Download presentation
Presentation is loading. Please wait.

1
The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure Internal Medicine/Pediatrics Noon conference series July 31, 2006

2
Accurate blood pressure measurement in the office Patient position Patient position Patient should be seated in a chair (not on an examination table) for 5 minutes Patient should be seated in a chair (not on an examination table) for 5 minutes Feet on floor Feet on floor Arm supported at heart level Arm supported at heart level Appropriate size cuff Appropriate size cuff Cuff bladder encircling at least 80% of the arm Cuff bladder encircling at least 80% of the arm
 for 5 minutes Patient should be seated in a chair (not on an examination table) for 5 minutes Feet on floor Feet on floor Arm supported at heart level Arm supported at heart level Appropriate size cuff Appropriate size cuff Cuff bladder encircling at least 80% of the arm Cuff bladder encircling at least 80% of the arm")
3
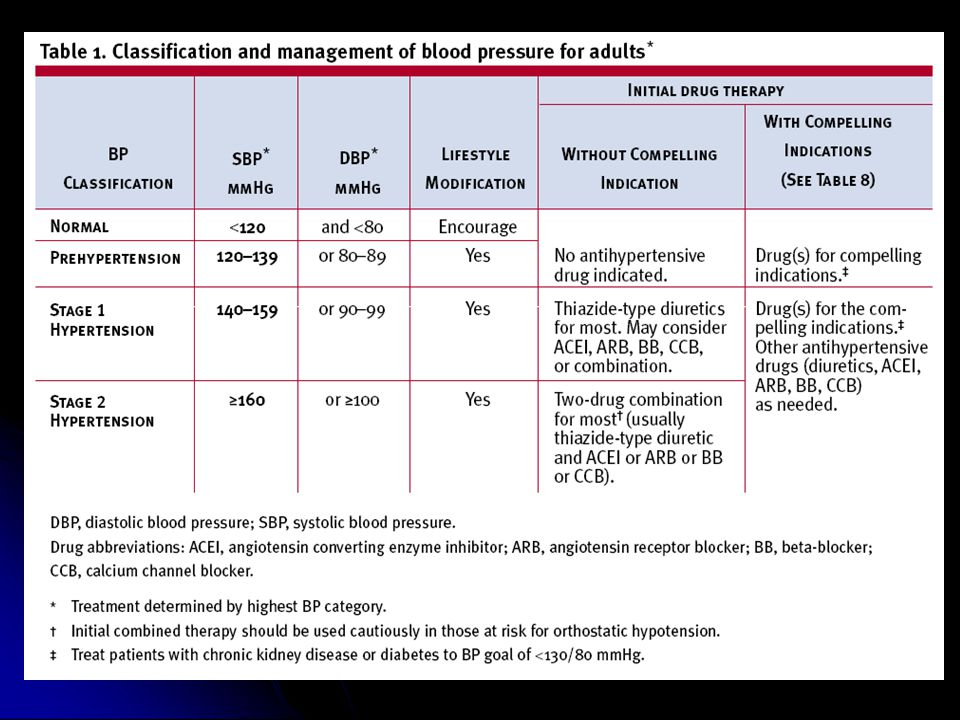
Classification of high blood pressure in adults Classification is based on 2 measurments made at 2 separate office visits Classification is based on 2 measurments made at 2 separate office visits Normal Normal Systolic 120 AND diastolic 80 Systolic 120 AND diastolic 80 Prehypertension Prehypertension Systolic 120-129 OR diastolic 80-89 Systolic 120-129 OR diastolic 80-89 Increased risk for progression to hypertension Increased risk for progression to hypertension Stage 1 hypertension Stage 1 hypertension Systolic 140-159 OR diastolic 90-99 Systolic 140-159 OR diastolic 90-99 Stage 2 hypertension Stage 2 hypertension Systolic 160 OR diastolic 100 Systolic 160 OR diastolic 100

