Download presentation
Presentation is loading. Please wait.

1
Obstetric Hemorrhage Anne McConville, MD
This is a big topic, could likely be several lectures. Remains today the leading cause of maternal death worldwide, mostly due to developing countries. Severe hemorrhage occurs in 4-5/1000 deliveries and in US is 3rd leading cause of maternal death, with leading cause being hypertensive disorders of pregnancy and sepsis. Recent UK study showed that 64% of maternal deaths were associated with substandard care, most commonly was failure to recognize extent of blood loss and to institute treatment quickly. There are many causes of hemostasis and hemorrhage and we will try to touch on may of these.

2
The Direct leading cause of pregnancy related mortality in the United States is
A) Failed Intubation B) Hemorrhage C) Thromboembolism D) Hypertensive disorders of pregnancy E) Infection
 Failed Intubation. B) Hemorrhage. C) Thromboembolism. D) Hypertensive disorders of pregnancy. E) Infection.")
3
Cesarean Delivery is associated with a blood loss of about:
A) 100 mL B) 250 mL C) 500 mL D) 750 mL E) 1000 mL
 100 mL. B) 250 mL. C) 500 mL. D) 750 mL. E) 1000 mL.")
4
Estimated Blood Loss During Parturition
Average EBL during NVD = 600 mL Average EBL during CS = 1000 mL Physiologic changes of pregnancy help to diminish the effects What physiologic changes help diminish these effects? Physiologic anemia (bleed lower HCT), increased blood volume, autotransfusion, hypercogulable state of pregnancy. We always see OB docs trying to minimize EBL, but the are full of crap, we need to be quick to recognize excessive bleeding because maternal and fetal outcomes depend on this.
, increased blood volume, autotransfusion, hypercogulable state of pregnancy. We always see OB docs trying to minimize EBL, but the are full of crap, we need to be quick to recognize excessive bleeding because maternal and fetal outcomes depend on this.")
5
30 y.o. G2P1 at 28 weeks gestation presents with an episode of brisk vaginal bleeding. She denies having pain. She has had 1 prior C/S. The most likely diagnosis is: A) Placental abruption B) Uterine Rupture C) Cervicitis D) Placenta Previa E) Abdominal trauma
 Placental abruption. B) Uterine Rupture. C) Cervicitis. D) Placenta Previa. E) Abdominal trauma.")
6
Placenta Previa Anterpartum vaginal bleeding may occur in 20% of pregnant women and most are not life threatening and most occur during the 1st trimester. The greatest risk of antepartmum hemorrhage is not to mom but to baby. 2nd and 3rd trimester bleeding used to be associated with neonatal mortality of up to 80% but now is much lower (2.3% of previa and 12% of abruptions). Placenta previa defined palcental implantation in advance of fetal presentation, with some degree of encroachment on the cervical os. PP occurs in about 3.5/1000 pregnancies. Previous uterine trauma seems to possible etiology and scars on the uterus as well lead implantation to occur in lower segment. Risk factors include multiparity, AMA, previous c/s or other uterine surgery and previous PP. PP carries increased risk of C-hyst. Hallmark of PP is painless bleeding in 2nd or 3rd timester (sentinel bleed, usually resolves). Fetal or maternal compromise is unlikely during first episode.
. Placenta previa defined palcental implantation in advance of fetal presentation, with some degree of encroachment on the cervical os. PP occurs in about 3.5/1000 pregnancies. Previous uterine trauma seems to possible etiology and scars on the uterus as well lead implantation to occur in lower segment. Risk factors include multiparity, AMA, previous c/s or other uterine surgery and previous PP. PP carries increased risk of C-hyst. Hallmark of PP is painless bleeding in 2nd or 3rd timester (sentinel bleed, usually resolves). Fetal or maternal compromise is unlikely during first episode.")
7
The next step in management of patient from question 3 is:
A) Proceed to OR for prompt cesarean delivery B) Large bore IV access, fluid resuscitation and transvaginal ultrasound C) Cervical exam followed by induction of labor with cytotec and pitocin. D) Fetal non-stress test and BPP E) MRI
 Proceed to OR for prompt cesarean delivery. B) Large bore IV access, fluid resuscitation and transvaginal ultrasound. C) Cervical exam followed by induction of labor with cytotec and pitocin. D) Fetal non-stress test and BPP. E) MRI.")
8
Management of Placenta Previa
Abdominal or transvaginal ultrasound mainstay of diagnosis. Maternal resuscitation Fetal monitoring by NST and BPP Betamethasone to accelerate fetal lung maturity Tocolytic therapy in selected patients TV better for posterior placentas. Digital cervical exams are avoided due to possible placental trauma and need for emergent c/s. Mother should be resuscitated via large bore IV access and transfused as needed. Betamthasone or corticosteroid given to parturients between weeks gestation PP may be associated with preterm labor and uterine contractions/irritability may provoke more bleeding, however tocolytics have CV side effects. Risk of these effects should be weighed and should not be given to those in with uncontrolled hemorrhage or if the diagnosis could be abruption. Tocolytic choice varies but studies now show that CCB’s may be as effective as Mag and B-agonists with fewer side effects

