Download presentation
Presentation is loading. Please wait.

1
Chest Trauma, Chest Tubes & Underwater Seal Drainage
By: Victoria Murray & Mary Beth Chauder

2
Objectives To review the anatomy and physiology of the respiratory system. To identify the various types of trauma associated with the chest, and the nursing management associated with them To discuss the mechanics of chest tubes, their uses, and the nursing management associated with them To discuss pain management, nursing interventions and nursing diagnosis associated with chest trauma To evaluate the understanding of the class with the use of a case study.

3
The Respiratory System
Quick Overview Composed of the Upper and Lower Respiratory Tract: Together, they are responsible for ventilation, or the movement of air in and out of the airways Upper respiratory tract consists of the nose, sinuses and nasal passages, pharynx, tonsils and adenoids, larynx, and trachea and is largely responsible for warming and filtering the air The lower respiratory tract, comprised of the lungs, bronchi, bronchioles and alveoli and is responsible for gas exchange 1) Lungs are paired elastic structures enclosed in the thoracic cage, which is an airtight chamber with distensible walls. - Each lung is divided into lobes. The left lung has an upper and lower lobe, and the right lung has an upper, middle and lower lobe. Each lobe is further divided into fissures 2) Bronchi and Bronchioles – Lobar bronchi (3 in right, and 2 in left) which divide into segmental bronchi which are the structures identified when choosing the most effective postural drainage position. Bronchi further divide to bronchioles, which then divide into terminal bronchioles. 3) Alveoli – The lungs are made up of about 300 million alveoli, which are arranged in clusters of about There are 2 types of alveoli i) epithelial that form the alveolar walls ii) alveoli that are metabolically active and secrete surfactant, which prevents alveolar collapse and iii) alveolar macrophages that ingest foreign matter. 4) Pleura - The lungs are covered with a membrane called the visceral pleura. The interior chest wall is lined with a membrane called the parietal pleura. The space in between, the pleural space, is filled with approximately 4 ml of lubricating fluid to help the pleura slide during respiration. A negative intrapleural pressure is needed to expand the lung 5) Mediastinum – is in the middle of the thorax between the pleura sacs that contain the two lungs. It contains all the thoracic tissue outside of the lungs The chest cavity is a closed structure bound by muscle, bone, connective tissue, vascular structures and the diaphragm. This cavity has three distinct sections, each sealed from the others: 1 & 2 = Each lung, 3 section is the mediastinum. Trauma, disease, or surgery can result in air, blood, or fluid leaking into the intrapleural space creating a positive pressure that collapses lung tissue. Small leaks are sometimes absorbed, however large leaks require chest tubes to remove the air or fluid from the pleural space (Day et al., 2010)
 Lungs are paired elastic structures enclosed in the thoracic cage, which is an airtight chamber with distensible walls. - Each lung is divided into lobes. The left lung has an upper and lower lobe, and the right lung has an upper, middle and lower lobe. Each lobe is further divided into fissures. 2) Bronchi and Bronchioles – Lobar bronchi (3 in right, and 2 in left) which divide into segmental bronchi which are the structures identified when choosing the most effective postural drainage position. Bronchi further divide to bronchioles, which then divide into terminal bronchioles. 3) Alveoli – The lungs are made up of about 300 million alveoli, which are arranged in clusters of about There are 2 types of alveoli i) epithelial that form the alveolar walls ii) alveoli that are metabolically active and secrete surfactant, which prevents alveolar collapse and iii) alveolar macrophages that ingest foreign matter. 4) Pleura - The lungs are covered with a membrane called the visceral pleura. The interior chest wall is lined with a membrane called the parietal pleura. The space in between, the pleural space, is filled with approximately 4 ml of lubricating fluid to help the pleura slide during respiration. A negative intrapleural pressure is needed to expand the lung. 5) Mediastinum – is in the middle of the thorax between the pleura sacs that contain the two lungs. It contains all the thoracic tissue outside of the lungs. The chest cavity is a closed structure bound by muscle, bone, connective tissue, vascular structures and the diaphragm. This cavity has three distinct sections, each sealed from the others: 1 & 2 = Each lung, 3 section is the mediastinum. Trauma, disease, or surgery can result in air, blood, or fluid leaking into the intrapleural space creating a positive pressure that collapses lung tissue. Small leaks are sometimes absorbed, however large leaks require chest tubes to remove the air or fluid from the pleural space. (Day et al., 2010)")
4
Ventilation Mechanisms
Ventilation is the movement of air in and out of the airways to continually replenish O2 and remove CO2. It depends on a system of open airways and the movement of respiratory muscles, primarily the diaphragm which is innervated by the phrenic nerve. Air flows from an area of high pressure to low pressure. During inspiration movement of the diaphragm and other muscles of respiration enlarges the thoracic cavity creating a low pressure, therefore air flows in. During expiration, the diaphragm relaxes and the lungs recoil, resulting in decreased thoracic cavity and increased pressure, therefore air flows out. Ventilation is controlled by a complex network of chemoreceptors that sends messages to the brain, which in turn activates the diaphragm by means of the phrenic nerve. (Day et al., 2010)
")
5
Blunt or Penetrating Trauma
What is Chest Trauma? ME Chest trauma can be classified as either blunt or penetrating. Blunt chest trauma results from sudden compression or positive pressure inflicted to the chest wall. Penetrating chest trauma occurs when a foreign object penetrates the chest wall (Day et al., 2010). Classified as either: Blunt or Penetrating Trauma
. Classified as either: Blunt or Penetrating Trauma.")
6
Blunt Trauma Most Common Causes: Generalized Symptoms:
MVA (Seatbelt, wheel) Falls Bicycle Crashes Generalized Symptoms: Hypoxemia Hypovolemia Cardiac Failure ME Blunt thoracic injuries are responsible for approximately 8% of all trauma admissions. Although blunt chest trauma is more common than penetrating trauma, it is often difficult to identify the extent of the damage because the symptoms may be generalized and vague. In addition, patients may not seek immediate medical attention, which may complicate the problem. The most common causes of blunt chest trauma are: Motor vehicle accidents – trauma from steering wheel or seat belt Falls Bicycle crashes – trauma from handlebars Mechanisms of blunt chest trauma: Acceleration – moving object hitting the chest or patient being thrown into an object Deceleration – sudden decrease in rate of speed or velocity, such as an MVA Shearing – stretching forces to areas of the chest causing tears, ruptures, or dissections Compression – direct blow to the chest, such as a crush injury Signs and Symptoms Hypoxemia – from disruption of the airway; injury to the lung parenchyma, rib cage, and respiratory musculature; massive hemorrhage; collapsed lung; and pneumothorax. Hypovolemia – from massive fluid loss from the great vessels, cardiac rupture, or hemothorax. Cardiac failure – from cardiac tamponade, cardiac contusion, or increased intrathoracic pressure. These pathologic states frequently result in impaired ventilation and perfusion leading to acute respiratory failure, hypovolemic shock, and death. Mechanisms of Blunt Chest Trauma: Acceleration – moving object impacts chest Deceleration – sudden decrease in speed/velocity (MVA) Shearing – stretching forces to areas of chest Compression – direct blow to the chest
 Falls. Bicycle Crashes. Generalized Symptoms: Hypoxemia. Hypovolemia. Cardiac Failure. ME. Blunt thoracic injuries are responsible for approximately 8% of all trauma admissions. Although blunt chest trauma is more common than penetrating trauma, it is often difficult to identify the extent of the damage because the symptoms may be generalized and vague. In addition, patients may not seek immediate medical attention, which may complicate the problem. The most common causes of blunt chest trauma are: Motor vehicle accidents – trauma from steering wheel or seat belt. Falls. Bicycle crashes – trauma from handlebars. Mechanisms of blunt chest trauma: Acceleration – moving object hitting the chest or patient being thrown into an object. Deceleration – sudden decrease in rate of speed or velocity, such as an MVA. Shearing – stretching forces to areas of the chest causing tears, ruptures, or dissections. Compression – direct blow to the chest, such as a crush injury. Signs and Symptoms. Hypoxemia – from disruption of the airway; injury to the lung parenchyma, rib cage, and respiratory musculature; massive hemorrhage; collapsed lung; and pneumothorax. Hypovolemia – from massive fluid loss from the great vessels, cardiac rupture, or hemothorax. Cardiac failure – from cardiac tamponade, cardiac contusion, or increased intrathoracic pressure. These pathologic states frequently result in impaired ventilation and perfusion leading to acute respiratory failure, hypovolemic shock, and death. Mechanisms of Blunt Chest Trauma: Acceleration – moving object impacts chest. Deceleration – sudden decrease in speed/velocity (MVA) Shearing – stretching forces to areas of chest. Compression – direct blow to the chest.")
7
Penetrating Trauma Most Common Causes: Gunshot Stab Wound
Classified By: Velocity: Stab Wound Low Gunshot High ME Stab and gunshot wounds are the most common types of penetrating chest trauma. They are classified according to their velocity. Stab wounds are generally considered of low velocity because the weapon destroys a small area around the wound. The most common weapons causing stab wounds are knives and switchblades. The external appearance of a stab wound may be deceptive because pneumothorax, hemothorax, lung contusion, and cardiac tamponade, along with severe and continuing hemorrhage can occur from just a small wound. Gunshot wounds to the chest may be classified as of low, medium, or high velocity. The factors that determine the velocity and resulting extent of damage include the distance from which the gun was fired, the calibre of the gun, and the size of the bullet. A bullet can cause damage at the site of penetration and along it’s pathway. It may also ricochet off bony structures and damage the chest organs and great vessels. If the diaphragm is involved in either a gunshot wound or a stab wound, injury to the chest cavity must be considered.

