Download presentation
Presentation is loading. Please wait.

1
Wrist and Hand

2
Wrist and Hand Bones Wrist (Carpals) Hand Scaphoid (Navicular) Lunate
Triquetral Pisiform Trapezium Trapezoid Capitate Hamate Hand Phalanges Thumb Proximal and distal Fingers DIP PIP MIP

4
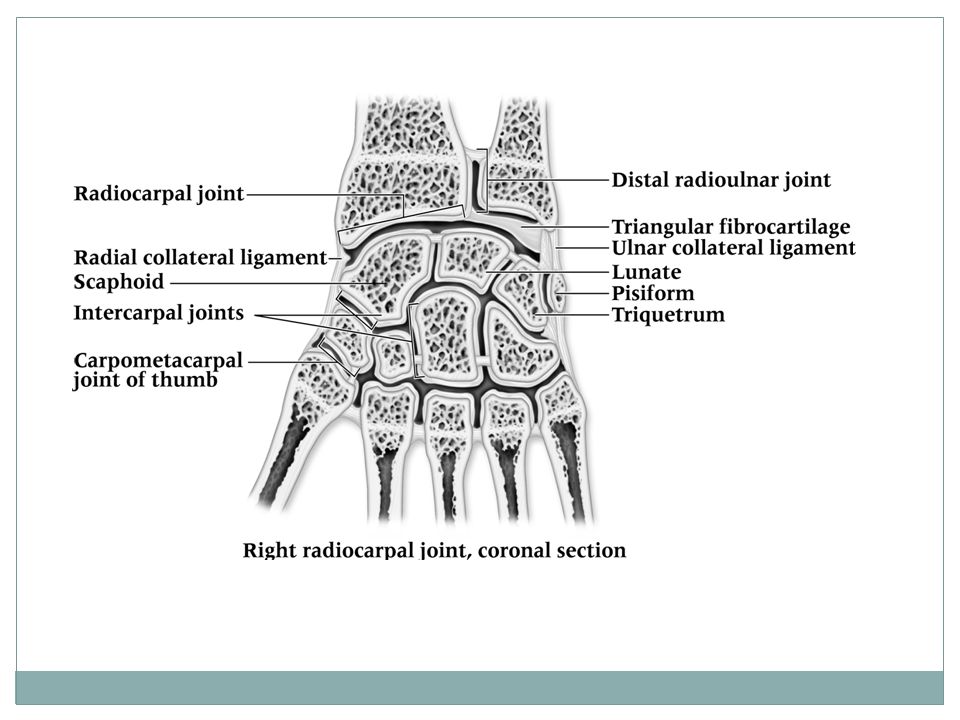
Wrist Joints/Ligaments
Radial Carpal Joint Radius and carpal bones Triangular Fibrocartilage Medial side Ulnar Collateral Ligament Radial Collateral Ligament Lateral side Intercarpal joints Between the wrist bones Carpal Metacarpal Joint of Thumb

6
Finger Ligaments Collateral Ligaments At each joint of the finger

8
Muscles Palmar Interossei (3) Palmar muscles Palmar muscles
Lumbricales Origin: tendon of flexor digitorum profundus Insertion: Tendons of the extensor digitorum communis Action flexes the metacarpophalangeal joints Extends the interphanlangeal joints Dorsal Interossei (4) Origin: Adjacent sides of all the metacarpals Insertion:Proximal phalanx of 2nd, 3rd and 4th fingers Abducts the fingers from the middle finger Palmar Interossei (3) Origin: medial side of the 2nd metacarpal and lateral side of the 4th and 5th metacarpals Insertion: Proximal phalanx of the same finger Action Adducts the fingers toward the middle finger
 Origin: Adjacent sides of all the metacarpals. Insertion:Proximal phalanx of 2nd, 3rd and 4th fingers. Abducts the fingers from the middle finger. Palmar Interossei (3) Origin: medial side of the 2nd metacarpal and lateral side of the 4th and 5th metacarpals. Insertion: Proximal phalanx of the same finger. Action. Adducts the fingers toward the middle finger.")
9
Muscles Flexor Pollicis Brevis Abductor Pollicis Brevis
Thenar muscles Thenar Muscles Flexor Pollicis Brevis Origin: trapezium and 1st metacarpal Insertion: base of the proximal phalanx of the thumb Action Flexes and adducts the thumb Adductor Pollicis Origin: capitate and 2-3rd metacarpals Insertion: proximal phalanx of thumb Adducts the thumb Abductor Pollicis Brevis Origin: scaphoid and trapezium Insertion: proximal phalanx of the thumb Action Abducts the thumb Opponens Pollicis Origin: trapezium Insertion: latearl border of the metacarpal of the thumb Pulls the thumb in front of the palm to meet the little finger