9
Anesthetic Management of Placenta Previa
Assess airway, volume status, and presence of ongoing bleeding Large bore IV access, baseline HCT, T&C With the exception of marginal placenta previa, Cesarean delivery will be performed Neuraxial vs. General anesthesia Prepare to treat intraoperative hemorrhage Marginal previa that is 2cm from cervical os may attempt vaginal delivery. Most OB anesthesiologists prefer neuraxial whereas non-ob anesthesiologists tend to prefer GA. Studies have actually shown that during C-hyst for previa, there was less blood loss with neuraxial than GA. Why do PP hemorrhage I during c/s? Normal implantation, just in the wrong spot, right? Surgeon may cut through placenta if it is anterior previa, may actually require classical C/S Lower uterine segment does not contract as well as fundal implantation site The are risk for placenta accreta, both independently and because previa is a risk of C/S If GA chosen, must remember this risk of atony because of implantation in less contractile LUS and avoid volatile agents as much as possible.

10
D) Placental Abruption E) Cervicitis
32 y.o. G5P4 presents at 38 weeks with vaginal bleeding. She was having contractions that have subsided. She has had 3 prior classical C/S. FHR tracing shows FHR 108 and minimal variability. The most likely diagnosis is: A) Placenta Previa B) Placenta Accreta C) Uterine Rupture D) Placental Abruption E) Cervicitis
 Placenta Previa. B) Placenta Accreta. C) Uterine Rupture. D) Placental Abruption. E) Cervicitis.")
11
Uterine Rupture This can be disatstrous to mother and baby. Quite rare, less than 1 % even in those with a scarred uterus. In women with unscarred uterus likely cause is trauma with forceps delivery, macrosomia, long augmented labor, external version, penetrating wound or blunt trauma, grand multiparity, uterine anomoly Most common type of rupture is dehiscence of previous scar, not full thickness, does not cause FHR abnormalities, and does not require emergency C/S. 23 cases of catastrophic rupture associated with 35%mortality. Anesthetic management often necessitates GA unless the patient already has an existing epidural the the rupture occurs during labor. Interestingly, rupture of unscarred uterus morel likely to require transfusion. Hysterectomy definitive treatment as the risk of rupture will remain in future pregnancies.

12
D) Placental Abruption E) Vasa Previa
32 y.o. G3P2 at 31 weeks gestation presents with brisk vaginal bleeding, abdominal pain, and contractions. No history of previous uterine surgery. What is the most likely diagnosis: A) Placenta Accreta B) Placenta Previa C) Placenta Percreta D) Placental Abruption E) Vasa Previa
 Placenta Accreta. B) Placenta Previa. C) Placenta Percreta. D) Placental Abruption. E) Vasa Previa.")
13
Placental Abruption Defined as complete or partial separation of the placenta that is normally implanted before delivery. Fetal compromise occurs due to loss of placental surface area available for exchange Risk factors include tob, cocaine, HTN, AMA, preeclampsia, previous abruption, advanced parity % of pregnancies, higher incidence in black women Usual triad is as this patient had, sometimes bleeding may be concealed and present only as preterm labor and NRFHT’s Maternal hypotension may be present. Complications include shock, ARF, DIC, IUGR Risk to fetus is hypoxia and prematurity