8
Initial Assessment of Suspected Chest Trauma
VITALS & LOC Temperature, Pulse, RR, BP, SPO2 & PAIN Inspect Respirations Effort & Depth; Chest Wall Symmetry. Paradoxical Chest Wall Motion; Bruising ; Penetrating Wounds Palpate Trachea for deviation; Adequate and Equal Chest Wall Movement; Chest wall tenderness; Rib 'crunching' indicating rib fractures Percuss Percuss Both Sides of the Chest Looking for Dullness or Resonance Auscultate Normal & Equal Breath Sounds The primary goal of the initial assessment is identify and treat immediately life-threatening conditions Life-threatening chest injuries include: Tension pneumothorax, massive hemothorax, open pneumothorax, cardiac tamponade and flail chest. Physical examination is the primary tool for diagnosis of acute thoracic trauma Vitals Inspect: Respiration Rate, Effort & Depth; Chest Wall Symmetry. Paradoxical Chest Wall Motion – indicating flail chest; Bruising (seat belt or steering wheel marks) lacerations; Penetrating Wounds Palpate Trachea for deviation; Adequate and Equal Chest Wall Movement; Chest wall tenderness; Rib 'crunching' indicating rib fractures Percuss Percuss Both Sides of the Chest Looking for Dullness or Resonance Auscultate Normal & Equal Breath Sounds – Any cracking or decreased entry? Also helpful ABGs, Diagnostic imaging (x-ray, CT etc…) (Brown et al., 2009)
 lacerations; Penetrating Wounds. Palpate. Trachea for deviation; Adequate and Equal Chest Wall Movement; Chest wall tenderness; Rib crunching indicating rib fractures. Percuss. Percuss Both Sides of the Chest Looking for Dullness or Resonance. Auscultate. Normal & Equal Breath Sounds – Any cracking or decreased entry Also helpful ABGs, Diagnostic imaging (x-ray, CT etc…) (Brown et al., 2009)")
9
Initial Assessment of Suspected Chest Trauma
Trachea Chest Expansion Breath Sounds Percussion Tension Pneumothorax Away from Affected side Decreased (Hyperexpansion) Diminished Hyper-resonate Simple Pneumothorax Midline Decreased May be Diminished May be Hyper-resonate Hemothorax Diminished (lg) or Normal (sm) Dull Pulmonary Contusion Normal Normal , Crackles Lung Collapse Towards Affected Side (Trauma. Org, 2004)
 Diminished. Hyper-resonate. Simple Pneumothorax. Midline. Decreased. May be Diminished. May be Hyper-resonate. Hemothorax. Diminished (lg) or Normal (sm) Dull. Pulmonary Contusion. Normal. Normal , Crackles. Lung Collapse. Towards Affected Side. (Trauma. Org, 2004)")
10
Secondary Assessment of Chest Trauma
Gather history of event from family, client, and EHS. Chief complaint In depth medical history Allergies Pain assessment

11
Complications Of Chest Trauma
Pneumothoraxes Simple Traumatic Open Hemothorax Tension Pneumothorax Pleural Effusion Sternal and Rib Fractures Flail Chest Pulmonary Contusion Cardiac Tamponade Pulmonary Embolism * A pneumothorax occurs when the parietal or visceral pleura is breached and the pleural space is exposed to positive atmospheric pressure. Normally , the pressure in the pleural space is negative compared with atmospheric pressure; this negative pressure is required to maintain lung inflation. When either pleura is breached, air enters the pleural space, and the lungs or a portion of it collapses.

12
Pneumothorax defined & types individually discuss
Three Types: Simple Traumatic Open Hemothorax Tension Simple pneumothorax A simple or spontaneous pneumothorax occurs when air enters the pleural space through a breach of either the parietal or visceral pleura. Most commonly, this occurs as air enters the pleural space through the rupture of a bleb or a bronchopleural fistula. A spontaneous pneumothorax may occur in an apparently healthy person in the absence of trauma due to a rupture of an air-filled bleb, or blister, on the surface of the lung, allowing air from the airways to enter the pleural cavity. It may be associated with diffuse interstital lung disease and severe emphysema. Traumatic Pneumothorax Traumatic pneumothorax occurs when air escapes from the lung through a laceration and air enters the pleural space; or air enters the pleural space through a wound in the chest wall. It can occur from both blunt (rib fracture) and penetrating chest trauma. It may also occur from abdominal trauma or from diaphragmatic tears. Traumatic pneumothorax may also occur from invasive thoracic procedures (thoracentesis, transbronchial lung biopsy, insertion of a subclavian line) in which the pleura is inadvertently punctured or with barotrauma from mechanical ventilation. Open pneumothorax A form of traumatic pneumothorax. Occurs when a wound in the chest wall is large enough to allow air to pass freely in and out of the thoracic cavity with each respiration. Because the rush of air through the hole in the chest wall produces a sucking sound, such injuries are termed sucking chest wounds. In such patients, not only does the lung collapse, but the structures of the mediastinum (heard and great vessels) also shift toward the uninjured side with each inspiration and in the opposite direction with expiration. This is termed mediastinal flutter or mediastinal swing, and it produces serious circulatory problems. (Day et al., 2010)
 and penetrating chest trauma. It may also occur from abdominal trauma or from diaphragmatic tears. Traumatic pneumothorax may also occur from invasive thoracic procedures (thoracentesis, transbronchial lung biopsy, insertion of a subclavian line) in which the pleura is inadvertently punctured or with barotrauma from mechanical ventilation. Open pneumothorax. A form of traumatic pneumothorax. Occurs when a wound in the chest wall is large enough to allow air to pass freely in and out of the thoracic cavity with each respiration. Because the rush of air through the hole in the chest wall produces a sucking sound, such injuries are termed sucking chest wounds. In such patients, not only does the lung collapse, but the structures of the mediastinum (heard and great vessels) also shift toward the uninjured side with each inspiration and in the opposite direction with expiration. This is termed mediastinal flutter or mediastinal swing, and it produces serious circulatory problems. (Day et al., 2010)")
13
Tension Pneumothorax Air is drawn into the pleural space from a laceration. Air that enters becomes trapped Increased positive pressure Lung collapses and causes a mediastinal shift away from the affected lung Tension Pneumothorax A tension pneumothorax occurs when air is drawn into the pleural space from a lacerated lung or through a small hole in the chest wall. It my be a complication of other types of pneumothorax. In contrast to open pneumothorax, the air that enters the chest cavity with each inspiration is trapped; it cannot be expelled during expiration through the air passages or the hole in the chest wall. With each breath tension is increased within the affected pleural space. This causes the lung to collapse and the heart, the great vessels, and the trachea to shift toward the unaffected side of the chest; mediastinal shift. Both respiration and circulatory function are compromised because of the increased intrathoracic pressure. The increased intrathoracic pressure decreases venous return to the heart, causing decreased cardiac output and impairment of peripheral circulation. In extreme cases, the pulse may be undetectable – this is known as pulseless electrical activity. (Day et al., 2010) (Day et al., 2010)
 (Day et al., 2010)")
14
Hemothorax 40% of the circulating blood volume can accumulate
A small amount of blood (<300) in the pleural space may cause no clinical manifestations and may require no intervention (blood is reabsorbed spontaneously). Massive HTX results from a rapid accumulation of more than 1500cc of blood in the chest cavity. This may be life threatening because of resultant hypovolemia and tension Rib fractures and pulmonary parenchyma disruption are the most common causes Hemothorax is known as bleeding into the pleural space and is common of thoracic trauma. (Day et al., 2010)
 in the pleural space may cause no clinical manifestations and may require no intervention (blood is reabsorbed spontaneously). Massive HTX results from a rapid accumulation of more than 1500cc of blood in the chest cavity. This may be life threatening because of resultant hypovolemia and tension. Rib fractures and pulmonary parenchyma disruption are the most common causes. Hemothorax is known as bleeding into the pleural space and is common of thoracic trauma. (Day et al., 2010)")
15
Pneumothorax-Manifestations
Simple/Uncomplicated Sudden onset of pain ↓ Tactile Fremitis Absent breath sounds Hyperresonant Percussion Minimal respiratory distress Large/Tension Air hungry, anxious, dyspnea, diaphoresis, hypotension, tachycardia Central cyanosis may re from severe hypoxemia Acute Respiratory Distress—lung collapses totally The signs and symptoms associated with pneumothorax depend on its size and cause. Pain is usually sudden and may be pleuritic. The patient may have only minimal respiratory distress with slight chest discomfort and tachypnea with a small simple or uncomplicated pneumothorax. If the pneumothorax is large and the lung collapses totally, acute respiratory distress occurs. The patient is anxious, has dyspnea and air hunger, has increased use of accessory muscles, and may develop central cyanosis from severe hypoxemia. For any type of pneumothorax, the nurse assesses for tracheal alignment, expansion of the chest, breath sounds, and the percussion of the chest. In a simple pneumothorax, the trachea is midline, expansion of the chest is decreased, breath sounds may be diminished, and percussion of the chest may reveal normal sounds or hyperressonance, depending on the size of the pneumothorax. In a tension pneumothorax, the trachea is shifted away from the affected side, chest expansion may be decreased or fixed in a hyperexpansion state, breath sounds are diminished or absent, and percussion to the affected side is hyperresonant. The clinical picture is one of air hunger, agitation, increasing hypoxemia, central cyanosis, hypotension, tachycardia, and profuse diaphoresis.