10
Muscles Palmaris Brevis Abductor digiti minimi
Hypothenar Muscles Hypothenar Muscles Palmaris Brevis Origin: Flexor retinaculum Insertion: Skin on the ulnar border of the hand Action Pulls the skin toward the middle of the palm Abductor digiti minimi Origin: pisiform Insertion: base of little finger Abducts the little finger Flexor digiti minimi brevis Origin: hamate Insertion: base of little finger Action Flexes little finger Opponens digiti minimi Insertion: metacarpal of little finger Brings the little finger out to meet the thumb

13
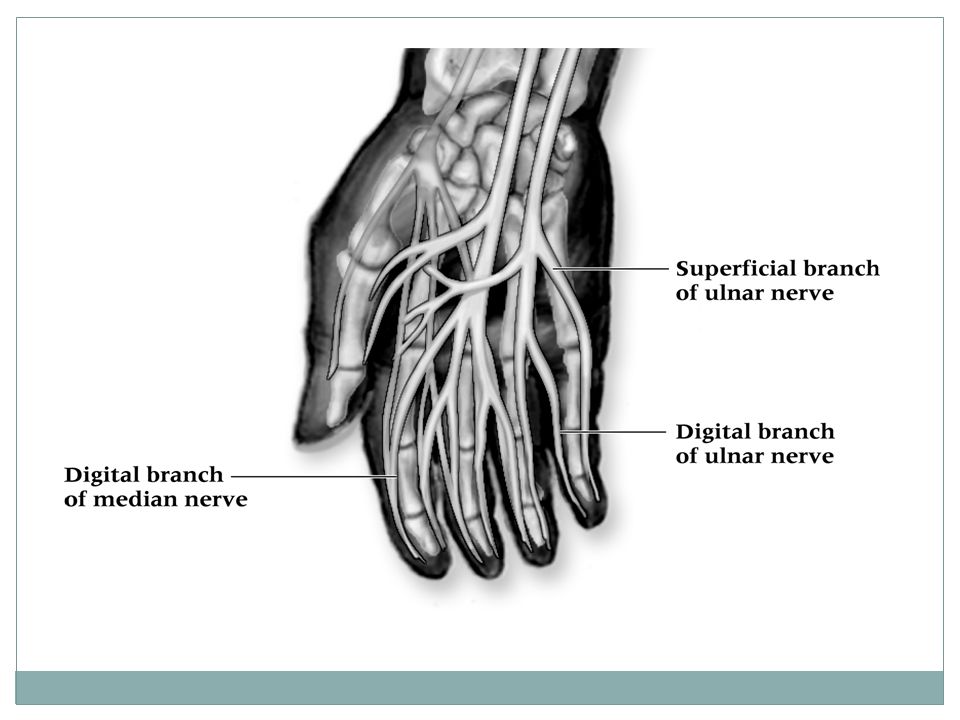
Blood and Nerve Supply Three major nerves
Ulnar, median and radial Ulnar and radial arteries supply the hand Two arterial arches (superficial and deep palmar arches)
")
15
Special Tests

16
Finklestin’s Test Test for de Quervain’s syndrome
Athlete makes a fist w/ thumb tucked inside Wrist is ulnarly deviated Positive sign is pain indicating stenosising tenosynovitis Pain over carpal tunnel could indicate carpal tunnel syndrome

17
Tinel’s Sign Produced by tapping over transverse carpal ligament
Tingling, paresthesia over sensory distribution of the median nerve indicates presence of carpal tunnel syndrome

18
Phalen’s Test Test for carpal tunnel syndrome
Position is held for approximately one minute If test is positive, pain will be produced in region of carpal tunnel

19
Valgus/Varus and Glide Stress Tests
Tests used to assess ligamentous integrity of joints in hands and fingers Valgus and varus tests are used to test collateral ligaments Anterior and posterior glides are used to assess the joint capsule

