Download presentation
Presentation is loading. Please wait.

1
Coverage of Thigh Ian Maxwell

2
Gastocnemius Flap Mathes and Nahai type I muscle flap Indications – Most commonly upper third of leg defects and knee Exposed bone, tendon, metal – Can be advanced on its pedicle as a V-Y for achilles coverage – Can be used as a functional muscle free flap Lateral or medial heads can be taken

3
Mathes and Nahai muscle flap classification

4
Muscle Anatomy Origin: – Lateral head: Lateral epicondyle of femur – Medial head: Superior to medial epicondyle – Posterior to insertion of adductor magnus Insertion – Calcaneal epiphysis via achilles tendon

5
Vascular Anatomy Medial head: Medial sural artery from popliteal artery (1cm proximal to knee joint) – 4-5cm from origin of artery to muscle insertion Lateral head: Lateral Sural artery – Pedicle length of 4cm (arises more distally) Venous drainage via venae comitantes
 – 4-5cm from origin of artery to muscle insertion Lateral head: Lateral Sural artery – Pedicle length of 4cm (arises more distally) Venous drainage via venae comitantes")
7
Innervation Tibial nerve

8
Flap dissection Midcalf longitudinal or straight incision beginning a few centimeters proximal to popliteal crease Sural vein and saphenous nerve retracted laterally Medial and lateral heads dissected in popliteal fossa and continued distally to achilles tendon

11
Flap dissection Medial head is cut from Achilles tendon Dissect through loose areolar plane proximally between soleus and medial head of gastroc Dissect pedicle If necessary proximally divide origin Tunnel subcutaneously to defect

13
Lateral head More difficult Common peroneal nerve at increased risk Shorter pedicle length Sometimes necessary of medial head flap can’t reach defect

14
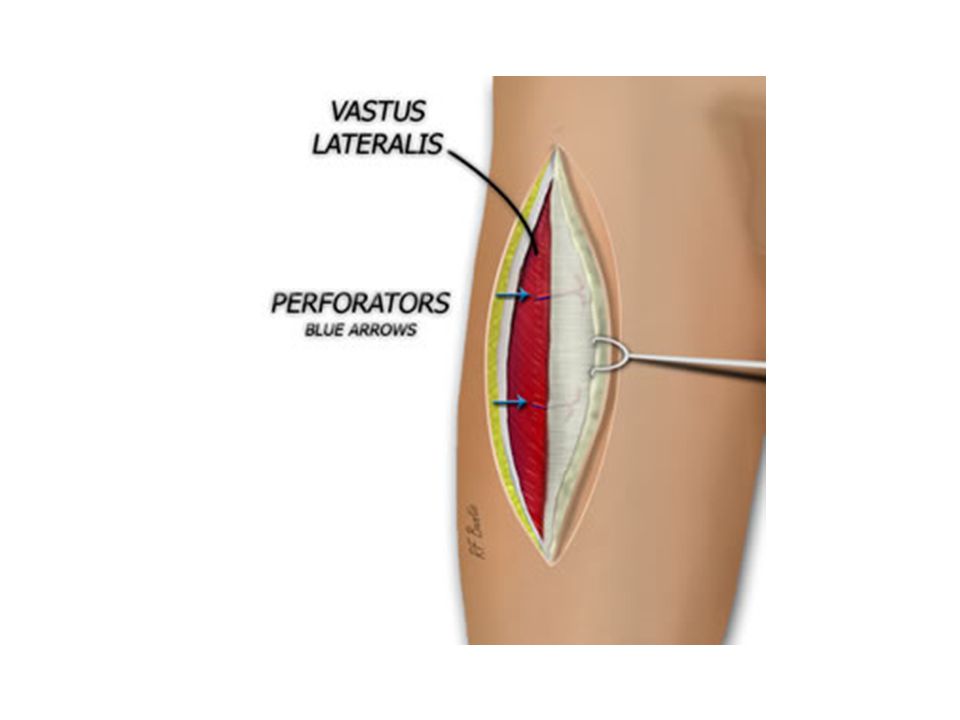
Anterolateral thigh Flap A type B and C (septocutaneous and musculocutaneous perforators) fasciocutaneous flap Useful for local or distant defect reconstruction Flap size up to 8cm X 25cm with primary closure Indications: – Free: anywhere – Local: Thin flap, large surface area wounds Groin, knee, abdomen, trochanteric region
 fasciocutaneous flap Useful for local or distant defect reconstruction Flap size up to 8cm X 25cm with primary closure Indications: – Free: anywhere – Local: Thin flap, large surface area wounds Groin, knee, abdomen, trochanteric region")
15
Arterial Supply Lateral femoral circumflex artery – Arises from lateral side of profunda femoris – Runs obliquely in septum between vastis lateralis and rectus femoris – Pedicle length is 12-16 cm For retrograde, distally based flaps can base it off of the lateral superior geniculate artery

17
Venous drainage From venae comitantes accompanying artery

18
Innervation Lateral femoral cutaneous nerve of thigh Can harvest as a sensate flap

19
Flap elevation Mark ASIS and lateral patella – This is the central axis of the flap Draw a circle of radius 3cm in the middle of the line This is where the perforators are – Doppler them Base your flap around these perforators

20
Flap dissection Dissect anteriorly first down to deep fascia Dissect subfascial anterior to posterior Vessels near or approaching the septum are preserved Dissect posterior to anterior

22
Flap dissection If vessels are perforators are all septocutaneous then elevate on these If musculocutaeous then these must be dissescted out Follow pedicle proximally and ligate if free or preserve if pedicled If bulk is needed can preserve branches to VL or RF and take muscle with the flap

23
References Microsurgeon.org Serafin, d. Atlas of microsurgical tissue transplantation Wei, Mardini. Flaps and reconstructive surgery

Similar presentations










.>")


>")










