Download presentation
Presentation is loading. Please wait.

1
Parvaneh Rabiee, Kate Baxter, Gillian Parker and Sylvia Bernard RNIB Research Day 2014: Rehabilitation and social care RNIB, 105 Judd Street, London 20 October 2014

2
Background and the rationale for the project Aims and methods The key findings Conclusions Implications for policy and practice

3
A rise in the number of people living longer with long-term conditions Sight loss is most prevalent among older people Increasing pressure on health and social care services Preventive and rehabilitation services are a high policy priority for all care settings Reduce the number of people entering the care system Reduce needs for on-going support

4
Growing interest in rehabilitation not a new idea: 1997: The Audit Commission 2000 onwards: Significant investment in intermediate care and reablement services 2010: DH guidance on eligibility criteria for adult social care - endorsed by: UK Vision Strategy Advisory Group 2013 Vision 2020 UK 2013 ADASS guidance 2013 2013: RNIB - ‘Facing Blindness Alone’ campaign 2014: Recent DH Care Act guidance

5
Much of the existing research has focused on low vision services – not clear What community-based rehab services are currently doing to support people with VI What impact they have on people with VI What a model of ‘good practice’ might look like The study funded by Thomas Pocklington Trust is the first step towards a future full evaluation study of vision rehabilitation services

6
To provide an overview of the evidence base for community-based vision rehab interventions: People aged 18 and over Rehab interventions funded by LAs in England The study involved 4 main research elements: A review of literature Scoping workshops with people with VI and key professionals A national survey Case studies

7
No secure evidence around effectiveness, costs and different models of community-based vision rehab services – however some strong messages for: The potential for vision rehab to have a positive impact on daily activities and depression High prevalence of depression in people with VI and increased need for emotional support Vision rehab interventions mostly target physical/functional rather than social and emotional issues The cost effectiveness of group-based self- management programmes

11
60% screened by professional with specialist vision rehab skills 95% assessed by professional with specialist vision rehab skills 25% required FACS assessments 66% reported a waiting list Average waiting time 8-10 weeks

13
Survey data on budgets poorly reported Annual budgets £13,000 to £800,000 Average budget £221,000 Annual caseloads 16 to 2000 Additional data from three case studies Annual budgets £238,000 to £336,000 Annual caseloads 282 to 3322