21
Circulatory and Neurological Evaluation
Hands should be felt for temperature Cold hands indicate decreased circulation Pinching fingernails can also help detect circulatory problems (capillary refill) Hand’s neurological functioning should also be tested (sensation and motor functioning) Allen’s test can also be used Patient is instructed to clench fist 3-4 times, holding it on the final time Pressure applied to ulnar and radial arteries Patient then opens hand (palm should be blanched) One artery is released and should fill immediately (both should be checked)
 Hand’s neurological functioning should also be tested (sensation and motor functioning) Allen’s test can also be used. Patient is instructed to clench fist 3-4 times, holding it on the final time. Pressure applied to ulnar and radial arteries. Patient then opens hand (palm should be blanched) One artery is released and should fill immediately (both should be checked)")
22
Functional Evaluation
Functional EvaluationRange of motion in all movements of wrist and fingers should be assessed Active, resistive and passive motions should be assessed and compared bilaterally Wrist - flexion, extension, radial and ulnar deviation MCP joint - flexion and extension PIP and DIP joints - flexion and extension Fingers - abduction and adduction MCP, PIP and DIP of thumb - flexion and extension Thumb - abduction, adduction and opposition 5th finger - opposition

23
Wrist/Hand/Finger Injuries

24
Wrist Sprains Wrist Sprains Management Etiology Signs and Symptoms
Most common wrist injury Arises from any abnormal, forced movement Falling on hyperextended wrist, violent flexion or torsion Multiple incidents may disrupt blood supply Signs and Symptoms Pain, swelling and difficulty w/ movement Management Refer to physician for X-ray if severe RICE, splint and analgesics Have patient begin strengthening soon after injury Tape for support can benefit healing and prevent further injury

25
Triangular Fibrocartilage Complex Injury (TFCC)
Etiology Occurs through forced hyperextension, falling on outstretched hand Violent twist or torque of the wrist Often associated w/ sprain of UCL Signs and Symptoms Pain along ulnar side of wrist, difficulty w/ wrist extension, possible clicking Swelling is possible, not much initially Patient may not report injury immediately

26
Triangular Fibrocartilage Complex Injury (TFCC)
Management Referred to physician for treatment Treatment will require immobilization initially for 4 weeks Immobilization should be followed by period of strengthening and ROM activities Surgical intervention may be required if conservative treatments fail

27
Tendinitis Etiology Management Signs and Symptoms
Repetitive pulling movements of (commonly) flexor carpi radialis and ulnaris; Repetitive pressure on palms (cycling) can cause irritation of flexor digitorum Primary cause is overuse of the wrist Signs and Symptoms Pain on active use or passive stretching Isometric resistance to involved tendon produces pain, weakness or both Management Acute pain and inflammation treated w/ ice massage 4x daily for first hours, NSAID’s and rest When swelling has subsided, ROM is promoted w/ contrast bath PRE can be instituted once swelling and pain subsided (high rep, low resistance)
 flexor carpi radialis and ulnaris; Repetitive pressure on palms (cycling) can cause irritation of flexor digitorum. Primary cause is overuse of the wrist. Signs and Symptoms. Pain on active use or passive stretching. Isometric resistance to involved tendon produces pain, weakness or both. Management. Acute pain and inflammation treated w/ ice massage 4x daily for first hours, NSAID’s and rest. When swelling has subsided, ROM is promoted w/ contrast bath. PRE can be instituted once swelling and pain subsided (high rep, low resistance)")
28
Nerve Compression, Entrapment, Palsy
Etiology Median and ulnar nerve compression Result of direct trauma to nerves Signs and Symptoms Sharp or burning pain associated w/ skin sensitivity or paresthesia Management Chronic entrapment may cause irreversible damage Surgical decompression may be necessary

29
Bishop/Benediction Hand: results from injury to the ulnar nerve
2. Claw Hand: results from compression of the median and ulnar nerves 3. Drop wrist: results from palsy of the radial nerve 4. Ape Hand: results from palsy of the median nerve

30
Carpal Tunnel Syndrome
Etiology Compression of median nerve due to inflammation of tendons and sheaths of carpal tunnel Result of repeated wrist flexion or direct trauma to anterior aspect of wrist Signs and Symptoms Sensory and motor deficits (tingling, numbness and paresthesia); weakness in thumb Management Conservative treatment - rest, immobilization, NSAID’s If symptoms persist, corticosteroid injection may be necessary or surgical decompression of transverse carpal ligament
; weakness in thumb. Management. Conservative treatment - rest, immobilization, NSAID’s. If symptoms persist, corticosteroid injection may be necessary or surgical decompression of transverse carpal ligament.")
31
De Quervian’s Disease (Hoffman’s disease)
Etiology Stenosing tenosynovitis in thumb (extensor pollicis brevis and abductor pollicis longus Constant wrist movement can be a source of irritation Signs and Symptoms Aching pain, which may radiate into hand or forearm Positive Finklestein’s test Point tenderness and weakness during thumb extension and abduction painful catching and snapping