14
What is the most appropriate next step in the management of the patient from question 6?
A) Prompt C/S under GETA B) Large bore IV access, volume resuscitation and fetal monitoring C) Induction of labor with cytotec followed by oxytocin D) Epidural analgesia, BPP, followed by C/S E) Abdominal ultrasound followed by observation if no abruption present
 Prompt C/S under GETA. B) Large bore IV access, volume resuscitation and fetal monitoring. C) Induction of labor with cytotec followed by oxytocin. D) Epidural analgesia, BPP, followed by C/S. E) Abdominal ultrasound followed by observation if no abruption present.")
15
Management of Placental Abruption
Maternal Resuscitation, LUD, Oxygen, Urinary catheter Continuous FHR monitoring Laboratory studies, T&C Timing and route of delivery determined by maternal and fetal status Anesthesiologist must consider severity of abruption and urgency of delivery when planning anesthetic Neuraxial vs. GETA Prepare to treat coagulopathy Coexisting uterine atony may also compound bleeding at delivery In less severe abruptions without evidence of maternal and fetal compromise, may allow pregnancy to continue after steroids and with close observation and frequent fetal monitoring. In patient is term and/or stable to undergo IOL, epidural analgesia is not contraindicated. In many cases, the fetal and maternal status are critical, necessitating GETA. Occasionally abruptions occur during labor with an existing epidural in which case it may be used for cesarean section. When performing emergency GETA in patient with abruption, thiopental and propofol should be avoided as may precipitate profound hypotension and unmask severe hypovolumia. Etomidate or Ketamine would be more appropriate choices. Volume management occasionally may require arterial and central venous catheters. Treat atony with uterotonic agents. Side note: Vasa Previa is velementous insertion of fetal vessels such that the fetal vessels overlie the cervical os. In this case the fetal vessels are not protected by umbilical cord or placenta and are subject to tear if membranes are ruptured resulting in fetal hemorrhage. 1/2500 deliveries, no threat to mother. Fetal mortality is 50-75% (highest of of pregnancy complication). Fetus has oly ml/kg of blood so very little blood loss results in fetal exsanguination. Associated with multiple gestation (triplets). Suspect when bleeding accompanies ROM followed by NRFHT’s. elective delivery at 36 weeks with hospitalization at weeks.
. Fetus has oly ml/kg of blood so very little blood loss results in fetal exsanguination. Associated with multiple gestation (triplets). Suspect when bleeding accompanies ROM followed by NRFHT’s. elective delivery at 36 weeks with hospitalization at weeks.")
16
Which of the following is NOT a treatment for Uterine Atony?
A) Uterine massage B) Uterine balloon tamponade C) Nitroglycerin D) Uterine compression suture E) Misoprostol
 Uterine massage. B) Uterine balloon tamponade. C) Nitroglycerin. D) Uterine compression suture. E) Misoprostol.")
17
Uterine Atony Most common cause of severe PPH
Most common indication for peripartum transfusion Uterine contraction primary mechanism of hemostasis Risk factors include: Multiparity, macrosomia, long labor, augmented labor, precipitous labor, chorioamnionitis, polyhydramnios, tocolytic agents, volatile halogenated anesthetics, fibroids Uterine atony is failure of primary hemostasis mechanism. Parturients with hemorrhage may have UA that are unresponsive to vasoconstrictors Basically, anything that stretches the uterus may result in atony Previous PPH also a risk factor

18
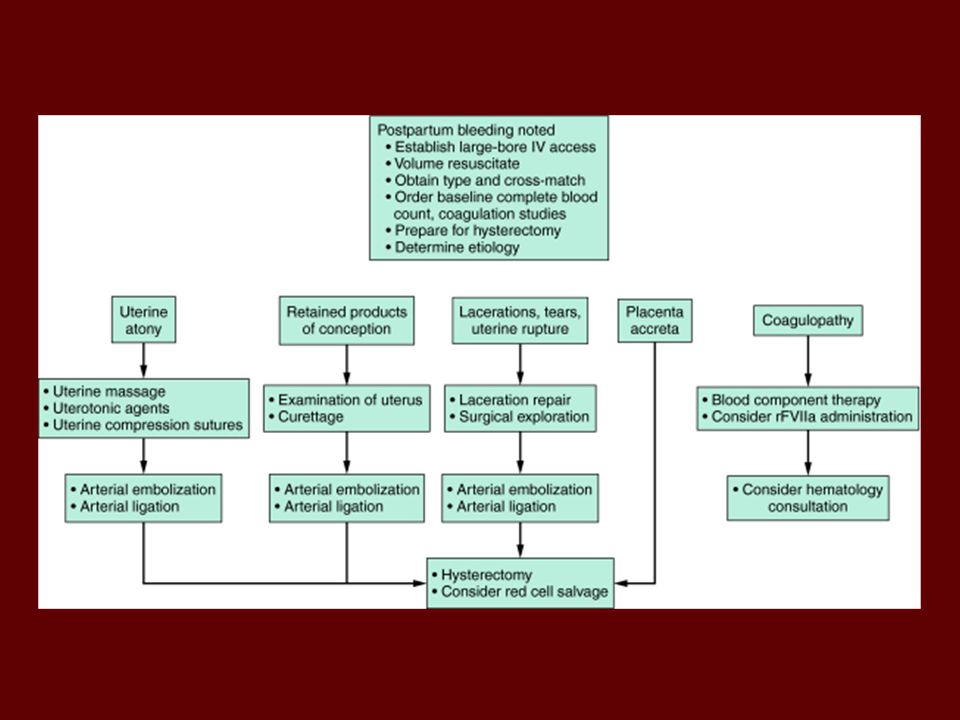
Management of Uterine Atony
Pharmacologic Oxytocin Methylergonovine 15-Methylprostaglandin F2α Misoprostol Surgical Uterine Massage Uterine Compression Suture Uterine Balloon tamponade Arterial Ligation Hysterectomy Radiologic Uterine artery embolization What is max concentration of Pit? What are side effects of Pit? Any contraindication? Why infusion? What is methergine dose? Route? In whom is it contraindicated? Side effects (N/V, arteriolar constriction, thromboembolic events). How often can give it? Hemebate dose? Who is it contraindicated? Route? Side effects (bronchoconstriction, temp elevation, diarrhea, shivering). How often? Cytotec? Route? Dose ( mcg per rectum). Off label use. Side effects (same as hembate, both prostaglandins)
. How often can give it Hemebate dose Who is it contraindicated Route Side effects (bronchoconstriction, temp elevation, diarrhea, shivering). How often Cytotec Route Dose ( mcg per rectum). Off label use. Side effects (same as hembate, both prostaglandins)")
19
B-Lynch Suture

