Download presentation
Presentation is loading. Please wait.

1
Mehdi Abbasi M.D Shariati hospital

2
P.P.F increases in frequency P.P.F often increase in osteoporotic bone, making stable fixation even more problematic

3
Mechanisms of injury Low-energy falls are the mechanisms of injury in most patients According to last Swedish registry at least 75% of P.P.F occur postoeratively Spontaneous P.P.F is more common after revision surgery High energy trauma accounts for only a small percentage of P.P.F and these types are associated with a more comminution

4
Mechanisms of injury Intraoperative P.P.F occur more commonly during revision procedures Given the predominance of low-energy injury mechanisms, associated injuries are uncommon

5
History History should include: Date of implantation Used prosthesis Arthroplasty complication such as infection Functional state of patient, any recent changes in status or symptoms related to the arthroplasty can be a clue to heighten suspicion of subtle P.P.F or prefracture implant loosening

6
Physical exam Prior surgical wound Presence or absence of associated lesions

7
Imaging A.P and lateral views of joint and full length of bones above and below the joint Attention should paid to fractures, prosthesis(loosening), osteolysis, cortical erosion cortical penetration and notching Diagnosis of intraoperative fractures can be from direct observation, but intraoperative radiograph should be obtained
, osteolysis, cortical erosion cortical penetration and notching Diagnosis of intraoperative fractures can be from direct observation, but intraoperative radiograph should be obtained")
8
Incidence and risk factor 300000 T.K.A per year 0.3% to 2.5% P.P.F in primary T.K.A Up to 38% P.P.F in revision T.K.A Patient-specific risk factors: R.A Osteolysis Osteopenic bone Frequent falls Technique-specific risk factors

9
Incidence and risk factors Osteopenia is a major contributing factor of P.P.F B.M.D in the distal of femur decrease 19-44% one year after T.K.A Stress fracture in the femur and tibia have been described after T.K.A. The patient complains of sudden pain without trauma and sign of infection Periodic X.R and early bone scan are diagnostic Local factors : osteolytic lesion, anterior femoral notching P.S femoral component increases risk for intraoperative fracture

10
Classification of P.P femur fracture Lewis and rorabek classification

11
Classification of P.P femur fracture Su et al classification

12
treatment Nonoperative treatment for displaced fractures has been associated with poor results. Internal fixation: traditional condylar buttress type plate is prone to complication Traditional fixed angle plate constructs such as condylar plate reduces varus collapse but have limited application. Modern methods of fixation, locked plating and retrograde nailing, provide superior results

13
treatment Bicondylar and unicondylar locked screw fixation provide excellent distal fixation. Retrograde intramedulary nailing can be applied to P.P.F that have adequate distal bone stock. It is preferred method by some authors.

14
Revision knee arthroplasty For patient with loose implant associated with a P.P.F or inadequate bone stock to achieve fixation, revision is considered In patient with a loose implant or a history of prefracture pain, occult infection should be ruled out. Revision T.K.A with intramedulary femoral stem that engage the diaphysis and simultaneously stabilize the fracture can be used Distal femoral replacement megaprosthesis have been used for salvage of failed internal fixation of P.P.F For a younger, active patient an allograft prosthetic composite may be a better alternative

15
Periprosthetic fracture of tibial and patella Incidence: They are less common than femoral side According to myoclinic joint registry (1999) incidence of P.P.F after primary T.K.A is 0.4% in the tibia 0.7% in the patella and 0.9% in the femur The frequency of P.P.F in revision surgery is higher
 incidence of P.P.F after primary T.K.A is 0.4% in the tibia 0.7% in the patella and 0.9% in the femur The frequency of P.P.F in revision surgery is higher")
16
Patella Patellar fracture is the second most frequent P.P.F around the knee. About 12% of reported fractures were directly associated with trauma. The remaining occurred spontaneously and most fractures occur during first 2 years after arthroplasty. Etiologic factors specific to the patella are component design, excessive resection of bone, limb and prosthesis alignment and lateral release.

