Download presentation
Presentation is loading. Please wait.

1
Postpartum Hemorrhage Dr.Ghassan A. Barayan, MBBS
Management of Postpartum Hemorrhage Done by Group C2 Presented by : Dr.Ghassan A. Barayan, MBBS

2
Case Hx G5 P4 + 0 lady , in active labour pain . Admitted to the hospital and she delivered a 3.8 kg baby. Immediately after the placental delivery she had heavy vaginal bleeding . DDX management

4
Maternal mortality Hemorrhage Infection Hypertension Thromboembolism
The single most Important cause of Maternal death Every year, women die because of postpartum hemorrhage – one every 4 minutes

5
Definition Estimated blood loss with vaginal delivery: > 500cc
Estimated blood loss with C/S: > 1000cc 1ry : within 24h after delivery 2ndry : after 24h up to weeks

6
Avoid underestimating significant bleeding
Don’t underestimate EBL Don’t disregard slow but unrelenting trickle If signs of shock* without high EBL, must consider hidden bleeding (internal injury, hidden hematoma) Requires urgent treatment
 Requires urgent treatment.")
7
A 60 kg pregnant has 6L of blood volume at 30 weeks

8
Epidemiology Incidence : 4 % 88 % of deaths are seen in the first 4 hrs Abdominal or pelvic bleeding can be hidden

9
Early postpartum hemorrhage causes
Uterine atony Genital tract trauma Retained placental tissue Low placental implantation due to relative musculature in the LUS so insufficient control of bleeding Uterine inversion Coagulation disorders Abruptio placentae Amniotic fluid embolism Retained dead fetus Inherited coagulopathy

10
Four “Ts”* Tone . . . . . . - Uterine atony
Tissue Retained products Trauma Tears, abrasions Thrombin Clotting disruptions

11
Clinical presentation
The patient whether presents with Vaginal Bleeding OR Severe hypovolemic shock

12
“Tone: Think of Uterine Atony”
Uterine atony causes 80% of hemorrhage failure of uterus to contract after placental separation

13
Hx : identify risk factor
Uterine overdistention: -multiple gestation polyhydromnios fetal macrosomia Prolonged oxytocin administration Prolonged labor Precipitous labor (last <3h ) Halogenated anesthesia Magnesium sulfate ttt of pre-eclampsia Chorioamnionitis Uterine fibroids Grand multiparity
 Halogenated anesthesia. Magnesium sulfate ttt of pre-eclampsia. Chorioamnionitis. Uterine fibroids. Grand multiparity.")
15
Bimanual Uterine Exam Confirms diagnosis of uterine atony: the fundus is soft “ boggy “ , poorly contracting

16
Initial Assessment (orders)
Remember ABCs Check the vitals and correct the shock state Start a large-bore IV Obtain CBC Platelet count , PT , PTT Blood crossmatch (keep 4 units of packed RBCs in hand ) IV infusion of norm.saline or ringer lactate (it’s best to avoid glucose containing fluids) 3ml of crystalloid / ml of EBL
 IV infusion of norm.saline or ringer lactate (it’s best to avoid glucose containing fluids) 3ml of crystalloid / ml of EBL.")
17
Initial Assessment (orders).cont.
Insert urethral catheter to monitor urine output Blood and blood product transfusion may be required if blood loss is continuing, if the blood volume lost is over 30%, or if the patient’s clinical status reflects developing shock despite aggressive resuscitation

18
Management Bimanual Uterine massage is often adequate for stimulating uterine involution. medications

19
Oxytocin ( pitocin ) promotes rhythmic contractions of the upper uterine segment Give IM or IU, no rapid IV infusion (Can cause BP) 10 – 40 U in 1 L NS at 250cc/h. / IV Can get Antidiuretic effect in very high doses

20
Methylergonovine Methergine 0.2 mg IM only Max. of 3 doses
contracts both upper and lower uterine segments tetanically causes vasoconstriction and hypertension contraindicated in hypertension side effects: HTN, nausea, vomitting