20
Bakri Balloon

21
C) Placental Abruption D) Uterine Atony E) Placenta Accreta
40 y.o. G4P2 with low-lying placenta diagnosed during pregnancy experiences hemorrhage during repeat C/S. She has had 2 prior C/S. Other history includes D&C for miscarriage. The uterus appears to be contracting. The most likely diagnosis is: A) Retained Placenta B) Placenta Previa C) Placental Abruption D) Uterine Atony E) Placenta Accreta
 Retained Placenta. B) Placenta Previa. C) Placental Abruption. D) Uterine Atony. E) Placenta Accreta.")
22
Placenta Accreta Defined as abnormally adherent placenta.
3 variants of same process. Rising incidence with increasing c/s rate. Greatest risk with placenta previa in setting of prior C/S. Now the leading cause of cesarean hysterectomy. Diagnosed with suspicion on ultrasound…see placenta lacunae, loss of retroplacental clear space, loss of demarcation between bladder and uterus. Gold standard treatment is hysterectomy. Conservative measured have been tried.

23
Normal placenta

24
Placenta Accreta

25
Relationship Between Placenta Previa and Cesarean Section with Placenta Accreta

26
A) Retained Placenta B) Uterine Inversion C) Uterine Atony
An 18 y.o. G2P1 experiences hemorrhage in the labor room after vaginal delivery of a preterm infant at 28 weeks gestation. She had 1 D&C previously for miscarriage. On visual inspection there appears to be genital trauma. The most likely diagnosis is: A) Retained Placenta B) Uterine Inversion C) Uterine Atony D) Uterine Rupture E) Placenta Accreta
 Retained Placenta. B) Uterine Inversion. C) Uterine Atony. D) Uterine Rupture. E) Placenta Accreta.")
27
Retained Placenta A major cause of PPH 3.3% of all deliveries
Placenta separates in fragments Can be life-threatening Involves manual removal vs. D&C Neuraxial vs. General Uterine relaxation may be requested

28
Uterine Inversion Rare but disastrous event 1/5,000-10,000 delivered
Risk factors include: uterine atony, fundal pressure, excessive umbilical cord traction, short umbilical cord, uterine anomalies May be incomplete (not visible) Treatment is immediate replacement Anesthetic usually involves uterine relaxation followed by uterine contraction with oxytocin Replace before placenta removed
 Treatment is immediate replacement. Anesthetic usually involves uterine relaxation followed by uterine contraction with oxytocin. Replace before placenta removed.")
29
All of the following are associated with DIC except:
A) Placenta Accreta B) Placenta Previa C) Placental Abruption D) Dead Fetus Syndrome E) Amniotic Fluid Embolism
 Placenta Accreta. B) Placenta Previa. C) Placental Abruption. D) Dead Fetus Syndrome. E) Amniotic Fluid Embolism.")
31
Monkeys

Similar presentations


: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")


 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")













