Download presentation
Presentation is loading. Please wait.

1
Histopathology and Cytology for Breast lesions Britt-Marie Ljung MD Professor of Pathology, Dir. of Cytology University of California at San Francisco

2
Palpable Breast masses Fine needle aspiration biopsy (FNA)- cytology Core needle biopsy (CNB) - histopathology Open surgical biopsy incisional/excisional -histopathology
- cytology Core needle biopsy (CNB) - histopathology Open surgical biopsy incisional/excisional -histopathology")
3
FNA biopsy Sampling with 22-25 gauge needle Clinic procedure Immediate check of sample for adequacy and preliminary diagnosis 2-4 samples depending on size of mass, nature and abundance of material Local anesthetic optional Post procedure pain minimal Processing time for permanent material <1 hour

4
FNA biopsy Preliminary dx within minutes possible Cell block material can be used for hormone receptor evaluation Nuclear grading only Cannot prove invasive component based on FNA alone (5%)
")
9
Core needle biopsy 11-18 gauge needles Clinic procedure 5 to about 15 cores Local anesthetic necessary Post procedure pain can be significant Processing time for permanent specimen 24+ hours

10
Core needle biopsy Grading estimate possible, but limited sample, may change after excision No surgical margins Size of lesion not reliable Most cases containing invasive disease will show on core (70+%) depending on number of cores Immediate preliminary dx can be done using touch preparations
 depending on number of cores Immediate preliminary dx can be done using touch preparations")
12
Open surgical biopsy Requires operating room facility Local or general anesthesia necessary Immediate evaluation possible by frozen section or touch/scrape preparation Processing time of permanent sections 2+ days Invasive component verifyable in virtually all cases Post op discomfort significant in all cases

13
Open surgical biopsy/excision surgical margins Size of lesion if excisional bx Comprehensive view of DCIS vs invasive disease Final grading Removal of mass if excisional bx

22
Accuracy issues in common for all modalities Specimen handling including fixation and staining Skills in interpretation Sampling errors, varying degrees

28
FNAB Accuracy Palpable Breast, Meta-analysis Sensitivity65% - 98% Specificity34% - 100% Giard R and Herman SJ Cancer Apr 15, 1992 Vol 69, No 8, p. 2104

29
FNAB Accuracy – Impact of Training in Sampling Technique Sensitivity Specificity With Training 98%100% Without Training 75% 100% Definition of training in sampling technique: > 100 cases during up to one year supervised by experienced teacher with proven track record. Ljung et al Cancer (Cancer Cytopathology) 2001; 93: 23-268
 2001; 93:")
30
Impact of training in FNA procurement Formally TrainedNo Formal Training Missed CancersMissed Cancers 2% 25% Non dx Non dx 2% 37% Ljung et al Cancer 2001:93 (4):263-68
:263-68")
31
Impact of training in FNA procurement Formally trained operators did on average more FNAs Operators without formal training who did many FNAs did NOT perform better than operators without training who did few FNAs Conclusion: Experience without training did not improve performance

32
Factors improving FNA accuracy Hands-on one-to-one training in sampling technique Frequent use of the technique (>100/y) Immediate evaluation and use of direct smears Sampling and interpretation by same person Interpret FNA in clinical context (Triple test, breast) US guidance for small and non-palpable targets
 Immediate evaluation and use of direct smears Sampling and interpretation by same person Interpret FNA in clinical context (Triple test, breast) US guidance for small and non-palpable targets")
33
Levels of training, FNA sampling See one, do one, teach one ~ 50% dx 10 cases in training ~ 60% dx 50 cases in training ~ 85% dx 100 cases in training ~ 90% dx 200 cases in training ~ 95% dx

34
Accuracy Breast Core biopsies, meta-analysis Guided by: False Negative Palpation0 – 13% Ultrasound 0 - 12% Stereotactic 0.2 – 8.9% Dillon M et al Annals of Surgery Vol 242 No. 5 Nov 2005

35
Image Guided Core Needle Biopsy Accuracy Strategy: Increase number of cores/weight of tissue Sensitivity Recommended with 5 no of cores 14 gauge cores 14 gauge Mass Lesions98% 5-6 Ca++91% 15 Arch. Dist86% 15 US-guided98% 5-12 cores Operator dependent Brenner RJ et al AJR Am J Roentgenol 166:341-346 1996

