Download presentation
Presentation is loading. Please wait.

1
Surgery Grand Rounds JoAnne M. LaRow, D.O. October 27, 2004

2
Nasal Cutaneous Flaps Alternative for repair of centrally located nasal skin defects < or equal to 2.5cm in greatest diameter Alternative for repair of centrally located nasal skin defects < or equal to 2.5cm in greatest diameter Useful for elderly pts because their skin is lax & mobile Useful for elderly pts because their skin is lax & mobile When designed properly flaps have advantage of color, texture, & thickness similar to those of the missing skin of the defect When designed properly flaps have advantage of color, texture, & thickness similar to those of the missing skin of the defect NCF’s are not sufficient to resurface an entire aesthetic unit of the nose & the scars produced may not always fall in the borders between aesthetic units NCF’s are not sufficient to resurface an entire aesthetic unit of the nose & the scars produced may not always fall in the borders between aesthetic units However, the ultimate contour of the nasal repair is far more important aesthetically than the location or # of scars However, the ultimate contour of the nasal repair is far more important aesthetically than the location or # of scars

3
Types Pivotal, advancement, or V-to-Y island pedicle advancement Pivotal, advancement, or V-to-Y island pedicle advancement Pivotal flaps such as single lobe transposition & rotation flaps are confined to repair of skin defects of the central & upper nasal vault where nasal skin is thin, mobile, & more redundant Pivotal flaps such as single lobe transposition & rotation flaps are confined to repair of skin defects of the central & upper nasal vault where nasal skin is thin, mobile, & more redundant V-to-Y island pedicle advancement flaps are limited to small defects of the anterior alar groove V-to-Y island pedicle advancement flaps are limited to small defects of the anterior alar groove For the caudal nose, bilobe flap is the most versatile & useful For the caudal nose, bilobe flap is the most versatile & useful

5
Primary Closure

6
A.H. Pt is 62 yr old A.H. Pt is 62 yr old Defect 1.6 x 1.1cm Defect 1.6 x 1.1cm Nodular basal cell carcinoma Nodular basal cell carcinoma I Stage Mohs procedure I Stage Mohs procedure Primary closure Primary closure

7
Rotation Flap Pivotal flaps with a curvilinear configuration Pivotal flaps with a curvilinear configuration Can be used anywhere on the nose except the ala Can be used anywhere on the nose except the ala Restricted to defects < 1.0-cm or less Restricted to defects < 1.0-cm or less Best for repairing triangular defects b/c portions of the standing cutaneous deformity that naturally form as the flap is pivoted are used to fill the triangle, reducing the need for excision Best for repairing triangular defects b/c portions of the standing cutaneous deformity that naturally form as the flap is pivoted are used to fill the triangle, reducing the need for excision Design flap so the length of its curvilinear border is 4 times the width of the defect Design flap so the length of its curvilinear border is 4 times the width of the defect With a 4:1 ratio, excision of a Burrow triangle is usually not necessary With a 4:1 ratio, excision of a Burrow triangle is usually not necessary A z-plasty at the pivotal point of the flap eases transfer & may eliminate the need to excise a Burrow triangle A z-plasty at the pivotal point of the flap eases transfer & may eliminate the need to excise a Burrow triangle

