extrapyramidal rigidity, hypokinesia

13
Muscle groups affected Oropharyngeal: mouth, tongue, pharynx, larynx Axial muscles: cervical, erector spinae (opisthotonus) Upper Limbs: Elbow extensor rigidity, fisting Lower limbs: Ankle evertors as well as invertors
 Upper Limbs: Elbow extensor rigidity, fisting Lower limbs: Ankle evertors as well as invertors")
14
Where dystonia comes from The basal ganglia controls aspects of voluntary, semi- voluntary and involuntary muscle activation and co- contraction And not to forget the cerebellum

15
Why bother treating spasticity - outcomes

16
Assessing impact of spasticity Sitting Walking, Splints - tolerability Posture control equipment - tolerability Other orthopaedic interventions Upper limb ADL Ease of cares Pain e.g. cramps, or agitation Sleep e.g. nocturnal cramps, need for repositioning Long term consequences - controversial

17
Check non-medication treatments in place

18
Focal and generalised spasticity

19
Intramuscular Botulinum toxin injection Treatment for focal and multi-focal hypertonia Reduces neuromuscular junction transmission Need to identify which muscles to inject and why Transient effect – good and bad features Good for localised therapy Relatively safe Different formulations and doses

20
Botulinum toxin – upper limb Goals of treatment – cares, function, splint tolerance, cosmetic Adjunctive therapies – splint, casting, OT, physio Assessment tools – AHA (bimanual), Melbourne Upper limb (unilateral), COPM, VAS with patient/parent defined goals (simpler) Good evidence of benefit with repeated injections May only need to repeat at 9 months or >1 year
, Melbourne Upper limb (unilateral), COPM, VAS with patient/parent defined goals (simpler) Good evidence of benefit with repeated injections May only need to repeat at 9 months or >1 year")
21
Botulinum toxin – lower limb Goals of treatment – pain relief, cares, walking,sitting, splint and other equipment tolerance Adjunctive therapies – splints, casts, physio, surgery Assessment tools – gait analysis, GMFM, VAS and parent/patient-defined goals Botulinum toxin does not prevent or treat musculoskeletal deformities – need surgery

22
Other focal and multi-focal therapy Intramuscular phenol injections Selective peripheral neurotomy Selective dorsal rhizotomy (more for generalised lower limb )
")
23
Focal and generalised spasticity

24
Spasticity Medication trials In cerebral palsy: Baclofen vs Placebo Dantrolene vs Placebo Other spasticity groups: Tizanidine vs Placebo Diazepam vs Amobarbital vs Placebo Gabapentin vs Placebo Diazepam vs Tizanidine Baclofen vs Tizanidine Dantrolene vs Placebo Baclofen vs Placebo

25
Baclofen Typical first-line medication GABA-B agonist Needs at lleast three times a day dose Use up to 2.5mg/kg/day Additional sleep inducing effects Main adverse effects: sleepiness, decreased trunk tone, ?seizures increased

26
Diazepam and similar Used to be first-line before baclofen GABA-A agonist Multiple effects e.g. anxiolytic, anticonvulsant Significant adverse effects e.g. respiratory depression Tolerance Start at low doses e.g. 0.1mg/kg/day

27
Dantrolene Works on muscle calcium-contraction coupling Not sedative effect of baclofen and diazepam Main adverse effect: liver failure or asymptomatic hepatic enzyme rises Problems not reported at 12mg/kg/day

28
Trihexyphenidyl Treatment for dystonic posturing (hypokinetic) Possibly for excessive movements as well Anticholinergic (muscarinic) Side effects of most anticholinergics: dry mouth (can be useful); behaviour change Start at 1mg bd; increase weekly by 0.1mg/kg/day to 1mg/kg/day as tds
 Possibly for excessive movements as well Anticholinergic (muscarinic) Side effects of most anticholinergics: dry mouth (can be useful); behaviour change Start at 1mg bd; increase weekly by 0.1mg/kg/day to 1mg/kg/day as tds")
29
Others L-DOPA preparations e.g. Sinemet Tetrabenazine Tizanidine Gabapentin Pregabalin Azumolene Clonidine Fampridine-SR

30
Spasticity and dystonia management

31
The updated European Consensus 2009 on the use of Botulinum toxin for children with cerebral palsy. Eur J Paed Neurol 2009

