Download presentation
Presentation is loading. Please wait.

1
LASIK: How It’s Done Vincent J. Marino, D.O. FAOCO Medical Director, LASIKPlus Cincinnati & Dayton, OH 7840 Montgomery Rd. Cincinnati, OH 45236 6470 Centerville Business Parkway, Centerville, OH 45459

2
LASIK: How It’s Done Pretest Question #1 What percentage of LASIK patients achieve uncorrected visual acuity of 20/40 vision or better? A.99% * B.94% C.75% D.50%

3
LASIK: How It’s Done Pretest Question #2 What group below best describes the population that acquires presbyopia (age related loss of near vision)? A.Presbyopia only effects some people over the age of 40. B.Presbyopia effects all individuals over the age of 40 regardless of glass prescription. * C.Presbyopia only happens to your parents. D.Myopic (nearsighted) individuals can not become presbyopic.
 individuals can not become presbyopic..")
4
20 th Annual Grandview Family Practice Conference February 20, 2015 Vincent J. Marino, DO 1992 - Nova Southeastern University College of Osteopathic Medicine 1993 - Internship Grandview Hospital 1996 - Residency Ophthalmology Grandview Hospital Fellow American Osteopathic College of Ophthalmology 1996 – Present, LASIKPlus Cincinnati & Dayton, OH Experience 86,000 LASIK surgeries

5
LASIK LASIK: acronym l(aser) as(sisted) i(n-situ) k(eratomileusis) eye surgery to correct vision in which a laser reshapes the inner cornea.
 as(sisted) i(n-situ) k(eratomileusis) eye surgery to correct vision in which a laser reshapes the inner cornea.")
6
Why does one undergo elective refractive surgery? Has a Myopic, Hyperopic, Astigmatic refraction (glasses Rx).
..")
7
Why does one undergo elective refractive surgery? Tired of wearing glasses More than 150 million Americans use corrective eyewear to compensate for refractive errors. 1

8
Why does one undergo elective refractive surgery? Contact lens intolerant or over wears contact lenses. More than 30 million people in the U.S. wear contact lenses. Serious eye infections that can lead to blindness affect up to 1 out of every 500 contact lens users per year. Not following proper contact lens care instructions Between 40%-90% of contact lens wearers do not properly follow the care instructions for their contact lenses. Improper cleaning and irregular replacement of contact lenses and contact lens cases—as well as other behaviors relating to contact lens hygiene and care— have been linked to a higher risk of complications.

9
Why does one undergo elective refractive surgery? Activities that makes contacts or glasses hard to wear Job (firefighting, police), Military, sports
, Military, sports.")
10
History of refractive surgery 4 1988 Marguerite B. McDonald, MD First PRK 1989 Gholam A. Peyman, MD patent on flap production 1999 LASIK formally approved by the FDA

11
Elective surgery LASIK is the world’s most popular elective procedure—more than 28 million LASIK procedures have been performed worldwide.

12
Candidacy Good medical health, good ocular health, good topography, good pachymetry (corneal thickness) > 18 years and stable refraction Insure that healing for an elective surgery may go well. Rx in range =/- 0.75D or greater. Up to -11.00 Diopers of Myopia Up to +5.00 Diopters of Hyperopia Up to -6.00 Diopters of Astigmatism

13
Candidacy Refractive Range Measured in units of optical units Diopter (D) o 1 Diopter = 1/meter (f) Emmetropia = +/- 0.5 D Astigmatism 0 ------------------------------(-6 D)------>
 o 1 Diopter = 1/meter (f) Emmetropia = +/- 0.5 D Astigmatism (-6 D)------>")
14
Evaluation Medical and family history Dilated eye exam Refraction objective and subjective IOP (intra ocular pressure) Corneal Topography Aberrometry Pachymetry (corneal thickness)
 Corneal Topography Aberrometry Pachymetry (corneal thickness)")
15
Evaluation Topography

16
Aberrometry Evaluation Aberrometry

17
Consent Goals and expectations (20/40 or better, most will achieve 20/20 or better) Review enhancement limits, may do second surgery if Rx drifts (3-4%) if Rx drift. Usually less than one Diopter. Presbyopia education (over 40 years, need reading glasses if both eyes are corrected for distance). Monovision option Review risk, benefits and alternatives
. Monovision option Review risk, benefits and alternatives.")
18
Presbyopia Near Vision reflex o Convergence o Pupil constriction o Accommodation Loss of accommodation due to age = presbyopia

19
Presbyopia Loss of near vision due to age o Loss of accommodation (focusing power) o All individuals regardless of refraction o 40 years and older o Progressive Results from the thickening and loss of flexibility of the natural lens Stabilizes in mid-sixties o Myopes with a refractive range of -1.00 to -3.00 diopter can read without glasses. Myopes become presbyopic and experience blurred vision at near with their spectacle (eye glass) correction.
 correction..")
20
Presbyopia Monovision Optional treatment method to decrease the dependence on glasses for both distance and near vision for individuals over 40 years. Dominant eye is corrected for distance Non Dominant eye is corrected for near Monovision can be set up with contact lenses or LASIK “Blended vision” Functional vision, not perfect at distance or near. Compromise, “best of both worlds”. Monovision patients may require part time glasses for driving and fine near vision.