5
Management of hypetension Reduction of cardiovascular and renal morbidity and mortality Reduction of cardiovascular and renal morbidity and mortality In patients with diabetes mellitus or renal disease, the target blood pressure is 130/80 In patients with diabetes mellitus or renal disease, the target blood pressure is 130/80 In patients without diabetes mellitus or renal disease, the target blood pressure is 140/90 In patients without diabetes mellitus or renal disease, the target blood pressure is 140/90 Primary focus should be directed toward achieving the systolic blood pressure goal Primary focus should be directed toward achieving the systolic blood pressure goal Most patients will achieve the diastolic pressure goal once the systolic pressure is at goal Most patients will achieve the diastolic pressure goal once the systolic pressure is at goal Goals of pharmacotherapy

6
Management of hypetension Dietary Approaches to Stop Hypertension (DASH) diet Dietary Approaches to Stop Hypertension (DASH) diet Dietary sodium reduction Dietary sodium reduction Independent of DASH diet Independent of DASH diet Physical activity Physical activity Moderation of alcohol consumption Moderation of alcohol consumption Lifestyle modifications
 diet Dietary Approaches to Stop Hypertension (DASH) diet Dietary sodium reduction Dietary sodium reduction Independent of DASH diet Independent of DASH diet Physical activity Physical activity Moderation of alcohol consumption Moderation of alcohol consumption Lifestyle modifications")
7
Management of hypetension For a 2100 kcal/day eating plan: For a 2100 kcal/day eating plan: Total fat: 27% of calories Saturated fat: 6% of calories Protein: 18% of calories Carbohydrate: 55% of calories Cholesterol: 150 mg Sodium: 2,300 mg Total fat: 27% of calories Saturated fat: 6% of calories Protein: 18% of calories Carbohydrate: 55% of calories Cholesterol: 150 mg Sodium: 2,300 mg Potassium: 4,700 mg Calcium: 1,250 mg Magnesium: 500 mg Fiber: 30 g Dietary Approaches to Stop Hypertension (DASH diet)
")
9
Management of hypertension Thiazide-type diuretics should be used as initial therapy for most patients Thiazide-type diuretics should be used as initial therapy for most patients Certain comorbidities are “compelling indciations” for the use of other drugs as initial monotherapy (see below) Certain comorbidities are “compelling indciations” for the use of other drugs as initial monotherapy (see below) Most patients will require drugs to achieve target blood pressure Most patients will require drugs to achieve target blood pressure If blood pressure is 20/10 mmHg above target, consider initiating therapy with 2 drugs (separately or in combination) If blood pressure is 20/10 mmHg above target, consider initiating therapy with 2 drugs (separately or in combination) Consider the risk of orthostatic hypotension in such patients who also have diabetes mellitus, autonomic neuropathy, etc Consider the risk of orthostatic hypotension in such patients who also have diabetes mellitus, autonomic neuropathy, etc Pharmacotherapy
 Certain comorbidities are compelling indciations for the use of other drugs as initial monotherapy (see below) Most patients will require drugs to achieve target blood pressure Most patients will require drugs to achieve target blood pressure If blood pressure is 20/10 mmHg above target, consider initiating therapy with 2 drugs (separately or in combination) If blood pressure is 20/10 mmHg above target, consider initiating therapy with 2 drugs (separately or in combination) Consider the risk of orthostatic hypotension in such patients who also have diabetes mellitus, autonomic neuropathy, etc Consider the risk of orthostatic hypotension in such patients who also have diabetes mellitus, autonomic neuropathy, etc Pharmacotherapy")
11
Management of hypertension Patients should return at approximately monthy intervals until target blood pressure is reached Patients should return at approximately monthy intervals until target blood pressure is reached After blood pressure is stable at target, monitoring can usually be done at 3-6 month intervals After blood pressure is stable at target, monitoring can usually be done at 3-6 month intervals Serum potassium and creatinine should be monitored at least 1-2 times per year Serum potassium and creatinine should be monitored at least 1-2 times per year Cormorbidities (diabetes mellitus, congestive heart failure, etc) may influence the monitoring schedule Cormorbidities (diabetes mellitus, congestive heart failure, etc) may influence the monitoring schedule Monitoring
 may influence the monitoring schedule Cormorbidities (diabetes mellitus, congestive heart failure, etc) may influence the monitoring schedule Monitoring")
12
Management of hypertension Target blood pressure 130/80 mmHg Target blood pressure 130/80 mmHg Combinations of 2 medications are usually necessary Combinations of 2 medications are usually necessary ACE and ARBS slow the progression of non-diabetic (as well as diabetic) kidney disease ACE and ARBS slow the progression of non-diabetic (as well as diabetic) kidney disease Limited creatine elevation ( 35% above baseline) is acceptable (unless hyperkalemia develops) Limited creatine elevation ( 35% above baseline) is acceptable (unless hyperkalemia develops) …with diabetes mellitus
 kidney disease ACE and ARBS slow the progression of non-diabetic (as well as diabetic) kidney disease Limited creatine elevation ( 35% above baseline) is acceptable (unless hyperkalemia develops) Limited creatine elevation ( 35% above baseline) is acceptable (unless hyperkalemia develops) …with diabetes mellitus")
13
Management of hypertension Target blood pressure 130/80 mmHg Target blood pressure 130/80 mmHg Combinations of 3 medications are usually necessary Combinations of 3 medications are usually necessary ACE and ARBS slow the progression of diabetic nephropathy ACE and ARBS slow the progression of diabetic nephropathy with chronic kidney disease