21
Prostaglandins F2 Hemabate 0.25mg intramyometrial q 15min
Rapid response 3-10 minutes Max. 8 doses Avoid in asthmatic patients. This is 80% to 90% effective in stopping PPH in cases that are refractory to oxytocin and ergometrine

22
misoprostol Cytotec Recent data indicates that it can be used as 1st line 800 – 1000 mcg rectally

23
Other measures Uterine packing or tamponade
When uterotonic agents fail Useful in cases of placenta praevia or accreta Either gauze or Foley, Sangestaikin blakemore tube Recent reports of large series have confirmed the high success rates of balloon devices Uterine artery embolization by placing angiocatheter and injecting thrombogenic material

24
Embolization

25
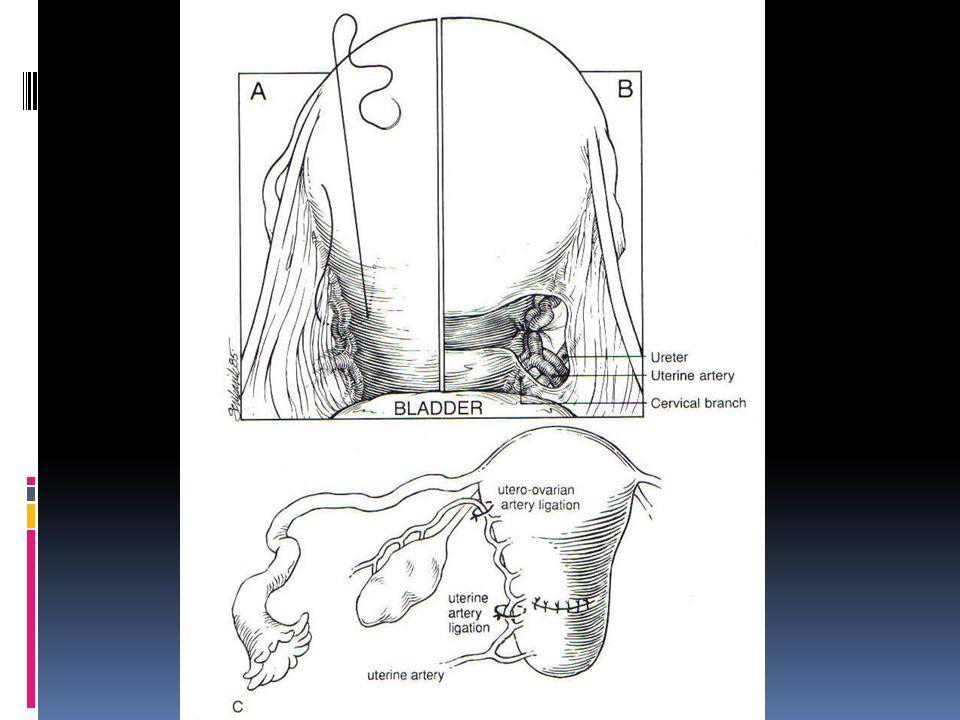
Exploratory laparotomy :
B-lynch technique : effective in uterine atony Bilateral uterine artery ligation Hypogastric artery ligation Suprecervical or TAH is the definitive treatment for intractable PPH

28
Human recombinant factor VIIa
New treatment to control severe , life threatening hemorrhage It acts on the extrinsic clotting pathway Cessation of bleeding occurs in minutes

31
2-Tissue: Retained placenta
Prolong 3rd stage of delivery( > 30 minutes) seen in ~ 6% of deliveries. Prior retained placenta. Prior manual removal of placenta Prior C/S, curettage p-pregnancy, uterine infection, and increased parity. Prior C/S scar & previa (25%) Most patients have no risk factors.
 seen in ~ 6% of deliveries. Prior retained placenta. Prior manual removal of placenta. Prior C/S, curettage p-pregnancy, uterine infection, and increased parity. Prior C/S scar & previa (25%) Most patients have no risk factors.")
32
US evaluation of retained tissue should be performed before uterine instrumentation

33
Brandt-Andrews maneuver
To determine if the placenta has separated Firm traction is applied to the umbilical cord with one hand while the other applies suprapubic counterpressure

34
Abnormal adherent placenta
Caused by missing or defective decidual layer . Placenta Accreta: Placenta adherent to myometrium. Placenta Increta: myometrial invasion. Placenta Percreta: penetration of myometrium to or beyond serosa.