21
Equipment Flap production Femtosecond laser VS Microkeratome Microkeratome: Buttonhole, partial flap, suction loss, less stable refractive outcome re non-planar flap (thinner in the middle) Femtosecond laser: scars may yield incomplete flaps but are rare. Able to reapply suction after suction loss and complete flap. More stable refractive outcomes. Lower incidence of dry eye. Ability to produce thinner flaps to conserve corneal tissue and provide higher refractive treatments.

22
Surgery Microkeratome blade inspection

23
Surgery Microkeratome assembled

24
Surgery Femtosecond laser

25
Equipment Femtosecond laser

26
Surgery Surgical instruments

27
Excimer laser Visx, Wavelight

28
Surgery Proparicaine anesthetic drops last 30 minutes

29
Surgery Flap production

30
Surgery Flap dissection and lift

31
Surgery Excimer laser refractive ablation

32
Surgery Flap reposition

33
Surgery Removal of debris Slit lamp

34
Surgery flap production suction ring

36
Surgery flap production docking

38
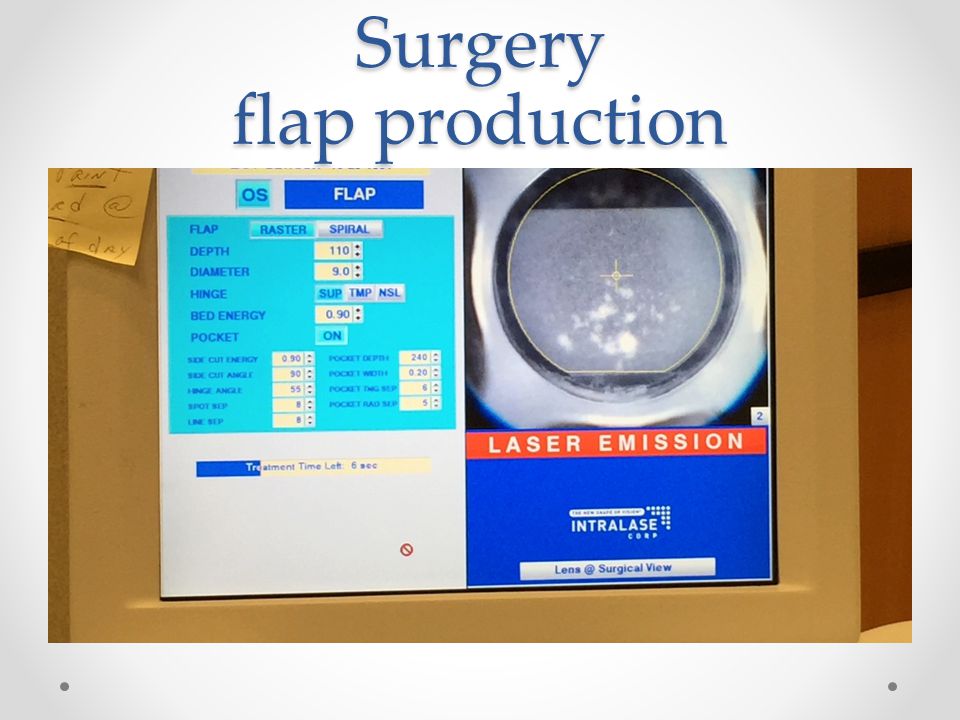
Surgery flap production

41
Post Operative follow up and care Rest for four hours with eyes closed mild burning expected No eye rubbing No swimming or hot tubs for one week Inflammation and infection warning signs given Diving vision expected at day one Antibiotic and steroid drops for one week

42
Recovery Post Operative follow up and care: Rest for four hours with eyes closed mild burning expected Diving vision expected at day one Antibiotic and steroid drops for one week

43
Recovery Most patients achieve 20/40 to 20/20 (driving vision) the next day. Most patients report near glasses like vision on day one. The quality of their vision improves dramatically through the weeks one to 12. Complete refractive stability occurs at about one year.

44
Recovery Patients are instructed not to rub their eyes for one week to prevent the flap from being dislodged (a rare complication but easily repaired). Protective safety glasses are worn during sleep for the first week.

45
Post Operative follow up and care One day o Ensure that the flap is in good position o Dry eye o inflammation o Infection One month o Refractive outcome o Dry eye Three months o Refractive outcome o Dry eye Annual exams o Insure good ocular health and refractive stability

46
Outcomes 94% 20/20 or better 99% 20/40 or better 3-4 % enhancement rate (second surgery) o Uncorrected visual acuity 20/30 or worse o Manifest (subjective) refraction +/- 0.75 Diopters o Difficulty with night vision o Refractive shift over time o residual refraction
 o Uncorrected visual acuity 20/30 or worse o Manifest (subjective) refraction +/ Diopters o Difficulty with night vision o Refractive shift over time o residual refraction")
47
Patient satisfaction 95% of patients are satisfied and have no further need for additional surgery. 3% require enhancement (second surgery) o Reasons: patient expectations and refractive shift. o most second surgeries occur years to decades secondary to small Rx shifts.
 o Reasons: patient expectations and refractive shift. o most second surgeries occur years to decades secondary to small Rx shifts..")
48
Complications Dry eye Diffuse Lamellar Keratitis Ectasia Flap Complications Suspicious settings

49
Future of LASIK Topography guided treatments for asymmetric corneas cross linking for ectasia and keratoconus

50
PRK Surface laser without the flap

Similar presentations






 in Adolescents S. Lance Forstot, MD, FACS The author has no financial interest in the subject matter of this.>")














>")