16
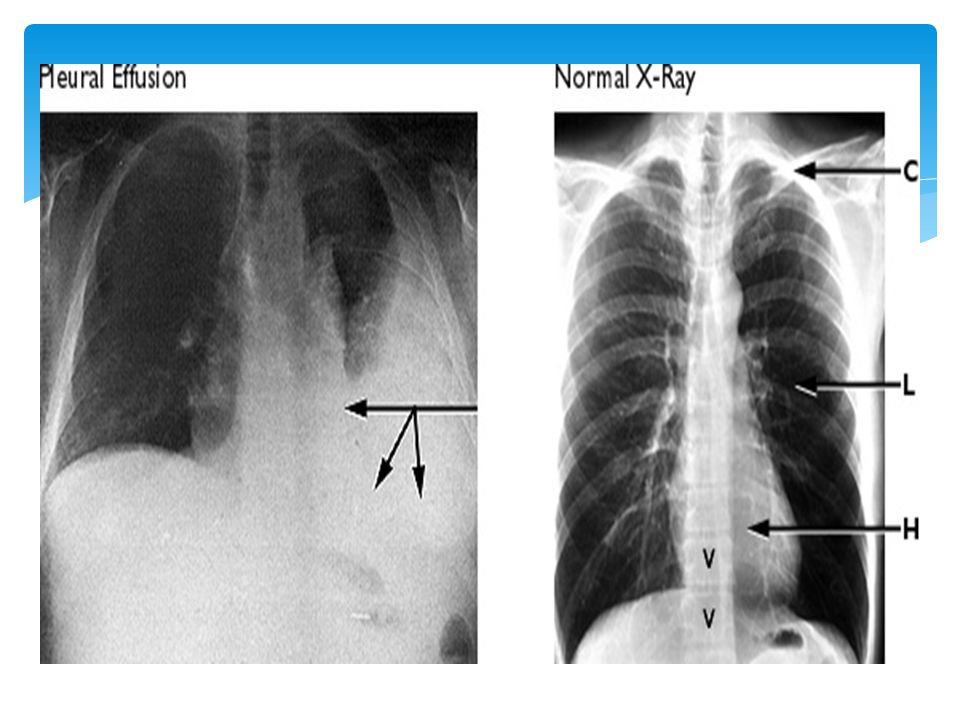
Pleural Effusion Pleural = Pleural Cavity
Effusion = abnormal, excessive collection of this fluid

17
Pleural Effusion Abnormal buildup of fluid between linings of the lung and chest wall result of a disease process or inflammation Normally 5 to 10 mL of serous fluid in the visceral and parietal pleura. Any more can cause great changes in intrathoracic pressure. Normally only small amount of fluid in the pleural space. Pleural fluid lubricates and allows visceral pleura to slide over parietal pleura. Pleural effusion often associated with Three T’s – trauma, tumor, TB. Can also be caused by heart failure, cirrhosis, pneumonia, pancreatitis.

18
Signs and Symptoms Pleural effusion in itself does not cause symptoms.
If effusion expands and presses on lung, patient may develop sharp, localized pain that worsens with coughing, or deep breathing. Dyspnea non-productive cough. The most common symptoms, regardless of the type of fluid in the pleural space or its cause, are shortness of breath and chest pain. However, many people with pleural effusion have no symptoms at all.

19
Signs and Symptoms cont...
Early signs include decreased or bronchial breath sounds on the affected side, dullness to percussion, and decreased fremitus over area of fluid accumulation Auscultation: EGOPHONY Hear “A” over fluid accumulation when patient speaks “E”.

20
Complications of Pleural Effusion
Respiratory compromise and distress from fluid compressing lung. Infection in pleural space---Sepsis/Empyema Fistulas in bronchi or chest wall Inflammation/infection in pleural space leads to increased potential for adhesions. Adhesions isolate effusion to one lung and complicates treatment.