36
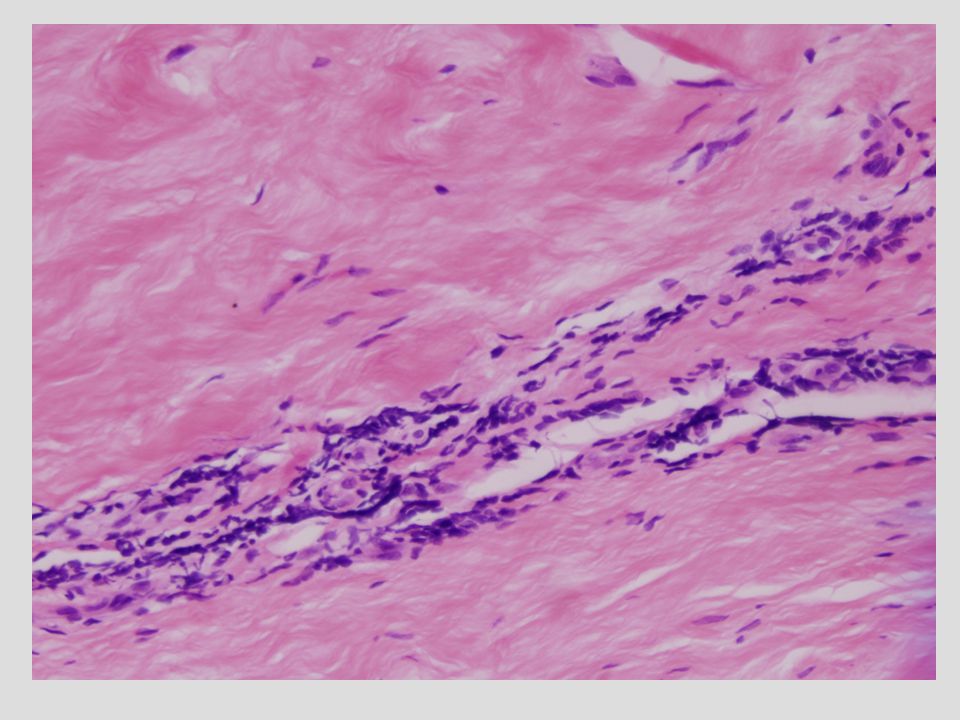
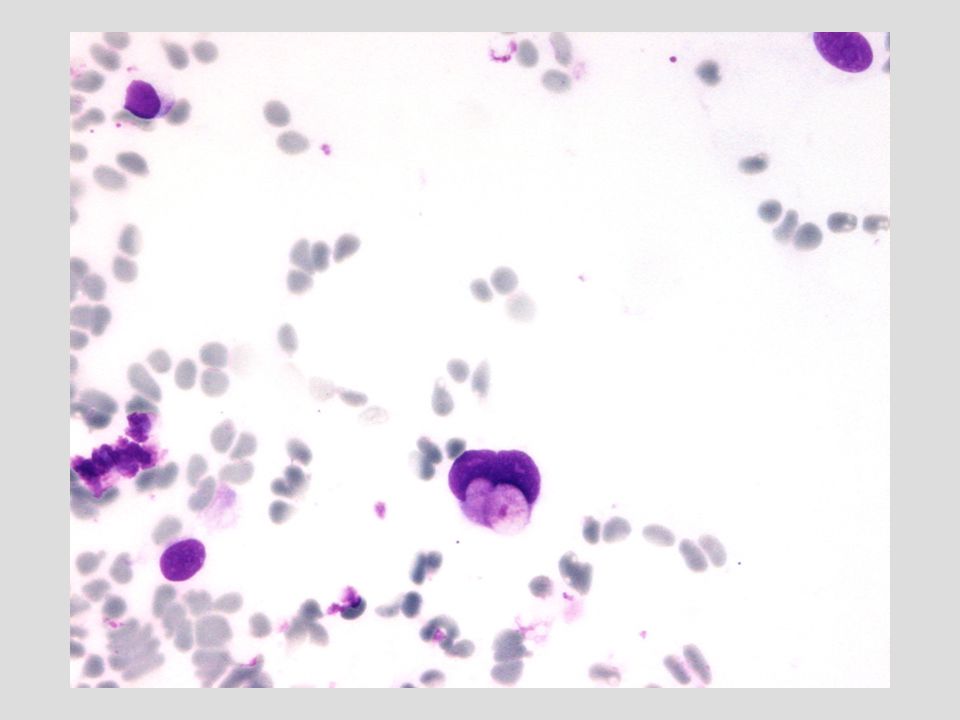
Accuracy Open biopsy Sampling problems are rare but not zero particularly for small lesions and lesions found by imaging Interpretation issues most common in lobular carcinoma with sparse and very small tumor cells that can mimmick lymphocytes

37
FNAB as part of Triple Test in palpable lesions Reported False neg rate FNAB alone 7% When applying Triple Test for Breast (clinical+imaging+cytology findings) False negative rate 0% Conclusion: if the bx result does not fit, regardless of bx type, take additional steps Lau S et al The Breast Journal Vol 10 No 6 2004 p. 487-491
Similar presentations






















 of Breast Cancer Lesions Alissa Garman Janie Goldsworthy Kristi Hinner Nick Kortan Client: Elizabeth Burnside.>")