14
Management of hypertension Stable angina pectoris Stable angina pectoris Beta blockers are first-line therapy Beta blockers are first-line therapy Calcium-channel blockers are an alternative to beta blockers Calcium-channel blockers are an alternative to beta blockers Acute coronary syndrome (unstable angina or myocardial infarction) Acute coronary syndrome (unstable angina or myocardial infarction) Beta blocker Beta blocker ACE inhibitors ACE inhibitors Post-myocardial infarction Post-myocardial infarction Beta blocker Beta blocker ACE inhibitor ACE inhibitor Aldosterone antagonists Aldosterone antagonists (lipid management and aspirin therapy) (lipid management and aspirin therapy) with ischemic heart disease
 Acute coronary syndrome (unstable angina or myocardial infarction) Beta blocker Beta blocker ACE inhibitors ACE inhibitors Post-myocardial infarction Post-myocardial infarction Beta blocker Beta blocker ACE inhibitor ACE inhibitor Aldosterone antagonists Aldosterone antagonists (lipid management and aspirin therapy) (lipid management and aspirin therapy) with ischemic heart disease")
15
Management of hypertension Asymptomatic ventricular dysfunction Asymptomatic ventricular dysfunction ACE inhibitors ACE inhibitors Beta blockes Beta blockes Symptomatic ventricular dysfunction Symptomatic ventricular dysfunction ACE inhibitors and ARBs ACE inhibitors and ARBs Beta blockers Beta blockers Aldosterone blockers Aldosterone blockers (loop diurectics) (loop diurectics) …with congestive heart failure
 (loop diurectics) …with congestive heart failure")
16
Management of hypertension Have a reduced response to monotherapy with… Have a reduced response to monotherapy with… Beta blockers Beta blockers ACE inhibitors ACE inhibitors ARBS ARBS …compared with …compared with Diuretics Diuretics Calcium channel blockers Calcium channel blockers Combinations that include a diuretic largely eliminate these differences Combinations that include a diuretic largely eliminate these differences Incidence of angioedema 2-4 times greater than in other ethnic groups Incidence of angioedema 2-4 times greater than in other ethnic groups In African Americans

18
Key messages In persons older than 50 years, systolic blood pressure greater than 140 mmHg is a much more important cardiovascular disease (CVD) risk factor than diastolic blood pressure. The risk of CVD beginning at 115/75 mmHg doubles with each increment of 20/10 mmHg; individuals who are normotensive at age 55 have a 90 percent lifetime risk for developing hypertension. Individuals with a systolic blood pressure of 120–139 mmHg or a diastolic blood pressure of 80–89 mmHg should be considered as prehypertensive and require health-promoting lifestyle modifications to prevent CVD.