22
Sternal & Rib Fractures
Rib Fractures are the most common type of Chest Trauma (60%) Sternal Fractures are most common in MVCs Sternal fractures are most common in motor vehicle crashes with a direct blow to the sternum via the steering wheel (Day et al., 2010). Rib #s are the most common type of chest trauma occurring in more than 60% of patient’s admitted with blunt chest trauma (Day et al., 2010) Fractures of the 1st 3 ribs are rare but are associated with high mortality rates because of the risk of laceration to the subclavian artery or vein (Day et al., 2010) Fractures involving the 5th-9th rib are the most common sites of fractures (Day et al., 2010) Fractures of the lower ribs can result in injuries to the spleen and liver, which may be lacerated by fragmented sections of the rib (Day et al., 2010) Fractures to the 5th-9th Rib are most common site of fracture (Day et al., 2010)
 Sternal Fractures are most common in MVCs. Sternal fractures are most common in motor vehicle crashes with a direct blow to the sternum via the steering wheel (Day et al., 2010). Rib #s are the most common type of chest trauma occurring in more than 60% of patient’s admitted with blunt chest trauma (Day et al., 2010) Fractures of the 1st 3 ribs are rare but are associated with high mortality rates because of the risk of laceration to the subclavian artery or vein (Day et al., 2010) Fractures involving the 5th-9th rib are the most common sites of fractures (Day et al., 2010) Fractures of the lower ribs can result in injuries to the spleen and liver, which may be lacerated by fragmented sections of the rib (Day et al., 2010) Fractures to the 5th-9th Rib are most common site of fracture. (Day et al., 2010)")
23
Sternal & Rib Fractures
Interventions: Pain Control Deep Breathing and Coughing Surgery is Rarely Necessary Manifestations Chest Pain Ecchymosis Crepitus Swelling Chest Wall Deformities The patient with sternal fractures has anterior chest pain, overlying tenderness, ecchymosis, crepitus, swelling and possible chest wall deformities (Day et al., 2010) For the patient with rib fractures, clinical manifestations are similar – severe pain, point tenderness, and muscle spasm over the area of the fracture that is aggravated by coughing, deep breathing and movement. The area around the fracture site may be bruised (Day et al., 2010). To reduce pain, the patient splints the chest by breathing in a shallow manner and avoids deep breathing, coughing or movement. This becomes problematic and can lead to atelectasis (Day et al., 2010) Assessment– Patient must be closely evaluated for underlying cardiac injuries - A crackling or grating sound in the thorax may be heard on auscultation. Diagnostic – Chest x-ray, ECG, pulse oximetry and ABG analysis Medical management – Important to control pain to allow for deep breathing and coughing to prevent atelectasis. However, care must be taken to avoid over sedation which decreases respiration. (Day et al., 2010) Surgery is rarely necessary unless fracture is grossly displaced and there is an increased risk of further injury (Day et al., 2010) Pain subsides in 5-7 days and rib fractures heal in 3-6 weeks (Day et al., 2010) Patient Must Be Closely Monitored for Underlying Cardiac Injuries!!
 For the patient with rib fractures, clinical manifestations are similar – severe pain, point tenderness, and muscle spasm over the area of the fracture that is aggravated by coughing, deep breathing and movement. The area around the fracture site may be bruised (Day et al., 2010). To reduce pain, the patient splints the chest by breathing in a shallow manner and avoids deep breathing, coughing or movement. This becomes problematic and can lead to atelectasis (Day et al., 2010) Assessment– Patient must be closely evaluated for underlying cardiac injuries - A crackling or grating sound in the thorax may be heard on auscultation. Diagnostic – Chest x-ray, ECG, pulse oximetry and ABG analysis. Medical management – Important to control pain to allow for deep breathing and coughing to prevent atelectasis. However, care must be taken to avoid over sedation which decreases respiration. (Day et al., 2010) Surgery is rarely necessary unless fracture is grossly displaced and there is an increased risk of further injury (Day et al., 2010) Pain subsides in 5-7 days and rib fractures heal in 3-6 weeks (Day et al., 2010) Patient Must Be Closely Monitored for Underlying Cardiac Injuries!!")
24
Flail Chest Caused by Blunt trauma
Flail Chest: A person with multiple rib fractures can develop a flail chest, a condition in which fractures cause instability in part of the chest wall (Potter & Perry, 2009). Flail chest is a frequency complication of blunt trauma from a steering wheel injury. It usually occurs when three or more adjacent ribs are fractured at two or more sites, resulting in free floating rib segments. As a result, the chest wall loses stability, and there is subsequent respiratory impairment - usually severe (Day et al., 2010) During inspiration, as the chest expands, the detached part of the rib segment (Flail segment) moves in a paradoxical manner – it is pulled inwards during inspiration, mediastinal structures shift to the unaffected side, reducing the amount of air that can be drawn into the lungs On expiration, because the intrathoracic pressure exceeds atmospheric pressure, the flail segment buldges outward, mediastinal structures shift back to the affected side- impairing the patient’s ability to exhale (Day et al., 2010)
. Flail chest is a frequency complication of blunt trauma from a steering wheel injury. It usually occurs when three or more adjacent ribs are fractured at two or more sites, resulting in free floating rib segments. As a result, the chest wall loses stability, and there is subsequent respiratory impairment - usually severe (Day et al., 2010) During inspiration, as the chest expands, the detached part of the rib segment (Flail segment) moves in a paradoxical manner – it is pulled inwards during inspiration, mediastinal structures shift to the unaffected side, reducing the amount of air that can be drawn into the lungs. On expiration, because the intrathoracic pressure exceeds atmospheric pressure, the flail segment buldges outward, mediastinal structures shift back to the affected side- impairing the patient’s ability to exhale (Day et al., 2010) v=uJHfX1RFkF0.")
25
Flail chest trauma As with rib fracture, treatment of flail chest is usually supportive. Management includes providing ventilatory support, clearing secreting from lungs and controlling pain Treatment varies depending on severity respiratory dysfunction Small segment is involved, the objective is to clear the airway through position, deep breathing, coughing and suctioning to aid in the expansion of the lung and to relieve pain by intercostal nerve blocks, high thoracic epidural blocks or cautious use of IV opiods For severe flail chest injury, endotracheal intubation and mechanical ventilation is required to provide internal pneumatic stabilization of the flail chest and to correct abnormal gas exchange (Day et al., 2010) In rare circumstances, surgery may be required to more quickly stabilize the flail segment (this only occurs if patient is unable to be ventilated) Regardless of severity all patients are carefully monitored by chest xrays, ABGs, pulse oximetry and bedside pulmonary function monitoring. Pain management is key to successful treatment (Day et al., 2010)
 In rare circumstances, surgery may be required to more quickly stabilize the flail segment (this only occurs if patient is unable to be ventilated) Regardless of severity all patients are carefully monitored by chest xrays, ABGs, pulse oximetry and bedside pulmonary function monitoring. Pain management is key to successful treatment (Day et al., 2010)")
26
Pulmonary Contusion Damage to the lung tissues resulting in hemorrhage and localized edema. The client is unable to clear secretions effectively, and the work of breathing is significantly increased Primary defect is the abnormal accumulation of fluid Pulmonary contusions are common thoracic injuries frequently associated with flail chest. It is defined as damage to the lungs tissues resulting in hemorrhage and localized edema. It is associated with trauma involving rapid compression and decompression (i.e. blunt trauma) (Day et al., 2010) The primary pathological defect is the abnormal accumulation of fluid in the lung. Often the patient has a constant cough, but is unable to clear the secretions. (Day et al., 2010)
 (Day et al., 2010) The primary pathological defect is the abnormal accumulation of fluid in the lung. Often the patient has a constant cough, but is unable to clear the secretions. (Day et al., 2010)")
27
Pulmonary Contusion Moderate Pulmonary Contusion:
Mucous, Serum and Frank Blood in the Tracheobroncial Tree Persistent Unproductive Cough Severe Pulmonary Contusion Central Cyanosis, Agitation, Combativeness Productive Cough with Frothy Bloody Secretions Treatment priorities are to maintain airway, provide oxygenation and pain management A patient with moderate pulmonary contusion has large amounts of mucus, serum and frank blood in the tracheobronchial tree – often the patient has a persistent cough but is unable to cough it up A patient with a severe pulmonary contusion may exhibit central cyanosis, agitation, combativeness and a productive cough with frothy bloody secretions Often, Pulmonary Constusions are not detected immediately. Changes to an x-ray show up 1-2 days after injury and appear as pulmonary infiltrates on the X-Ray Medical Management: Treatment priorities include maintaining the airway, provide oxygenation and controlling pain. In mild pulmonary contusion, IV fluids and oral fluids are beneficial to mobilize secretions (however intake must be monitored to prevent hypovolemia). Helpful techniques include postural drainage, physiotherapy including coughing and endotracheal suctioning Day et al., 2010
. Helpful techniques include postural drainage, physiotherapy including coughing and endotracheal suctioning. Day et al.,")
28
Cardiac Tamponade Compression of the heart as a result of fluid within the pericardial sac Usually due to chest trauma Manifestations Hypotension Jugular-venous distention Muffled heart sounds Periocardiocentesis to remove fluid from pericardial sac Cardiac tamponade: compression of the heart as a result of fluid within the pericardial sac usually resulting from trauma to the chest. Classical cardiac tamponade presents three signs. Hypotension occurs because of decreased stroke volume, jugular-venous distension due to impaired venous return to the heart, and muffled heart sounds due to fluid inside the Pericardium Compression of the heart as a result of fluid build-up in the pericardial sac. It usually is cause by blunt or penetrating trauma to the chest (Day et al., 2010) Cardiac tamponade also may follow diagnostic cardiac catheterization, angiographic procedures, pacemaker insertion, which can produce perforations of the heart and great vessels. Pericardial effusion with fluid compressing the heart may also develop from metastases to the pericardium from malignant tumours of the breast, lung and mediastinum and may or occur with lymphomas and leukemias, renal failure, TB and high-dose radiation to the chest (check Ch. 30) Pericardiocentesis is the treatment
 Cardiac tamponade also may follow diagnostic cardiac catheterization, angiographic procedures, pacemaker insertion, which can produce perforations of the heart and great vessels. Pericardial effusion with fluid compressing the heart may also develop from metastases to the pericardium from malignant tumours of the breast, lung and mediastinum and may or occur with lymphomas and leukemias, renal failure, TB and high-dose radiation to the chest (check Ch. 30) Pericardiocentesis is the treatment.")
29
Pulmonary Embolism Pulmonary embolism occurs when a blood clot becomes lodged in a lung artery, blocking blood flow to lung tissue. Blood clots often originate in the legs. The majority of all PEs are related to thrombi. Most of these clots originate in the deep calf, femoral, popliteal, or iliac veins. Up to 80% of patients diagnosed with a PE have thrombi in the lower legs (Moser, 1988). Other sources of emboli include tumors, air, fat, bone marrow, amniotic fluid, septic thrombi, and vegetations on heart valves.
. Other sources of emboli include tumors, air, fat, bone marrow, amniotic fluid, septic thrombi, and vegetations on heart valves.")
30
Nurses need to watch for it!
Pulmonary Embolism Blockage makes it more difficult for the heart to pump blood through lungs. As a result, less oxygen is available to the rest of the body. If the blockage is large enough, tissue death (infarction) occurs in the lung area cut off from circulation. Pulmonary embolisms are commonly misdiagnosed. Nurses need to watch for it!
 occurs in the lung area cut off from circulation. Pulmonary embolisms are commonly misdiagnosed. Nurses need to watch for it!")
31
Congestive heart failure
Misdiagnosed Why? Easily attributed to other conditions and vary with the size and number of clots. Such as a heart attack Pneumonia Hyperventilation Congestive heart failure Panic attacks. Misdiagnosed for