14
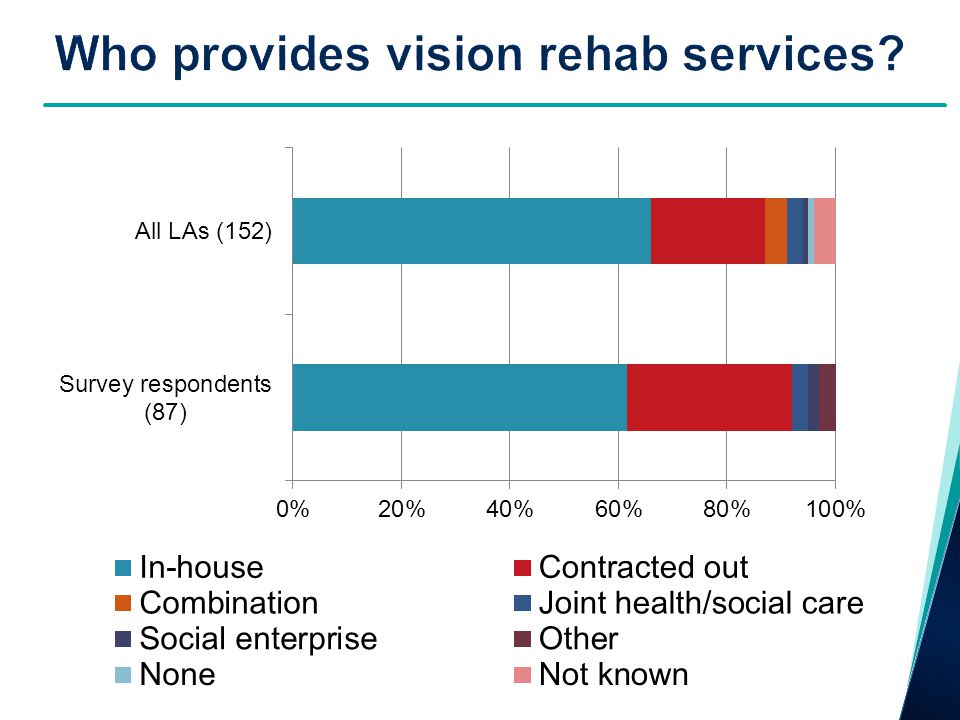
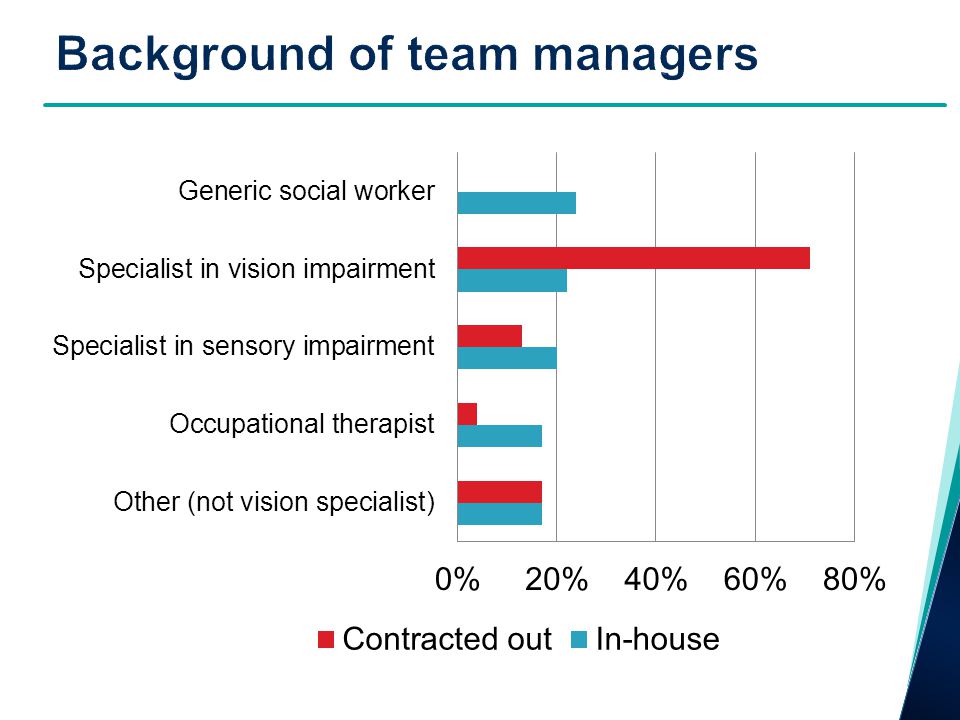
Who provides the service A and B: LA in-house C: Contracted out service Team delivering vision rehab A: Sensory Needs B and C: Visual Impairment Manager specialism A: Social Work B and C: Visual Impairment Current waiting time: A: up to 6 months B: up to 2 months C: up to 1 month

15
35-40% of time spent on admin duties – travelling time varied Differences in the way services operated Sites A & B restricted activities to one-to-one intervention - Site C offered a range of group-based activities Only one site (C) measured outcome using an evaluation tool Limited staff training & networking opportunities - more opportunities in site C
 measured outcome using an evaluation tool Limited staff training & networking opportunities - more opportunities in site C")
16
Access to specialist knowledge and skills Concerns about the loss of specialist input within the team Early access to vision rehab interventions Late referrals risk care needs intensifying and clients losing motivation A tendency among health professionals to see vision rehab as the last resort The characteristics of people who use vision rehab services

17
A long gap between diagnosis and referral - in particular those with degenerative conditions Rehab goals tailored around individual needs Support could continue as long as needed - But... Waiting list to get additional training - Site B Time constraints - Site C Progress monitored informally & no follow-up contacts

18
Boosted confidence, improved independence. Increased motivation People felt safer Greatest benefits related to mobility training, independent living skills and supply of aids, adaptation and equipment. Group-based activities offer great opportunities to socialise and learn from peers’ experiences Positive impacts on families

19
Information not always forthcoming and timely Concerns about future needs Help often offered when it is too late/when people ‘have to have it’ Emotional needs not met effectively Social activities most often geared towards older people

20
Staff with specialist knowledge and skills High quality assessment Personalised support Offering a wide range of support Flexibility to adapt to users’ abilities Timely intervention Shared vision among all relevant health and social care staff Regular follow-up visits Easy access to information

21
Potential for vision rehab to have a positive impact on the quality of life for people with VI A wide variation of vision rehab provision – measuring outcomes not a common practice Restricting access on the basis of FACS assessment Negative impacts of financial cuts Lack of recognition of specialist vision rehab skills Group-based activities effective but limited Main focus is on the physical aspects of life

22
All LAs should follow the recommended practice on FACS eligibility criteria – timely intervention Raising the profile of specialist vision rehabilitation skills Safeguarding specialist assessments Taking account of individual priorities Improved staff training and networking opportunities Greater focus on group-based activities

Similar presentations














 research project.>")