8
A.) A rotation flap designed to repair a 1.0-cm superficial skin defect A.) A rotation flap designed to repair a 1.0-cm superficial skin defect B.) the flap is pivoted into place. Z-plasty at the pivotal point eliminated the need to excise Burow’s triangle to equalize the length of wound borders B.) the flap is pivoted into place. Z-plasty at the pivotal point eliminated the need to excise Burow’s triangle to equalize the length of wound borders C.) A 4-month postoperative view C.) A 4-month postoperative view
 the flap is pivoted into place. Z-plasty at the pivotal point eliminated the need to excise Burow’s triangle to equalize the length of wound borders C.) A 4-month postoperative view C.) A 4-month postoperative view.")
9
V-toY Island Pedicle Advancement Flap Effective for small defects in region of anterior alar groove between the ala & tip Effective for small defects in region of anterior alar groove between the ala & tip Useful for skin defects up to 1.5-cm located in the junctional zone between the nasal tip & ala, including the nasal facet Useful for skin defects up to 1.5-cm located in the junctional zone between the nasal tip & ala, including the nasal facet A triangular flap, with its base making up the cephalic border of the defect, is designed with apex of the flap positioned laterally A triangular flap, with its base making up the cephalic border of the defect, is designed with apex of the flap positioned laterally The inferior border of flap rests in alar groove The inferior border of flap rests in alar groove Superior border extends laterally from the defect to include of nasal sidewall & tapers to meet the inferior border in the alar facial sulcus Superior border extends laterally from the defect to include of nasal sidewall & tapers to meet the inferior border in the alar facial sulcus Flap is incised to level of perichondrium of the lateral crus Flap is incised to level of perichondrium of the lateral crus Adjacent skin is widely undermined over nasal tip, dorsum, & sidewall, extending inferiorly beneath the skin of the ala to level of the caudal border of the defect Adjacent skin is widely undermined over nasal tip, dorsum, & sidewall, extending inferiorly beneath the skin of the ala to level of the caudal border of the defect Undermining is done to free the distal & proximal (distal) aspects down to subcutaneous plane Undermining is done to free the distal & proximal (distal) aspects down to subcutaneous plane Muscle & underlying fat in the middle are left alone & represent the pedicle Muscle & underlying fat in the middle are left alone & represent the pedicle This zone of tissue attachment in the center provides mobility for advancement This zone of tissue attachment in the center provides mobility for advancement Vascular supply is from the alar branch of the angular artery-which can be seen during dissection; it perforates the deep tissues in the extreme lateral aspect of the alar groove Vascular supply is from the alar branch of the angular artery-which can be seen during dissection; it perforates the deep tissues in the extreme lateral aspect of the alar groove The vessel is preserved whenever possible to provide flap with more axial vascular supply The vessel is preserved whenever possible to provide flap with more axial vascular supply
 aspects down to subcutaneous plane Undermining is done to free the distal & proximal (distal) aspects down to subcutaneous plane Muscle & underlying fat in the middle are left alone & represent the pedicle Muscle & underlying fat in the middle are left alone & represent the pedicle This zone of tissue attachment in the center provides mobility for advancement This zone of tissue attachment in the center provides mobility for advancement Vascular supply is from the alar branch of the angular artery-which can be seen during dissection; it perforates the deep tissues in the extreme lateral aspect of the alar groove Vascular supply is from the alar branch of the angular artery-which can be seen during dissection; it perforates the deep tissues in the extreme lateral aspect of the alar groove The vessel is preserved whenever possible to provide flap with more axial vascular supply The vessel is preserved whenever possible to provide flap with more axial vascular supply")
10
A.) 1.5-cm skin defect of the anterior alar groove A.) 1.5-cm skin defect of the anterior alar groove B.) A V-to-Y island advancement flap is designed B.) A V-to-Y island advancement flap is designed C.) Flap is mobilized on the muscle pedicle beneath the center of the flap. Pedicle is freed from the nasal cartilage sufficiently to permit only the exact degree of flap advancement necessary for wound repair C.) Flap is mobilized on the muscle pedicle beneath the center of the flap. Pedicle is freed from the nasal cartilage sufficiently to permit only the exact degree of flap advancement necessary for wound repair D.) The flap in position. The donor site is closed in a Y configuration D.) The flap in position. The donor site is closed in a Y configuration E &F) A 2-month postoperative view E &F) A 2-month postoperative view
 Flap is mobilized on the muscle pedicle beneath the center of the flap. Pedicle is freed from the nasal cartilage sufficiently to permit only the exact degree of flap advancement necessary for wound repair D.) The flap in position. The donor site is closed in a Y configuration D.) The flap in position. The donor site is closed in a Y configuration E &F) A 2-month postoperative view E &F) A 2-month postoperative view.")
11
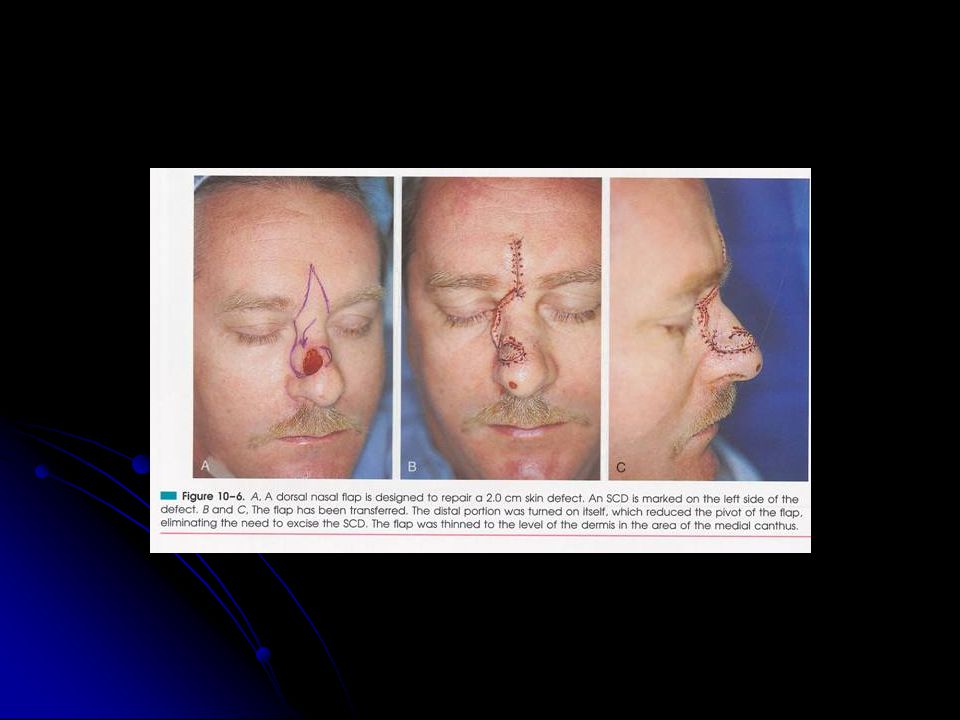
Dorsal Nasal Flap Recruits redundant skin of glabella & is a pivotal flap that can be used to repair skin defects of nasal tip, dorsum, & sidewall Recruits redundant skin of glabella & is a pivotal flap that can be used to repair skin defects of nasal tip, dorsum, & sidewall Allows repair of large lower & mid-nasal defects measuring 2.5-cm or less Allows repair of large lower & mid-nasal defects measuring 2.5-cm or less Ideal for elderly pts of defects located centrally on the tip Ideal for elderly pts of defects located centrally on the tip First assess skin laxity by pinch test: grasp skin between thumb & index finger -1-2-cm of skin on nasal bridge & glabella is needed First assess skin laxity by pinch test: grasp skin between thumb & index finger -1-2-cm of skin on nasal bridge & glabella is needed