32
Who is at risk? Immobilization — Being immobilized puts a strain on the circulatory system. Although the heart acts as the body’s main pump, movement also assists in keeping blood circulating properly. Long periods of inactivity may increase risk of blood clots. Examples include lengthy road trips or flights, or bed rest due to illness or surgery. Blood abnormalities — Some people are born with blood that’s more prone to clotting & those dehydrated, septic, have Ca, those giving birth. The most predominant risk factors associated with PE are best described by what is known as Virchow's triad: venous stasis, endothelial injury, and hypercoagulation. Three different forces can contribute to venous stasis. These factors include: decreased velocity of blood flow through the vessels, venous dilation, and venous obstruction. Decreased velocity through the bloodstream is most often caused by immobility. When a person ambulates, the structures in the foot compress and calf muscles contract. These actions assist in propelling the blood from the lower extremities back to the heart. When immobile, whether due to bed rest or paralysis, blood return slows due to lack of muscle activity and venous stasis is likely to result. Venous pooling can also be exacerbated by immobility. When blood is allowed to pool in the veins, venous dilation and congestion develop. Other factors that can cause venous pooling are (a) heart failure with slow return of blood; (b) pregnancy due to increased volume of blood and obstruction of flow through the pelvis due to the fetus; (c) general anesthesia causing slowed heart rate and eliminating peripheral muscle contraction; (d) surgical positions with hips and knees flexed; and (e) obstruction that can be caused by tumors, edema, trauma or peripheral vascular disease. Venous stasis slows the ability of the venous system to carry away clotting factors. High levels of activated clotting factors can increase the likelihood of clot formation. Venous stasis may potentiate clot formation and cause vessel wall injury.
 heart failure with slow return of blood; (b) pregnancy due to increased volume of blood and obstruction of flow through the pelvis due to the fetus; (c) general anesthesia causing slowed heart rate and eliminating peripheral muscle contraction; (d) surgical positions with hips and knees flexed; and (e) obstruction that can be caused by tumors, edema, trauma or peripheral vascular disease. Venous stasis slows the ability of the venous system to carry away clotting factors. High levels of activated clotting factors can increase the likelihood of clot formation. Venous stasis may potentiate clot formation and cause vessel wall injury.")
33
Other Risk Factors for Pulmonary Embolism
Advanced age (especially over age 70) Significantly overweight Birth control pills, HRT drugs & the osteoporosis drug raloxifene (Evista) are examples of drugs that list a small risk of developing blood clots. Obesity places more pressure on the blood vessels in the lower extremeties which impairs venous return EVISTA® (raloxifene hydrochloride) is a selective estrogen receptor modulator
 Significantly overweight. Birth control pills, HRT drugs & the osteoporosis drug raloxifene (Evista) are examples of drugs that list a small risk of developing blood clots. Obesity places more pressure on the blood vessels in the lower extremeties which impairs venous return. EVISTA® (raloxifene hydrochloride) is a selective estrogen receptor modulator.")
34
About 90 % of Pulmonary Emboli Result When a Clot Travels from a Leg to a Lung - often no symptoms
Blood tests, a chest X-ray, an electrocardiogram — to help rule out other possible reasons for symptoms. Sometimes a leg blood clot may cause redness, swelling and pain in the calf muscle area. Refer to a physician promptly. A pulmonary angiogram is a more definitive test, although it involves some risk and is more expensive. the CT scan (computed tomography scan) — instead of lung scan or pulmonary angiogram. CT scan is a less invasive test that provides fast and accurate results.
 — instead of lung scan or pulmonary angiogram. CT scan is a less invasive test that provides fast and accurate results.")
35
Nursing Diagnosis for Chest Traumas
Impaired Gas Exchange Ineffective Airway Clearance Ineffective Breathing Patterns Imbalanced Fluid Volume Decreased Cardiac Output Decreased tissue perfusion Acute Pain Anxiety PC: Bleeding Risk for infection

36
Chest Tubes Read excerpt from article Managing a Chest Tube and Drainage System Chest Tube

37
What are Chest Tubes A chest tube is a large catheter inserted through the thorax to remove air, blood, pus or lymph Small Bore (12-20 Fr) Large Bore (24-32 Fr) A chest tube is a large catheter inserted through the thorax to remove air, blood, pus or lymph Perry & Potter, 2010)
 Large Bore (24-32 Fr) A chest tube is a large catheter inserted through the thorax to remove air, blood, pus or lymph. Perry & Potter, 2010)")
38
Indications for Use Pneumothorax Tension Pneumothorax
Bilateral Pneumothoraces Hemothorax Post-Operatively (Cardiac Surgery) Pleural Effusion Empyema Chylothorax Esophageal Rupture with Gastric Contents in Pleural Space Indications for use (Briggs, 2010): Persistent pneumothorax following failed needle aspiration Secondary pneumothorax not suitable for needle aspiration Pneumothorax when the patient requires mechanical ventilation Tension pneumothorax Bilateral pneumothoraces Traumatic pneumothorax Prophylactically in high-risk patients requiring ventilation Hemothorax Post-op, after cardiac surgery Symptomatic or recurrent pleural effusion Malignant pleural effusion Empyema (infected fluid-pus in the pleural space) Chylothorax (Chyle-lymphatic fluid in the pleural space) Esophageal rupture with gastric contents in pleural space (Briggs, 2010)
 Pleural Effusion. Empyema. Chylothorax. Esophageal Rupture with Gastric Contents in Pleural Space. Indications for use (Briggs, 2010): Persistent pneumothorax following failed needle aspiration. Secondary pneumothorax not suitable for needle aspiration. Pneumothorax when the patient requires mechanical ventilation. Tension pneumothorax. Bilateral pneumothoraces. Traumatic pneumothorax. Prophylactically in high-risk patients requiring ventilation. Hemothorax. Post-op, after cardiac surgery. Symptomatic or recurrent pleural effusion. Malignant pleural effusion. Empyema (infected fluid-pus in the pleural space) Chylothorax (Chyle-lymphatic fluid in the pleural space) Esophageal rupture with gastric contents in pleural space. (Briggs, 2010)")
39
Equipment Required Underwater seal drainage system
Chest tube of appropriate size Underwater seal drainage system Sterile gloves, gown and drapes Local anesthetic Skin Prep solution Chest Tube Tray Dressing Material Chest tube clamps Equipment Required by physician(Briggs, 2010): Chest tube of appropriate size Underwater seal drainage bottle filled to seal with sterile water Sterile gloves, gown and drapes Local anesthetic (lidocaine) Skin Prep solution Chest Tube Tray (all items are sterile – includes: knife handle, chest tube clamp, small sponge forceps, needle holder, knife blade, silk sutures, kelly clamps, 4x4 sponges, suture sissors, hand towels) Dressings: gauze, split chest tube dresses, 4-inch tape and elastic bandages Rubber tipped hemostats for chest tube clamps (Briggs, 2010)
: Chest tube of appropriate size. Underwater seal drainage bottle filled to seal with sterile water. Sterile gloves, gown and drapes. Local anesthetic (lidocaine) Skin Prep solution. Chest Tube Tray (all items are sterile – includes: knife handle, chest tube clamp, small sponge forceps, needle holder, knife blade, silk sutures, kelly clamps, 4x4 sponges, suture sissors, hand towels) Dressings: gauze, split chest tube dresses, 4-inch tape and elastic bandages. Rubber tipped hemostats for chest tube clamps. (Briggs, 2010)")
40
Chest Tubes Continued There are two types of Chest tubes: Pleural
Mediastinal

41
Pleural Chest Tube Durai, et al., 2010; Perry & Potter, 2010
Pleural Chest tubes are tubes inserted in the pleural space to remove air or fluid (Durai et al., 2010). Small bore chest tubes (12 – 20 Fr) are used to remove air and large bore chest tubes (24-32 Fr) are used to drain blood, pus or lymph (Perry & Potter, 2010). Small chest tubes used to remove air are inserted in the anterior 2nd or 3rd intercostal space. Because air rises, these chest tubes are placed high, allowing for air to leave the intrapleural space and the lung re-expands (Perry & Potter, 2010) Larger chest tubes used to drain blood, lymph or pus are inserted posterior and laterally around the 5th or 6th intercostal space. Fluid in the intrapleural space is affected by gravity and settles in the lower portion of the lung cavity, therefore placement of the tube needs to be lower (Perry & Potter, 2010) Durai, et al., 2010; Perry & Potter, 2010
. Small bore chest tubes (12 – 20 Fr) are used to remove air and large bore chest tubes (24-32 Fr) are used to drain blood, pus or lymph (Perry & Potter, 2010). Small chest tubes used to remove air are inserted in the anterior 2nd or 3rd intercostal space. Because air rises, these chest tubes are placed high, allowing for air to leave the intrapleural space and the lung re-expands (Perry & Potter, 2010) Larger chest tubes used to drain blood, lymph or pus are inserted posterior and laterally around the 5th or 6th intercostal space. Fluid in the intrapleural space is affected by gravity and settles in the lower portion of the lung cavity, therefore placement of the tube needs to be lower (Perry & Potter, 2010) Durai, et al., 2010; Perry & Potter,")
42
Mediastinal Chest Tubes
A mediastinal chest tube is placed in the mediastinum just below the sternum. This tube drains blood or fluid, preventing accumulation around the heart. It is most commonly used after open heart surgery. Cardiac Tamponade is another indication for Mediastinal chest tubes Perry & Potter, 2010