35
Placenta Accreta: Most common type.
With incidence of % if previous C/S or previa The incidence increase as the no. of previous C/S increased Prior uterine surgery and placenta praevia in the current pregnancy r 2 important RF – US and color doppler TAH is the definitive treatment

36
Placenta accreta and uterine atony are the 2 commonest causes of postpartum hysterectomy

37
Removal of Abnormal Placenta
Oxytocin 10U in 20cc of NS placed in clamped umbilical vein. If this fails, get OB assistance. Check Hct, type & cross 2-4 u. Two large bore IVs. Anesthesia support.

38
Removal of Abnormal Placenta
Relax uterus with halothane general anesthetic and subcutaneous terbutaline. Bleeding will increase dramatically. With fingertips, identify cleavage plane between placenta and uterus. Keep placenta intact. Remove all of the placenta.

41
Removal of Abnormal Placenta
If successful, reverse uterine atony with oxytocin, Methergine, Hemabate. Consider surgical set-up prior to separation. If manual removal not successful, large blunt curettage or suction catheter, with high risk of perforation, so to be done on US guidance Consider prophylactic antibiotics.

43
Trauma (3rd “T”) (cervical, vaginal and preineal laceration) Suspected if bleeding persists and uterine fundus is contracting. Episiotomy Hematoma Uterine inversion Uterine rupture In C/S LT laterl extension of the incision can damage ascending branches of the uterine a while inferior extension damages the cervical branches.
 Suspected if bleeding persists and uterine fundus is contracting. Episiotomy Hematoma Uterine inversion Uterine rupture In C/S LT laterl extension of the incision can damage ascending branches of the uterine a while inferior extension damages the cervical branches.")
44
Genital tract Trauma Risk factors include: Instrumented deliveries forceps or vaccum. Primiparity. Pre-eclampsia. Multiple gestation, fetal macrosomia. Prolonged second stage, precipitous delivery VBAC Clotting abnormalities.

45
Repair of cervical laceration
At the two lateral angles while dilating the first stage. Repair lacerations quickly. Place initial suture above the apex of laceration to control retracted arteries.

46
Vulvar Hematomas more likely w/ operative vaginal deliveries and episiotomies excessive unilateral swelling and pain Hematomas less than 3cm in diameter can be observed expectantly. If larger or expanding , incision and evacuation of clot is necessary. Irrigate and ligate bleeding vessels. With diffuse oozing, perform layered closure to eliminate dead space. Broad spectrum antibiotics should be given

47
Limited from spread by fascia lata
Central tendon of the perineum prevents it from crossing the midline

48
Uterine rupture association

49
Retroperitoneal heamtoma
more likely after C/S delivery – symptom may be shock, excess flank pain.

50
Uterine Inversion Rare: ~1/2500 deliveries
Turning inside out of the uterus C/F: Acute abdominal pain Blue-gray mass protruding from vagina. Suspect if shock disproportionate to blood loss

51
Causes include: Uterine atony.
Excessive traction on cord while exerting fundal pressure before complete placental separation Manual removal of the placenta Abnormal placentation Uterine anomalies

52
Hypotension worsened by vaso-vagal reaction.
Avoid excessive cord traction, and always guard the uterus when applying traction Hypotension worsened by vaso-vagal reaction. Consider atropine 0.5mg IV if bradycardia is severe.