12
Usually designed as a laterally based pivotal flap Usually designed as a laterally based pivotal flap Pedicle is centered in region of medial canthus Pedicle is centered in region of medial canthus A curvilinear line is drawn laterally from the defect to the junction of the cheek & nose A curvilinear line is drawn laterally from the defect to the junction of the cheek & nose From that point the line is directed superiorly, passing 0.5 cm medial to medial canthus & extending to superior aspect of glabella within glabellar crease From that point the line is directed superiorly, passing 0.5 cm medial to medial canthus & extending to superior aspect of glabella within glabellar crease Supplemental flap height is gained from glabella extension Supplemental flap height is gained from glabella extension From the nasofrontal angle, the glabellar height is 1.5-2 x the vertical height of the defect From the nasofrontal angle, the glabellar height is 1.5-2 x the vertical height of the defect From the superior point of the glabellar extension, a line angles inferiorly toward the contralateral medial canthus, creating a 30- to 45 degree angle backcut From the superior point of the glabellar extension, a line angles inferiorly toward the contralateral medial canthus, creating a 30- to 45 degree angle backcut This backcut remains superior to the level of the medial canthal tendon to protect the axial vessels from the angular artery (located inferior to the tendon) This backcut remains superior to the level of the medial canthal tendon to protect the axial vessels from the angular artery (located inferior to the tendon) Portion of the flap in the glabella region is undermined in the subcutaneous plane, the portion remaining is undermined beneath the nasal musculature Portion of the flap in the glabella region is undermined in the subcutaneous plane, the portion remaining is undermined beneath the nasal musculature Disadvantage of DNF is a cephalic displacement of nostril margin & nasal tip Disadvantage of DNF is a cephalic displacement of nostril margin & nasal tip In older pts this may be beneficial, but not in younger pts In older pts this may be beneficial, but not in younger pts Watch for a dicrepancy in thickness between flap & native skin in medial canthus Watch for a dicrepancy in thickness between flap & native skin in medial canthus
 This backcut remains superior to the level of the medial canthal tendon to protect the axial vessels from the angular artery (located inferior to the tendon) Portion of the flap in the glabella region is undermined in the subcutaneous plane, the portion remaining is undermined beneath the nasal musculature Portion of the flap in the glabella region is undermined in the subcutaneous plane, the portion remaining is undermined beneath the nasal musculature Disadvantage of DNF is a cephalic displacement of nostril margin & nasal tip Disadvantage of DNF is a cephalic displacement of nostril margin & nasal tip In older pts this may be beneficial, but not in younger pts In older pts this may be beneficial, but not in younger pts Watch for a dicrepancy in thickness between flap & native skin in medial canthus Watch for a dicrepancy in thickness between flap & native skin in medial canthus")
13
A.) the dorsal nasal flap is a pivotal flap based on the branches of the angular artery. The glabellar portion (shaded) is dissected in the subcutaneous plane A.) the dorsal nasal flap is a pivotal flap based on the branches of the angular artery. The glabellar portion (shaded) is dissected in the subcutaneous plane B.) the nasal portion is dissected beneath the musculature. An SCD is excised in or parallel to the alar groove B.) the nasal portion is dissected beneath the musculature. An SCD is excised in or parallel to the alar groove
 is dissected in the subcutaneous plane A.) the dorsal nasal flap is a pivotal flap based on the branches of the angular artery. The glabellar portion (shaded) is dissected in the subcutaneous plane B.) the nasal portion is dissected beneath the musculature. An SCD is excised in or parallel to the alar groove B.) the nasal portion is dissected beneath the musculature. An SCD is excised in or parallel to the alar groove.")
16
D-G) preoperative view & 6-month postoperative view D-G) preoperative view & 6-month postoperative view
 preoperative view & 6-month postoperative view D-G) preoperative view & 6-month postoperative view")
17
Dorsal Heminasal Flap A modified desogn of the DNF for mid-line defects of the upper dorsum A modified desogn of the DNF for mid-line defects of the upper dorsum Lateral border of the flap remains anterior to the thin skin of the medial canthus to avoid mismatch in skin thickness Lateral border of the flap remains anterior to the thin skin of the medial canthus to avoid mismatch in skin thickness The design limits the arc of tissue movement The design limits the arc of tissue movement It can be used for smaller defects (<2-cm) of nasal bridge that are 1-cm away from nostril margin It can be used for smaller defects (<2-cm) of nasal bridge that are 1-cm away from nostril margin DHF does not necessarily need a glabellar incision DHF does not necessarily need a glabellar incision Lateral incision is along the junction of the nasal sidewall & dorsum & therefore recruits skin only from the nasal bridge Lateral incision is along the junction of the nasal sidewall & dorsum & therefore recruits skin only from the nasal bridge
 of nasal bridge that are 1-cm away from nostril margin It can be used for smaller defects (<2-cm) of nasal bridge that are 1-cm away from nostril margin DHF does not necessarily need a glabellar incision DHF does not necessarily need a glabellar incision Lateral incision is along the junction of the nasal sidewall & dorsum & therefore recruits skin only from the nasal bridge Lateral incision is along the junction of the nasal sidewall & dorsum & therefore recruits skin only from the nasal bridge")
19
Bilobed Flap The most useful of the NCF’s The most useful of the NCF’s Is the flap of choice for reconstruction of certain defects of the lower third of the nose Is the flap of choice for reconstruction of certain defects of the lower third of the nose It is a double transposition flap It is a double transposition flap Whenever possible, bilobed flap is based laterally Whenever possible, bilobed flap is based laterally Medial-based flaps are hardy, but vascular supply is not as good Medial-based flaps are hardy, but vascular supply is not as good Ideal flaps for defects < 1.5-cm max dimention, located on central or lateral nasal tip without extension to ala Ideal flaps for defects < 1.5-cm max dimention, located on central or lateral nasal tip without extension to ala The defect should be at least 0.5-cm above margin of the nostril The defect should be at least 0.5-cm above margin of the nostril Flap recruits skin from mid-dorsum & sidewall where more generous skin laxity allows primary repair of the second lobe Flap recruits skin from mid-dorsum & sidewall where more generous skin laxity allows primary repair of the second lobe Estimate laxity by pinching the lateral nasal skin between the thumb & index finger Estimate laxity by pinching the lateral nasal skin between the thumb & index finger Pts with thick sebaceous skin have a higher risk of developing flap necrosis, trapdoor deformity, & depressed scars Pts with thick sebaceous skin have a higher risk of developing flap necrosis, trapdoor deformity, & depressed scars