43
Pre-Insertion of Chest Tubes
Nurse prepares sterile table scalpel, local anesthetic (such as lidocaine), thick silk or polypropylene suture on a cutting needle, a chest tube of appropriate size and the underwater seal with sterile water filled to the mark Opens drain package and prepares drain as per manufacturers instructions Nurse Positions Patient for Procedure Explain Procedure and assure patient Monitor Vital Signs and for Discomfort Prior to insertion, the nurse prepares a sterile table with a scalpel, local anesthetic (such as lidocaine), thick silk or polypropylene suture on a cutting needle, a chest tube of appropriate size and the underwater seal with sterile water filled to the mark (Durai, 2010). * MD responsible for admin of analgesic (Durai, 2010)
, thick silk or polypropylene suture on a cutting needle, a chest tube of appropriate size and the underwater seal with sterile water filled to the mark. Opens drain package and prepares drain as per manufacturers instructions. Nurse Positions Patient for Procedure. Explain Procedure and assure patient. Monitor Vital Signs and for Discomfort. Prior to insertion, the nurse prepares a sterile table with a scalpel, local anesthetic (such as lidocaine), thick silk or polypropylene suture on a cutting needle, a chest tube of appropriate size and the underwater seal with sterile water filled to the mark (Durai, 2010). * MD responsible for admin of analgesic. (Durai, 2010)")
44
Methods for Insertion Two Methods for Tube Insertion
Trocar based (i.e. the Seldinger technique) Allows for easier insertion Greater Risk Less Painful Blunt dissection More painful for the patient Safest Method Durai, 2010
 Allows for easier insertion. Greater Risk. Less Painful. Blunt dissection. More painful for the patient. Safest Method. Durai,")
45
Chest Tube Insertion The steps in insertion of a chest drain are as follows: 1) The area is prepped and draped appropriately (sterile technique) 2) An incision is made along the upper border of the rib below the intercostal space to be used. 3) The drain track will be directed over the top of the lower rib to avoid the intercostal vessels lying below each rib. 4) The incision should easily accommodate the operator's finger. 5) Using a curved clamp the track is developed by blunt dissection only. The clamp is inserted into muscle tissue and spread to split the fibres. The track is further developed with the operator's finger. 6) Once the track comes onto the rib, the clamp is angled just over the rib and dissection continued until the pleural is entered. 7) A finger is inserted into the pleural cavity and the area explored for pleural adhesions. At this time the lung, diaphragm and heart may be felt, depending on position of the track. 8) The chest tube is mounted on the clamp and passed along the track into the pleural cavity. 9) The tube is connected to an underwater seal and sutured / secured in place. 10)The chest is re-examined to confirm effectiveness of procedure and a chest X-ray is taken to confirm placement & position (
 An incision is made along the upper border of the rib below the intercostal space to be used. 3) The drain track will be directed over the top of the lower rib to avoid the intercostal vessels lying below each rib. 4) The incision should easily accommodate the operator s finger. 5) Using a curved clamp the track is developed by blunt dissection only. The clamp is inserted into muscle tissue and spread to split the fibres. The track is further developed with the operator s finger. 6) Once the track comes onto the rib, the clamp is angled just over the rib and dissection continued until the pleural is entered. 7) A finger is inserted into the pleural cavity and the area explored for pleural adhesions. At this time the lung, diaphragm and heart may be felt, depending on position of the track. 8) The chest tube is mounted on the clamp and passed along the track into the pleural cavity. 9) The tube is connected to an underwater seal and sutured / secured in place. 10)The chest is re-examined to confirm effectiveness of procedure and a chest X-ray is taken to confirm placement & position (")
46
Site of Insertion

47
Site of Insertion

48
Digital Exploration

49
Drain Insertion

50
Drain Sutured in Place

51
Underwater Seal Drainage System

52
Chest Drainage Systems
Consist of three parts: Suction Source Collection Chamber for pleural drainage Mechanism to prevent air reentry Three types of chest drainage systems: Traditional Water Seal Dry Suction Water Seal Dry Suction with a One way Valve Chest drainage systems have a suction source, a collection chamber for pleural drainage, and a mechanism to prevent air from reentering the chest with inhalation. Various types of chest drainage systems are available for use in removal of air and fluid from the pleural space and reexpansion of the lungs. Chest drainage systems come with either wet (water seal) or dry suction control. In wet suction systems, the amount of suction is determined by the amount of water instilled in the suction chamber. The amount of bubbling in the suction chamber indicates the strength of the suction. Wet systems use a water seal to prevent air from moving back into the chest on inspiration. Dry systems use a one-way valve and may have a suction control dial in place of the water. Both systems can operate by gravity drainage, without a suction source. (Day et al., 2010).
 or dry suction control. In wet suction systems, the amount of suction is determined by the amount of water instilled in the suction chamber. The amount of bubbling in the suction chamber indicates the strength of the suction. Wet systems use a water seal to prevent air from moving back into the chest on inspiration. Dry systems use a one-way valve and may have a suction control dial in place of the water. Both systems can operate by gravity drainage, without a suction source. (Day et al., 2010).")
53
Traditional Water Seal Drainage System
Contains 3 Chambers: Collection chamber Water seal chamber Wet suction control chamber Additional suction source can be added as needed. Intermittent bubbling indicates proper functioning The traditional water seal chest drainage system, or wet seal, has three chambers: a collection chamber, a water seal chamber, and a wet suction control chamber. The collection chamber acts as a reservoir for fluid draining from the chest tube. It is graduated to permit easy measurement of drainage. Suction may be added to create negative pressure and promote drainage of fluid and removal of air. The suction control chamber regulates the amount of negative pressure applied to the chest. The amount of suction is determined by the water level. It is generally set at 20-cm of water; adding more fluid results in more suction. After the suction is turned on, bubbling appears in the suction chamber. A positive pressure valve is located at the top of the suction chamber that automatically opens with increases in positive pressure within the system. Air will automatically be released through a positive-pressure relief valve if the suction tubing is inadvertently clamped or kinked. The water seal chamber has a one-way valve or water seal that prevents air from moving back into the chest when a patient inhales. There will be an increase in the water level with inspiration and a return to the baseline level during exhalation; this is referred to as tidaling. Intermittent bubbling in the water seal chamber is normal, but continuous bubbling can indicate an air leak. Bubbling and tidaling do not occur when the tube is placed in the mediastinal space; however, fluid may pulsate with the patient’s heartbeat. If the chest tube is connected to gravity drainage only, suction is not used. The pressure is equal to the water seal only. Two-chamber chest drainage systems are available for use with patients who need only gravity drainage. The water level in the water seal chamber reflects negative pressure present in the intrathoracic cavity. A rise in the water level indicates negative pressure in the pleural or mediastinal space. Excessive neagtive pressure can cause trauma to tissue. Most chest drainage systems have an automatic means to prevent excessive negative pressure. By pressing and holding a manual high-negativity vent until the water level in the water seal chamber returns to the 2-cm mark, excessive negative pressure is avoided, preventing damage to tissue. (Day et al., 2010).
.")
54
Dry Suction Water Seal System
Contains 3 Chambers: Collection chamber Water seal chamber Wet suction control chamber Suction pressure is set with regulator. Has an indicator to signify suction pressure is adequate. Quieter than traditional water seal system. Dry suction water seal systems, or dry suction, have a collection chamber for drainage, a water seal chamber, and a dry suction control chamber. The water seal chamber is filled with air to the 2-cm level. Bubbling in this area can indicate an air leak. The dry suction control chamber contains a regulator dial that conveniently regulates vacuum to the chest drain. Water is not needed for suction as it is in the wet system. Without the bubbling in the suction chamber, the machine is quieter. However, if the container is knocked over, the water seal may be lost. Once the tube is connected to the suction source, the regulator dial allows the desired level of suction to be dialed in; the suction is increased until an indicator appears. The indicator has the same function as the bubbling in the traditional water seal system; that is, it indicates that the vacuum is adequate to maintain the desired level of suction. Some drainage systems use a bellows (a chamber that can be expanded or contracted) or an orange-coloured float device as an indicator of when the suction control regulator is set. When the water in the water seal rise above the 2-cm level, intrathoracic pressure increases. Dry suction water seal systems have a manual high-negativity vent located on top of the drain. The manual high-negativity vent is pressed until the indicator appears and the water level in the water seal returns to the desired level, indicating that the intrathoracic pressure is decreased. (Day et al., 2010).
 or an orange-coloured float device as an indicator of when the suction control regulator is set. When the water in the water seal rise above the 2-cm level, intrathoracic pressure increases. Dry suction water seal systems have a manual high-negativity vent located on top of the drain. The manual high-negativity vent is pressed until the indicator appears and the water level in the water seal returns to the desired level, indicating that the intrathoracic pressure is decreased. (Day et al., 2010).")
55
Dry Suction with One Way Valve System
Has a one-way mechanical valve that allows air to leave the chest and prevents air from moving back into the chest. Can be set up quickly in an emergency. Works even if knocked over, ideal for ambulatory patients. A third type of chest drainage system is dry suction with a one-way mechanical valve. This system has a collection chamber, a one-way mechanical valve, and a dry suction control chamber. The valve acts in the same way as a water seal and permits air to leave the chest but prevents it from moving back into the pleural space. This model lacks a water seal chamber and therefore can be set up quickly in emergency situations and the dry control drain still works even if it is knocked over. If the wet suction drain is knocked over, the water seal could be lost. This makes the dry suction systems useful for the patient who is ambulating or being transported. However, without the water seal chamber there is no way to tell by inspection if the pressure in the chest is changed, even though an air leak indicator is present so that the system can be checked. If an air leak is suspected, 30 mL of water are injected into the air leak indicator or the container is tipped so that fluid enters the air leak detection chamber. Bubbles will appear if a leak is present. If the chest tube has been inserted to re-expand a lung after pneumothorax, or if very little fluid drainage is expected, a one-way valve may be connected to the chest tube. This valve may be attached to a collection bag or covered with a sterile dressing if no drainage is expected. (Day et al., 2010).
.")
57
Post Insertion & Maintenance of Chest Tubes