32
Spasticity and dystonia management: role of ITB

35
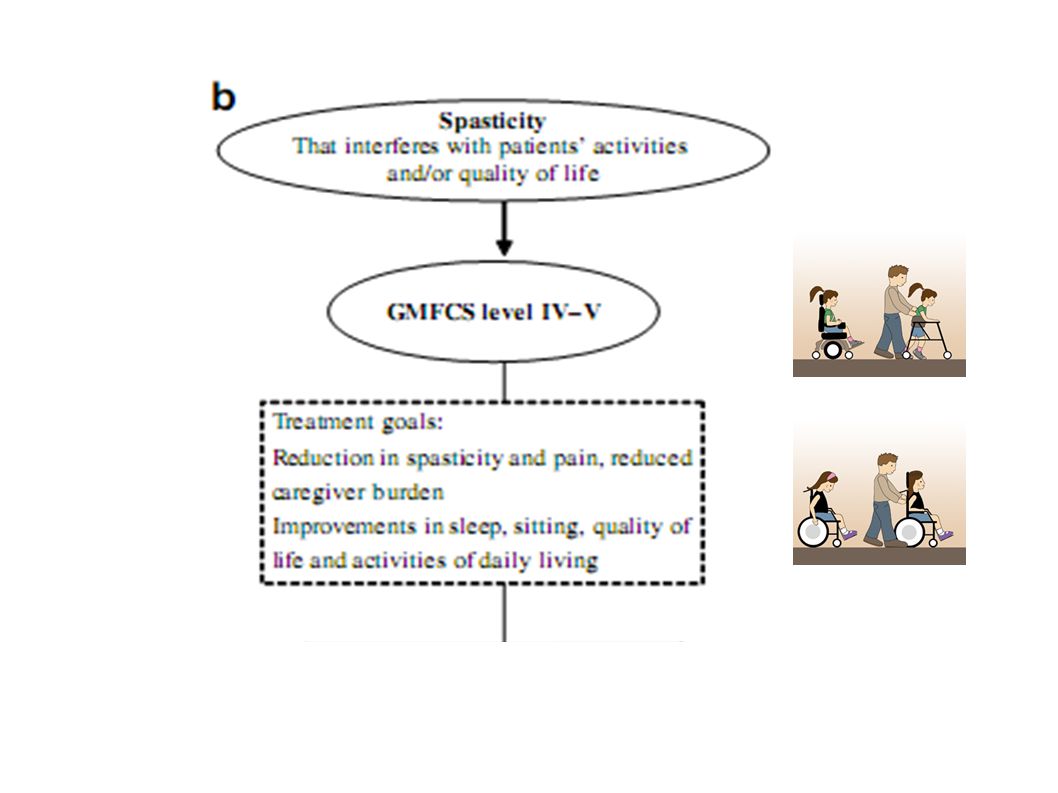
Reduce spasticity-related pain Improve sleep Aid posture management Reduce carer requirements Improve function eg upper limb Relief from adverse effects of oral medication Possibly improve age-dependent changes : contractures, joint deformities, respiratory problems Goals of treatment

36
Multidisciplinary including orthopaedic, physio, neurology, neurosurgery Co-morbidities Social factors Local factors (geography, adaptations) Physical impairment measures Care and comfort hypertonicity questionnaire (CCHQ) Paediatric Pain Profile (PPP) Evaluation
 Physical impairment measures Care and comfort hypertonicity questionnaire (CCHQ) Paediatric Pain Profile (PPP) Evaluation")
37
Case Study: SK 14 year old boy CP due to neonatal meningitis Asymmetric 4 limb spasticity, left worse Severe intellectual disability, blind Previous bilateral hip surgery ’03 Increasing pain 2 years – focal and general

38
Case Study: SK Baseline Paediatric Pain Profile scores (pre-ITB): Good day = 14 Hip pain = 50 Back pain = 26
: Good day = 14 Hip pain = 50 Back pain = 26")
39
Care and comfort questions

40
Spasticity and dystonia management Overview of treatment strategy Consensus on the appropriate use of ITB in paediatric spasticity. Eur J Paed Neurol 2009

Similar presentations



 PhD Consultant in Congenital Hand and Upper Limb Surgery Department.>")
 is a permanent physical condition.>")


 فلج مغزی.>")