21
A.) A distance equal to the radius of the defect (lxr) is measured from the lateral border of the defect to the pivotal point of the 2 lobes A.) A distance equal to the radius of the defect (lxr) is measured from the lateral border of the defect to the pivotal point of the 2 lobes 2 arcs are drawn with their centers at the pivotal point. 1 arc passes through the center of & the other tangential to the defect. Bases of both lobes arise from the first arc. The height of the first lobe extends to the second arc. The width of the first lobe equals the width of the defect 2 arcs are drawn with their centers at the pivotal point. 1 arc passes through the center of & the other tangential to the defect. Bases of both lobes arise from the first arc. The height of the first lobe extends to the second arc. The width of the first lobe equals the width of the defect B.) The axes of the defect & the 2 lobes of the flap are approx. 45degrees apart B.) The axes of the defect & the 2 lobes of the flap are approx. 45degrees apart
 The axes of the defect & the 2 lobes of the flap are approx. 45degrees apart B.) The axes of the defect & the 2 lobes of the flap are approx. 45degrees apart.")
22
C. the donor site of the second lobe is closed first. The first lobe is transposed & the SCD is removed. The second lobe is then transposed & trimmed C. the donor site of the second lobe is closed first. The first lobe is transposed & the SCD is removed. The second lobe is then transposed & trimmed D. The skin incisions are repaired with vertical matress sutures D. The skin incisions are repaired with vertical matress sutures