58
Management of Chest Tube
The nurse is responsible for managing the chest tube and drainage system including: Caring for the tube and drainage system when transporting patient Changing or emptying the drainage container Monitoring fluid drainage Monitoring chest tube position Milking and clamping contraindicated The chest tube should never be clamped because this can cause a tension pneumothorax. When transporting the patient the nurse should ensure that the container remains upright and safely attached to the bedside, below the level of the patient to prevent backflow of drainage. If it is absolutely necessary that the drainage has to be kept above the level of the patient for a short period of time, the tubing must be clamped, and a specially trained nurse must be present to observe for signs and symptoms of oxygen desaturation. The only time you change or empty the drainage container is when it is full. Ensure that you do not empty the water seal chamber itself, if you do you need to ensure that it is immediately refilled to the marked level. When changing or emptying the drainage system, make sure that you clamp the chest tube and then unclamp it when you are finished. The nurse should alert the surgeon if the chest tube drains more than 250ml of bloody drainage in an hour or a total of more than 500ml is drained. (Durai, Hoque, & Davis, 2010).
.")
59
Drainage System Assessment
Monitor drainage collection System for: Verify that all connection tubes are patent and connected securely Assess that water seal is intact when using wet suction system and assess regulator dial in dry suction system Fluctuations in the water seal chamber for wet suction Air bubbles in the water seal chamber Air leak indicator in dry suction systems Suction set at ordered rate Keep the system below patient’s chest level Maintain appropriate fluid in the water seal for wet suction ME - assessments

60
Monitoring the Water-Seal Chamber
There will be an increase in the water level with inspiration and a return to the baseline level with exhalation. This is referred to as tidaling. If your patient’s lung fully expands or the tubing becomes obstructed, you may not see any fluctuations. Bubbling in the bottom of the water-seal chamber indicates an air leak, caused by poor tubing connections. You may notice a small amount of bubbling right after chest tube insertion, or when the patient coughs. Fluctuation of the water level in the water seal shows effective connection between the pleural cavity and the drainage chamber and indicates the drainage system remains patent. Fluctuation will occur in both wet and dry water seal suctions devices. Fluctuations will stop when: The lung has reexpanded The tubing is obstructed with blood clots, fibrin, or kinks A loop of tubing is hanging below the rest of the tubing Suction is not working properly

61
Monitoring Continued TIDALING BUBBLING Drainage collection Chamber
Underwater Seal Chamber Assessment & Management of Air Leak TIDALING BUBBLING Yes indicates patient air leak (pneumothorax) No indicates lung re-expansion or obstruction by kinks or clots indicates possible connection or system air leak observed with pneumonectomy or decreased lung compliance
 No. indicates lung re-expansion or obstruction by kinks or clots. indicates possible connection or system air leak. observed with pneumonectomy or decreased lung compliance.")
62
Patient Assessment Assess client for: Comfort level
Auscultate lung sounds, and assess for rate, rhythm, and depth. Monitor HR, BP, Temp, RR, O2 sats Drainage for amount, color and consistency Monitor dressing status and drainage from insertion site Monitor chest wall at insertion site for subcutaneous emphysema or air leaks Mark volume and drainage (time, date, initial) every shift. Mark tube to ensure that it does not become dislodged.
 every shift. Mark tube to ensure that it does not become dislodged.")
63
Drainage Assessment Mediastinal Chest Tube Pleural Chest Tube
Less than mL/hr immediately after surgery Approximately 500 mL in the first 24 hours Pleural Chest Tube Between mL may drain 3 hours post insertion The 24 hour rate is mL Drainage is grossly bloody during the first several hours post-op and slowly changes to serous. Dark red drainage is expected only during the immediate post-op period… Bright red drainage would indicate active bleeding. Remember: a sudden gush of drainage may be retained blood/fluid being released during position change. (Perry & Potter, 2010).
.")
64
Complications of CT drainage systems
Nurse must be aware of the reason for chest tube insertion and what type of drainage to expect. Tension pneumothorax may occur from incorrect placement of tube. Tube may become disconnected from drainage system. Tube may accidentally be pulled out of pleural space. Occlusion of the chest tube. Drainage system may be knocked over disrupting seal. Risk for infection. Me (Durai et al., 2010; Sullivan2008).
.")
65
What if the Tubing Becomes Dislodged?
Immediately cover the site with a dry, sterile dressing and call the physician. If air is heard leaking from the site, tape the dressing on only two or three sides to allow air to escape and prevent tension pneumothorax. Closely monitor the patient and prepare for reinsertion. There are also sterile occlusive dressings with one way valves to prevent a tension pneumothorax.

66
What if the chest tube becomes disconnected from the drainage system?
If the chest tube and drainage system become disconnected, air can enter the pleural space, producing a pneumothorax. To prevent pneumothorax if the chest tube is inadvertently disconnected from the drainage system, a temporary water seal can be established by immersing the chest tube’s open end in a bottle of sterile water. Or if possible reconnect to the water seal drainage system!