17
Classification of patellar fractures ClassificationType IType IIType IIIaType IIIb Extensor mechanism IntactDisruptedIntact Implant fixationWell-fixed Well-fixed or loose Loose Bone stockUnspecified ReasonablePoor

18
Classification of Tibial fractures ClassificationType IType IIType IIIType IV Fracture location Tibial plateau Adjacent to stem Distal to prosthesis Tibial tubercle Subtype A Prosthesis well- fixed BProsthesis loose CIntraoperative

20
Patellar fracture treatment Patellar fracture treatment: no operative – ORIF – component resection patellectomy. When extensor mechanism is intact, conservative management is recommended. Surgical management is reserved for disturbance of extensor mechanism integrity, a loose patellar component and patellar maltracking. ORIF with T.BW or cerclage wiring results in nonunion with an average nonunion rate of 82% Therefore operative management is not an unreasonable consideration even in the face of a disrupted extensor mechanism.

21
Patellar fracture treatment The presence of fracture and a loose implant is associated with high complication rates regardless of treatment method. When there is adequate bone stock (>10mm) revision of the patellar component is reasonable. Severe bone loss mandates patellar resection arthroplasty. Extensor lag about 10˚ and a limitation of 20˚-30˚ of flexion are common.
 revision of the patellar component is reasonable. Severe bone loss mandates patellar resection arthroplasty. Extensor lag about 10˚ and a limitation of 20˚-30˚ of flexion are common..")
22
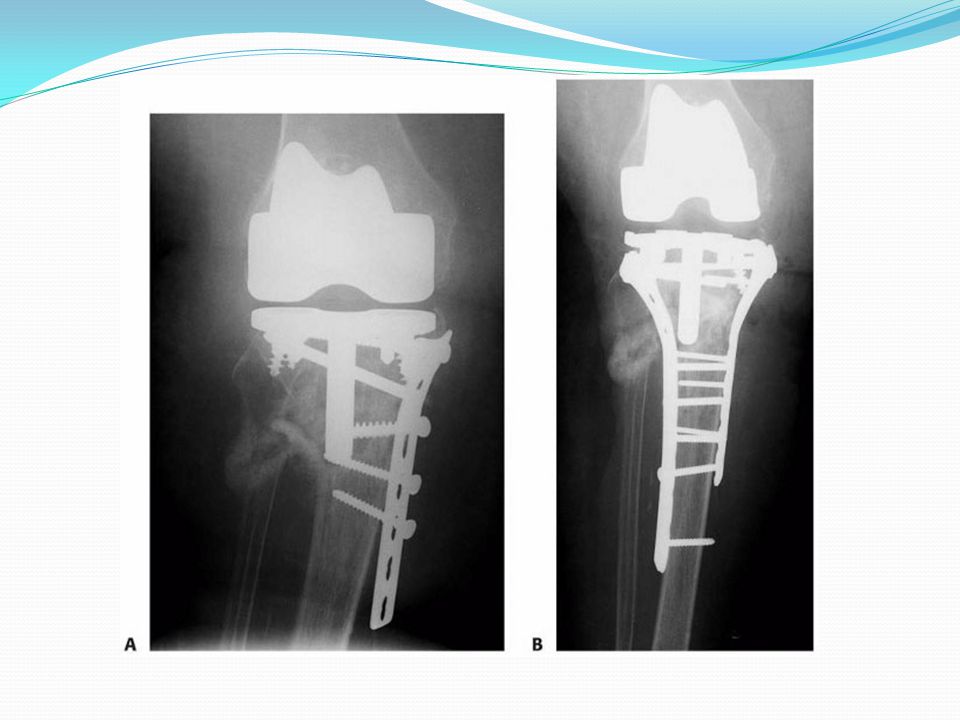
TIBIA P.P.F of tibia are uncommon Most often they are associated a loose tibial component therefore revision is preferred in these situations. Tibial revision for P.P.F requires the routine use of stem end augment and metaphysical filling metal implants. The surgeon should be aware that isolated tibial component revision is rare, and commonly, should be prepared to revise the entire arthroplasty. When arthroplasty component is stable, locked plate is preferred method of treatment.

Similar presentations