25
F-H, A 1-yr postoperative view. The flap was dermabraded 2 months after the transfer. F-H, A 1-yr postoperative view. The flap was dermabraded 2 months after the transfer.

26
MT: 64 yr-old MT: 64 yr-old Nodular BCC right nasal sidewall Nodular BCC right nasal sidewall

27
2 stage Mohs sx 2 stage Mohs sx Defect:1.2 x 1.0 cm Defect:1.2 x 1.0 cm Bilobed flap Bilobed flap

28
MT

38
NS NS: 72 yr-old NS: 72 yr-old BCC nasal tip BCC nasal tip 2 stage Mohs 2 stage Mohs Defect: 1.4 x.9-cm Defect: 1.4 x.9-cm Closure: bilobed flap Closure: bilobed flap

39
LB: 72 yr-old LB: 72 yr-old Nodular BCC nasal tip Nodular BCC nasal tip

41
1 stage Mohs sx 1 stage Mohs sx Defect: 1.2 x1.0 cm Defect: 1.2 x1.0 cm

44
CH: CH: SCC left nasal ala SCC left nasal ala 1 stage Mohs sx 1 stage Mohs sx Defect: 0.7 x 0.8- cm Defect: 0.7 x 0.8- cm

45
f/u 5 months later f/u 5 months later

46
f/u 7 months later f/u 7 months later

47
GH: 80 yr-old GH: 80 yr-old Bcc Bcc 5 stage Mohs 5 stage Mohs Tumor still present & pt not feeling well Tumor still present & pt not feeling well Pt & family decided to close & tx with radiation Pt & family decided to close & tx with radiation Defect: 3.0 x 2.4-cm closed primarily Defect: 3.0 x 2.4-cm closed primarily Later family declines radiation tx Later family declines radiation tx