19
Key messages (continued) Thiazide-type diuretics should be used in drug treatment for most patients with uncomplicated hypertension, either alone or combined with drugs from other classes. Certain high-risk conditions are compelling indications for the initial use of other antihypertensive drug classes (angiotensin converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, calcium channel blockers). Most patients with hypertension will require two or more antihypertensive medications to achieve goal blood pressure (<140/90 mmHg, or <130/80 mmHg for patients with diabetes or chronic kidney disease). Certain high-risk conditions are compelling indications for the initial use of other antihypertensive drug classes (angiotensin converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, calcium channel blockers).
. Most patients with hypertension will require two or more antihypertensive medications to achieve goal blood pressure (<140/90 mmHg, or <130/80 mmHg for patients with diabetes or chronic kidney disease). Certain high-risk conditions are compelling indications for the initial use of other antihypertensive drug classes (angiotensin converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, calcium channel blockers)..")
20
Key messages (continued) Thiazide-type diuretics should be used in drug treatment for most patients with uncomplicated hypertension, either alone or combined with drugs from other classes. Certain high-risk conditions are compelling indications for the initial use of other antihypertensive drug classes (angiotensin converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, calcium channel blockers). Most patients with hypertension will require two or more antihypertensive medications to achieve goal blood pressure (<140/90 mmHg, or <130/80 mmHg for patients with diabetes or chronic kidney disease). If blood pressure is >20/10 mmHg above goal blood pressure, consideration should be given to initiating therapy with two agents, one of which usually should be a thiazide-type diuretic.
. Most patients with hypertension will require two or more antihypertensive medications to achieve goal blood pressure (<140/90 mmHg, or <130/80 mmHg for patients with diabetes or chronic kidney disease). If blood pressure is >20/10 mmHg above goal blood pressure, consideration should be given to initiating therapy with two agents, one of which usually should be a thiazide-type diuretic..")
21
Key messages The most effective therapy prescribed by the most careful clinician will control hypertension only if patients are motivated. Motivation improves when patients have positive experiences with, and trust in, the clinician. Empathy builds trust and is a potent motivator. In presenting these guidelines, the committee recognizes that the responsible physician’s judgment remains paramount.

22
Key messages The most effective therapy prescribed by the most careful clinician will control hypertension only if patients are motivated. Motivation improves when patients have positive experiences with, and trust in, the clinician. Empathy builds trust and is a potent motivator. In presenting these guidelines, the committee recognizes that the responsible physician’s judgment remains paramount.

23
Key messages The most effective therapy prescribed by the most careful clinician will control hypertension only if patients are motivated. Motivation improves when patients have positive experiences with, and trust in, the clinician. Empathy builds trust and is a potent motivator. In presenting these guidelines, the committee recognizes that the responsible physician’s judgment remains paramount.

24
Question Category Systolic pressure Diastolic pressure Normal Prehypertension Stage 1 hypertension Stage 2 hypertension

25
Question Indication ( assume no comorbidity) Recommended initial therapy Prehypertension Hypertension Stage 1 hypertension Stage 2 hypertension
 Recommended initial therapy Prehypertension Hypertension Stage 1 hypertension Stage 2 hypertension")
26
Question Comorbidity Recommended initial therapy Diabetes mellitus Hypertension Ischemic heart disease Congestive heart failure

Similar presentations





















 Blood Pressure Linda Macdonald, M.D. October 9, 2007 Coronado Thunderbirds.>")