67
Removal of Chest Tube Explain Procedure Administer Analgesics
Remove Drain Cleanse Wound Apply Sterile Dressing Removal is only indicated with the problem or reason for insertion has been resolved (Sullivan, 2008) Although it is the physician who inserted the chest tube, articles suggest any nurse can remove the tube so long as they have sufficient training and it is done in a way that minimizes the risk of air re-entering the thorax – causing a pneumothorax. It requires 2 health care professionals for the procedure (Durai, 2010; Sullivan, 2008). Prior to removal, nurses should be aware of patient’s blood work (i.e. platelets level) and medications including anti-coagulants or thrombolytic s which would significantly impact their clotting (Sullivan, 2008) First, the procedure should be explained to the patient and the nurse needs to support the patient emotionally if needed – Patients report feeling less anxious and more prepared when the procedure is explained beforehand (Perry & Potter, 2010). Removing the chest tube can be painful for some patients, therefore it is important to administer analgesics prior and allowing enough time for it to take effect (usually 30 min). The pain experienced has been reported to be moderate (Sullivan, 2008) To start the removal, the securing sutures and purse string suture needs to be identified. Assist patient into a comfortable position. The patient needs to inhale deeply and hold their breath for the tube to be removed. Some evidence shows that removing the drain at end-inspiration or end-exhalation is equally safe, however the preferred method is end-inspiration. It is good to have the patient practice a few times inhaling and holding breath. The nurse pulls the drain tubing out in one quick and smooth motion. Once the drain is removed, the second nurse ties the purse-string suture and then instructs the patient to breath normally (Sullivan, 2008; Perry & Potter, 2010) Aseptically cleanse wound and apply occlusive sterile dressing. Firmly secure it in position with an elastic bandage (Perry & Potter, 2010) – The purse string suture can be removed in 7-12 days (Sullivan, 2008) (Durai, 2010; Sullivan, 2008; Perry & Potter, 2010)
 Although it is the physician who inserted the chest tube, articles suggest any nurse can remove the tube so long as they have sufficient training and it is done in a way that minimizes the risk of air re-entering the thorax – causing a pneumothorax. It requires 2 health care professionals for the procedure (Durai, 2010; Sullivan, 2008). Prior to removal, nurses should be aware of patient’s blood work (i.e. platelets level) and medications including anti-coagulants or thrombolytic s which would significantly impact their clotting (Sullivan, 2008) First, the procedure should be explained to the patient and the nurse needs to support the patient emotionally if needed – Patients report feeling less anxious and more prepared when the procedure is explained beforehand (Perry & Potter, 2010). Removing the chest tube can be painful for some patients, therefore it is important to administer analgesics prior and allowing enough time for it to take effect (usually 30 min). The pain experienced has been reported to be moderate (Sullivan, 2008) To start the removal, the securing sutures and purse string suture needs to be identified. Assist patient into a comfortable position. The patient needs to inhale deeply and hold their breath for the tube to be removed. Some evidence shows that removing the drain at end-inspiration or end-exhalation is equally safe, however the preferred method is end-inspiration. It is good to have the patient practice a few times inhaling and holding breath. The nurse pulls the drain tubing out in one quick and smooth motion. Once the drain is removed, the second nurse ties the purse-string suture and then instructs the patient to breath normally (Sullivan, 2008; Perry & Potter, 2010) Aseptically cleanse wound and apply occlusive sterile dressing. Firmly secure it in position with an elastic bandage (Perry & Potter, 2010) – The purse string suture can be removed in 7-12 days (Sullivan, 2008) (Durai, 2010; Sullivan, 2008; Perry & Potter, 2010)")
68
Post Removal Nursing Interventions
Respiratory Assessment Assess Vital Signs Chest X-Ray Assess Pain Assess Wound & Dressing - Auscultate lung sounds Palpate over lung where tube was inserted and observe for subcutaneous emphysema (SE results from entrance of air into the subcutaneous space – It is painful and as a result, patients may not take full lung expansion) Evaluate for respiratory distress immediately after tube removal and during first few hours (Perry & Potter, 2010) Evaluate patient’s vital signs (O2 sats, pulmonary status and psychological status) A chest x-ray should be completed post removal to check that neither fluid or air has re-collected in the pleural cavity. (Sullivan, 2008) Assess patient’s level of pain or discomfort. Observe for non-verbal cues of pain (grimacing, elevated BP, restlessness etc..) – This would indicate the wound did not close well. Assess wound and dressing for any signs of drainage, redness or inflammation which could indicate an infection (Perry & Potter, 2010).
 Evaluate for respiratory distress immediately after tube removal and during first few hours (Perry & Potter, 2010) Evaluate patient’s vital signs (O2 sats, pulmonary status and psychological status) A chest x-ray should be completed post removal to check that neither fluid or air has re-collected in the pleural cavity. (Sullivan, 2008) Assess patient’s level of pain or discomfort. Observe for non-verbal cues of pain (grimacing, elevated BP, restlessness etc..) – This would indicate the wound did not close well. Assess wound and dressing for any signs of drainage, redness or inflammation which could indicate an infection (Perry & Potter, 2010).")
69
Pain Management Related to:
Insertion – local anesthetic (lidocaine or prilocaine) In situ – PCA pump (morphine) Removal – EMLA cream (Eutectic mixture of Local Anesthetics) Overall goal is to provide pain management but not to the extent that respirations are depressed. ME Pain after a thoracotomy may be severe, depending on the type of incision and the patient’s reaction to and ability to cope with pain. Deep inspiration is very painful after thoracotomy. Pain can lead to postoperative complications if it reduces the patient’s ability to breathe deeply and cough and if it further limits chest excursions so that ventilation becomes ineffective. Overall, you need to treat the pain to prevent any of these complications. Insertion: Lidocaine and prilocaine are local anesthetic agents used to treat pain at the site of chest tube insertion. These medications are administered transdermally to penetrate the skin. Lidocaine and prilocaine have also been found effective when used together which is EMLA cream. In situ: because of the need to maximize patient comfort without depressing the respiratory drive, PCA is often used, most commonly with morphine. This allows the patient to control the frequency and total dosage with preset limits to avoid overdose. With proper instruction, PCA is well tolerated and allows earlier mobilization and cooperation with the treatment regime. EMLA cream has been found to be effective in treating pain from chest tube removal, a study showed it was more effective than morphine. However, many physicians prefer not to use analgesia when removing chest tubes because the pain, although severe, is of short duration, only a few minutes, and the analgesia may interfere with the respiratory effort.
 In situ – PCA pump (morphine) Removal – EMLA cream (Eutectic mixture of Local Anesthetics) Overall goal is to provide pain management but not to the extent that respirations are depressed. ME. Pain after a thoracotomy may be severe, depending on the type of incision and the patient’s reaction to and ability to cope with pain. Deep inspiration is very painful after thoracotomy. Pain can lead to postoperative complications if it reduces the patient’s ability to breathe deeply and cough and if it further limits chest excursions so that ventilation becomes ineffective. Overall, you need to treat the pain to prevent any of these complications. Insertion: Lidocaine and prilocaine are local anesthetic agents used to treat pain at the site of chest tube insertion. These medications are administered transdermally to penetrate the skin. Lidocaine and prilocaine have also been found effective when used together which is EMLA cream. In situ: because of the need to maximize patient comfort without depressing the respiratory drive, PCA is often used, most commonly with morphine. This allows the patient to control the frequency and total dosage with preset limits to avoid overdose. With proper instruction, PCA is well tolerated and allows earlier mobilization and cooperation with the treatment regime. EMLA cream has been found to be effective in treating pain from chest tube removal, a study showed it was more effective than morphine. However, many physicians prefer not to use analgesia when removing chest tubes because the pain, although severe, is of short duration, only a few minutes, and the analgesia may interfere with the respiratory effort.")
70
Case Study JB is a 25 year old male just arrived to the ER via EHS. Only known hx is that JB was involved in a head on collision with a drunk driver. JB is transferred to trauma stretcher and immediately you notice he is anxious and in pain. He is having difficulty breathing and his seatbelt has left him with bruising across the chest. Vital signs are BP 85/50mmHg, HR 120, RR 30, Temp is 37.o, and Sp02 is 90%. What type of chest trauma is suspected? What initial assessments would you want to perform? Blunt chest trauma. Assessments: chest expansion, peridoxical chest wall motion, trachea for deviation, tenderness, cruching/crepitus, percuss for dullness/resonance, Auscultate for crackles, air entry.

71
What size chest tube did you grab?
Following assessment it is determined JB has a hemothorax and a chest tube is required. What equipment would you gather for the physician? What size chest tube did you grab? You notice the physician is landmarking for the 2nd or 3rd intercostal space, what do you do? What are some complications of chest tube drainage systems? Chest tube of appropriate size Underwater seal drainage system Sterile gloves, gown and drapes Local anesthetic Skin Prep solution Chest Tube Tray Dressing Material Chest tube clamps Large Bore Fr Tell him to hold up, it goes into the 5th and 6th ICS, b/c gravity pulls fluid to base of lungs – 2nd – 3rd ICS is to remove air (air rises) Nurse must be aware of the reason for chest tube insertion and what type of drainage to expect. Tension pneumothorax may occur from incorrect placement of tube. Tube may become disconnected from drainage system. Tube may accidentally be pulled out of pleural space. Occlusion of the chest tube. Drainage system may be knocked over disrupting seal. Risk for infection.
 Nurse must be aware of the reason for chest tube insertion and what type of drainage to expect. Tension pneumothorax may occur from incorrect placement of tube. Tube may become disconnected from drainage system. Tube may accidentally be pulled out of pleural space. Occlusion of the chest tube. Drainage system may be knocked over disrupting seal. Risk for infection.")
72
Questions & Comments ?

73
References Briggs, D. (2010). Nursing care and management of patients with intrapleural drains. Nursing Standard. 24(21), Durai, R., Hoque, H., Davies, T.W. (2010). Managing a chest tube and drainage system. Association of Perioperative Registered Nurses. (91) 2, Day,R.A., Paul,P., Williams,B.,Smeltzer,S.C. & Bare,B.(2009). Textbook of Canadian Medical Surgical Nursing. Philadelphia, PA: Lippincott Williams & Wilkins. Pearce, A.P. (2009). Chest drain insertion: Improving techniques and decreasing complications. Emergency Medicine Australia. (21), Perry & Potter . (2010). Clinical Nursing Skills & Techniques (7th ed.). St. Louis: Mosby,. Sullivan, B. (2008). Nursing management of patients with a chest drain. British Journal of Nursing. (17)6, Trauma. Org. (2004). Chest trauma: Initial Evaluation. Retrieved from
. Nursing care and management of patients with intrapleural drains. Nursing Standard. 24(21), Durai, R., Hoque, H., Davies, T.W. (2010). Managing a chest tube and drainage system. Association of Perioperative Registered Nurses. (91) 2, Day,R.A., Paul,P., Williams,B.,Smeltzer,S.C. & Bare,B.(2009). Textbook of Canadian Medical Surgical Nursing. Philadelphia, PA: Lippincott Williams & Wilkins. Pearce, A.P. (2009). Chest drain insertion: Improving techniques and decreasing complications. Emergency Medicine Australia. (21), Perry & Potter . (2010). Clinical Nursing Skills & Techniques (7th ed.). St. Louis: Mosby,. Sullivan, B. (2008). Nursing management of patients with a chest drain. British Journal of Nursing. (17)6, Trauma. Org. (2004). Chest trauma: Initial Evaluation. Retrieved from")
Similar presentations





, FCCP>")