48
Approx. 2 yrs later Approx. 2 yrs later Bx:Recurrent keratinizing bcc Bx:Recurrent keratinizing bcc

49
2 stage Mohs sx Defect: 3.2 x 4.0-cm

50
Closure: primary with bilateral M-plastys Closure: primary with bilateral M-plastys

51
MW: 82 yr-old MW: 82 yr-old Morpheic bcc Morpheic bcc

52
8 stage Mohs sx 8 stage Mohs sx Defect: 5.2 x 2.8-cm Defect: 5.2 x 2.8-cm

53
Bilateral cheek advancement flap Bilateral cheek advancement flap Designed to move skin from medial cheek to side of nose Designed to move skin from medial cheek to side of nose First extend incision inferiorly along meilolabial fold First extend incision inferiorly along meilolabial fold Undermine medial portion of cheek Undermine medial portion of cheek Try moving tissue (trial closure) Try moving tissue (trial closure) Next extend incision further down meilolabial fold Next extend incision further down meilolabial fold If needed create second limb: incision made tangential to upper pole of defect & within or parallel to eyelid/cheek line If needed create second limb: incision made tangential to upper pole of defect & within or parallel to eyelid/cheek line This incision may or may not need to be as long as meilolabial incision (usually can be 1/3 or ½ the length) This incision may or may not need to be as long as meilolabial incision (usually can be 1/3 or ½ the length) This frees up more cheek which is advanced medially rather than medially & superiorly This frees up more cheek which is advanced medially rather than medially & superiorly b/c undermining is carried close to eye tissue undermine at a more shallow plane/ just above oculus oris muscle b/c undermining is carried close to eye tissue undermine at a more shallow plane/ just above oculus oris muscle Warn pt surgery produces severe ecchymosis & sometimes prolonged edema of lower eyelid area Warn pt surgery produces severe ecchymosis & sometimes prolonged edema of lower eyelid area
 Try moving tissue (trial closure) Next extend incision further down meilolabial fold Next extend incision further down meilolabial fold If needed create second limb: incision made tangential to upper pole of defect & within or parallel to eyelid/cheek line If needed create second limb: incision made tangential to upper pole of defect & within or parallel to eyelid/cheek line This incision may or may not need to be as long as meilolabial incision (usually can be 1/3 or ½ the length) This incision may or may not need to be as long as meilolabial incision (usually can be 1/3 or ½ the length) This frees up more cheek which is advanced medially rather than medially & superiorly This frees up more cheek which is advanced medially rather than medially & superiorly b/c undermining is carried close to eye tissue undermine at a more shallow plane/ just above oculus oris muscle b/c undermining is carried close to eye tissue undermine at a more shallow plane/ just above oculus oris muscle Warn pt surgery produces severe ecchymosis & sometimes prolonged edema of lower eyelid area Warn pt surgery produces severe ecchymosis & sometimes prolonged edema of lower eyelid area")
55
VP: 68 yr-old VP: 68 yr-old BCC left paranasal BCC left paranasal

57
2 stage Mohs sx 2 stage Mohs sx Defect:1.2 x 1.0-cm Defect:1.2 x 1.0-cm

58
One-sided advancement flap with Burrows triangle inferior margin One-sided advancement flap with Burrows triangle inferior margin

59
7 days post-op 7 days post-op Occasionally a pucker results & a Burrows triangle or a Z-plasty is needed at the lateral extension Occasionally a pucker results & a Burrows triangle or a Z-plasty is needed at the lateral extension

60
KA: 69 yr-old KA: 69 yr-old Lentigo maligna mid-forehead Lentigo maligna mid-forehead

62
2 stage Mohs sx 2 stage Mohs sx Defect: 2.0 x 2.2-cm Defect: 2.0 x 2.2-cm Closure: primary tx with Aldara 4 days/ week QD 3 days off x 1 month Closure: primary tx with Aldara 4 days/ week QD 3 days off x 1 month