32
De Quervain’s Disease Management Immobilization rest Cryotherapy
NSAID’s Ultrasound and ice are also beneficial Joint mobilizations have been recommended to maintain ROM

33
Scaphoid Fracture Etiology Management
Caused by force on outstretched hand, compressing scaphoid between radius and second row of carpal bones Often fails to heal due to poor blood supply Signs and Symptoms Swelling Severe pain in anatomical snuff box Presents like wrist sprain Pain w/ radial flexion Management Must be splinted and referred for X-ray prior to casting Immobilization lasts 6 weeks and is followed by strengthening and protective tape Wrist requires protection against impact loading for 3 additional months

34
Hamate Fracture Etiology Signs and Symptoms Management
Occurs as a result of a fall Signs and Symptoms Wrist pain Weakness Point tenderness Pull of muscular attachment can cause non-union Management Casting wrist and thumb is treatment of choice Hook of hamate can be protected w/ doughnut

35
Extensor Tendon Avulsion (Mallet Finger)
Etiology Caused by a blow to tip of finger avulsing extensor tendon from insertion Also referred to as baseball or basketball finger Signs and Symptoms Pain at DIP; X-ray shows avulsed bone on dorsal proximal distal phalanx Unable to extend distal end of finger (carrying at 30 degree angle) Point tenderness at sight of injury Management RICE and splinting for 6-8 weeks
 Point tenderness at sight of injury. Management. RICE and splinting for 6-8 weeks.")
36
Boutonniere Deformity
Etiology Rupture of extensor expansion dorsal to the middle phalanx Tendon slides below axis of PIP joint Forces DIP joint into extension and PIP into flexion Signs and Symptoms Severe pain obvious deformity inability to extend DIP joint Swelling, point tenderness Management Cold application, followed by splinting Splinting must be continued for 5-8 weeks Athlete is encouraged to flex distal phalanx

37
Jersey Finger (Flexor Digitorum Profundus Rupture)
Etiology Rupture of flexor digitorum profundus tendon Often occurs w/ ring finger when athlete tries to grab a jersey Signs and Symptoms DIP can not be flexed Finger remains extended Pain and point tenderness over distal phalanx Management Must be surgically repaired Rehab requires 12 weeks and there is often poor gliding of tendon, w/ possibility of re-rupture

38
Swan Neck Deformity (PsuedoBoutonniere) Etiology Signs and Symptoms
Distal tear of volar plate may cause Swan Neck deformity; Proximal tear may cause PsuedoBoutonniere deformity Signs and Symptoms Pain, swelling w/ varying degrees of hyperextension Tenderness over volar plate of PIP Indication of volar plate tear = passive hyperextension Management RICE and analgesics Splint in degrees of flexion for 3 weeks; followed by buddy taping and then PRE

39
Gamekeeper’s Thumb Etiology Signs and Symptoms
Sprain of UCL of MCP joint of the thumb Mechanism is forceful abduction of proximal phalanx Occasionally combined w/ hyperextension Signs and Symptoms Pain over UCL Weak and painful pinch

41
Gamekeeper’s Thumb Management Immediate follow-up must occur
If instability exists, athlete should be referred to orthopedist If stable, X-ray should be performed to rule out fracture Thumb splint should be applied for protection for 3 weeks or until pain free Splint should extend from wrist to end of thumb in neutral position Thumb spica should be used following splinting for support If a complete tear occurs, surgical repair is necessary to allow normal function to return

42
Sprains of IP Joints Etiology Signs and Symptoms Management
Can include collateral ligament, volar plate, extensor expansion tears Occurs w/ axial loading or valgus/varus stresses Signs and Symptoms Pain, swelling, point tenderness, instability Valgus and varus tests may be positive Management RICE, X-ray examination and possible splinting Splint at degrees of flexion for 10 days If sprain is to the DIP, splinting for a few days in full extension may assist healing process Taping can be used for support

43
Metacarpal Fracture Etiology S/S Management
Direct axial force, compressive force Being stepped on S/S Pain Swelling Appear to be an angular or rotational deformity Management Rice X-ray Reduce Splinting Splint 4-6 wks

44
Bennett’s Fracture Etiology S/S Management
1st metacarpal just distal to the CMC joint of the thumb Axial and abduction force to thumb S/S Pain Swelling over base of thumb Deformity Management Unstable and referred to orthopedic

45
Mallet Finger

46
Boutonniere Deformity

47
Jersey Finger

48
Swan Neck Deformity

49
Bennett’s Fracture

Similar presentations