54
Uterine Inversion: Replace through Cervix

55
Uterine Inversion: Restitution

56
If replacement is unsuccessful :
Uterine relaxant agents like NG IV ( 100 ug ) , Terbutaline, MgSO4
 , Terbutaline, MgSO4.")
57
Uterine Rupture Complete separation of the uterine wall
Incidence is 0.5 % Prior scar in 40 %

58
Risk factors include: Prior C/S Prior uterine surgery, myomectomy
Classical : 4-7 % Lower transverse < 1 % Prior uterine surgery, myomectomy Hyperstimulation with Oxytocin Trauma. Breech version and extraction Abruptio placenta Uterine manipulation during labor ”Forceps delivery, intra –uterine pressure cath insertion” Parity > 4. spontaneous

59
Uterine Rupture Suspect if: Rx : sudden change in FHR tracing
Fetal parts easily palpated abdominally Fetal bradycardia in 50 – 70 % of cases vaginal bleeding abdominal tenderness maternal tachycardia signs of shock are out of proportion to visible blood loss R/O abruptio placenta Rx : ABCs. IV fluids. Immediate laparotomy and deliver the infant and repair the scar

61
Thrombosis (4th “T”) Coagulopathies are rare.
Pre-existing conditions (congenital) ITP, von Willebrands Obstetric-related Hypertensive disorders, HELLP Abruption Fetal demise Sepis Drugs (e.g. aspirin) Suspect if oozing from puncture sites noted. Work up with platelets, PT, PTT, fibrinogen level, fibrin split products, and possibly antithrombin III.
 ITP, von Willebrands. Obstetric-related. Hypertensive disorders, HELLP. Abruption. Fetal demise. Sepis. Drugs (e.g. aspirin) Suspect if oozing from puncture sites noted. Work up with platelets, PT, PTT, fibrinogen level, fibrin split products, and possibly antithrombin III.")
62
Maintain: Fibrinogen > 100mg/dl with FFP
Platelets > 50,000 with packed platelets Hematocrit > 30% with PRBCs

63
AFE 1/20.000 pregnancies Causes 10 % of maternal deaths in US
Mortality rate is 80 % S & S : Hypoxia Hypotension and shock Altered mental status DIC Bronchospasm Clinical diagnosis Labs : ABG, electrolytes, CBC and coagulation profile Definitive diagnosis is demonstrating the fetal squamous cells and lanugo in the pulmonary vascular space

64
Rx : ABC Intubation IV access with volume support, inotropic agents and pressors PRBC and FFP as coagulopathy risk is 50 % in the first 2 hrs.

65
Management of excessive bleeding once vitally stable
Regardless of the cause, replacing RBC mass is mandatory 2 iron tablets ( each 300 mg ) PPH in subsequent pregnancies occurs in 10 %
 PPH in subsequent pregnancies occurs in 10 %")
66
Wait We are almost done

67
Late postpartum hemorrhage
It complicates 1 % of pregnancies Late hemorrhage is more likely due to: Subinvolution of the uterus. Endometritis. Uterine fibroid Retained placental fragment. Coagulopathy and blood dyscariasis VWD is present in % of adults with menorrhagia as pregnancy elevates factor 8 level, and drops postpartumply Treatment : ( depend on the cause ) Uterotonic agents Antibiotics Currettage
 Uterotonic agents. Antibiotics. Currettage.")
68
Complications RF Blood transfusion reaction Sheehan’s syndrome :
Failure of lactation Amenorrhea Superinvoluted uterus

69
Prevention Active Management of 3rd stage of labour
Oxytocic is given Cord is clamped Placenta delivered by controlled cord traction (CCT) with counter-traction on the fundus Fundal massage evidence supports use of oxytocin after delivery of anterior shoulder, or more commonly in the U.S after the delivery of the placenta Strong research support for use of post partum administration of pitocin
 with counter-traction on the fundus. Fundal massage. evidence supports use of oxytocin after delivery of anterior shoulder, or more commonly in the U.S after the delivery of the placenta. Strong research support for use of post partum administration of pitocin.")
70
Summary: Remember 4 Ts Tone Tissue Trauma Thrombin

73
Thank You

Similar presentations














: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")

 产后出血 林建华. Major causes of death for pregnancy women ( maternal mortality) Postpartum hemorrhage ( 28%) heart diseases pregnancy-induced.>")


 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")






 Dr. Abdalla H. Elsadig MD.>")