64
9 weeks later 9 weeks later

65
MG: 94 yr-old MG: 94 yr-old Recurrent BCC (infiltrative) right nasal side-wall Recurrent BCC (infiltrative) right nasal side-wall
 right nasal side-wall Recurrent BCC (infiltrative) right nasal side-wall")
67
3 stage Mohs sx with positive margins deep extending possibly to periostium 3 stage Mohs sx with positive margins deep extending possibly to periostium Defect: 3.0 x 3.0-cm Defect: 3.0 x 3.0-cm Closure: one-sided advancement flap with Borrows triangle inferiorly at right upper lip Closure: one-sided advancement flap with Borrows triangle inferiorly at right upper lip Post-op radiation tx Post-op radiation tx

75
7 days later 7 days later Temporary problem associated with advancing flaps from cheek onto nasal side-wall is that of tenting across former nasal/facial line, creating facial fullness & asymmetry Temporary problem associated with advancing flaps from cheek onto nasal side-wall is that of tenting across former nasal/facial line, creating facial fullness & asymmetry Usually the nasal/facial line reforms as flap adheres to the bed & is pulled into place Usually the nasal/facial line reforms as flap adheres to the bed & is pulled into place But on occasion a “trapdoor” appearance occurs & these need to be revised after 3-6 months But on occasion a “trapdoor” appearance occurs & these need to be revised after 3-6 months The flap is elevated & the fibrous tissue or fat is removed The flap is elevated & the fibrous tissue or fat is removed At this time buried sutures can be placed to recreate the nasal/facial line At this time buried sutures can be placed to recreate the nasal/facial line

81
One-sided Advancement Flap

84
Pt from “Atlas of Cutaneous Facial Flaps & Grafts” Pt from “Atlas of Cutaneous Facial Flaps & Grafts” Ronald L.Moy Ronald L.Moy

85
GC: 69 yr-old GC: 69 yr-old Nodular basal cell ca left alar crease Nodular basal cell ca left alar crease 1 stage Mohs sx 1 stage Mohs sx Defect: 2.0 x 1.2 cm Defect: 2.0 x 1.2 cm Perialar advancement flap Perialar advancement flap

87
Sutures removed 7 days later Sutures removed 7 days later

88
Peri-alar Advancement Flap

89
TH-47 yr old male; 3 ppd tab. TH-47 yr old male; 3 ppd tab. SCC superficial & well differentiated left helix SCC superficial & well differentiated left helix 2 stage Mohs sx 2 stage Mohs sx Defect: 2.0 x 1.5-cm Defect: 2.0 x 1.5-cm FTSG FTSG

91
Bolster removed 8 days later Bolster removed 8 days later

92
GE: 78 yr-old GE: 78 yr-old Bcc left temple Bcc left temple s/p temple artery bx bilateral inferiorly s/p temple artery bx bilateral inferiorly 3 stage Mohs 3 stage Mohs Defect: 4.2 x 3.0 cm Defect: 4.2 x 3.0 cm Closure: bilateral advancement flap with Burrows triangle anteriorly Closure: bilateral advancement flap with Burrows triangle anteriorly

94
JT: 94 yr-old JT: 94 yr-old A. SCC; B. BCC; C.AK; D. SCC in situ; E. SCC; D. SCC A. SCC; B. BCC; C.AK; D. SCC in situ; E. SCC; D. SCC

97
2 stage Mohs sx 2 stage Mohs sx Defect: 2.6 x 1cm Defect: 2.6 x 1cm Closure: primary with Burrows triangle superiorly Closure: primary with Burrows triangle superiorly H &E revealed new foci of SCC H &E revealed new foci of SCC Tx with Aldara after 6 weeks of healing Tx with Aldara after 6 weeks of healing

100
44 yr-old 44 yr-old Nodular & ulcerative BCC left lateral neck Nodular & ulcerative BCC left lateral neck Slowly growing over 20 yrs Slowly growing over 20 yrs MRI:mass extending very close to platysma muscle MRI:mass extending very close to platysma muscle 2 stage Mohs sx 2 stage Mohs sx Defect: 5.0-cm x 3.0-cm Defect: 5.0-cm x 3.0-cm Primary closure Primary closure

Similar presentations

























































 nerve block is a local anaisthisia that anesthetizes the maxillary canine, the central and lateral incisors, and.>")



 Meet Karpagam Medical College Hospital 27-02-2015.>")



