Download presentation
Presentation is loading. Please wait.

1
Dr.Suresh Babu Chaduvula Professor Dept. of OBGyn, College of Medicine, KKU, Abha, KSA

2
1] Abortion 2] Ectopic Pregnancy 3] Hydatidiform mole 4] Implantation bleeding 5] Local causes – Erosion, Polyp, Varicose veins rupture, Cervical malignancy
![ 1] Abortion 2] Ectopic Pregnancy 3] Hydatidiform mole 4] Implantation bleeding 5] Local causes – Erosion, Polyp, Varicose veins rupture, Cervical malignancy](http://images.slideplayer.com/13/3846058/slides/slide_2.jpg " 1] Abortion 2] Ectopic Pregnancy 3] Hydatidiform mole 4] Implantation bleeding 5] Local causes – Erosion, Polyp, Varicose veins rupture, Cervical malignancy")
3
Definition: Termination of pregnancy before the period of viability or fetus weighing less than 500 grams. Expulsion or Extraction of an embryo or fetus before viability Period of viability: Developing countries – 28 weeks. UK, USA – Less than 22 to 24 weeks

4
10 – 20% 75 % occur before 16 th week 75 % occur at 8 th week

5
1] Spontaneous 2] Threatened 3] Inevitable 4] Incomplete 5] Complete 6] Missed 7] Septic 8] Recurrent 9] Induced – Legal or Illegal [ Criminal ]
![ 1] Spontaneous 2] Threatened 3] Inevitable 4] Incomplete 5] Complete 6] Missed 7] Septic 8] Recurrent 9] Induced – Legal or Illegal [ Criminal ]](http://images.slideplayer.com/13/3846058/slides/slide_5.jpg " 1] Spontaneous 2] Threatened 3] Inevitable 4] Incomplete 5] Complete 6] Missed 7] Septic 8] Recurrent 9] Induced – Legal or Illegal [ Criminal ]")
6
1] Genetic factors – Chromosomal abnormalities – Autosomal trisomy – 50 % - Trisomy 16 is common Polyploidy – 20 % - Presence of extra haploid number of chromosomes – 69 or 92 chromosomes – Triploidy is common Chromosomal rearrangements – Inversion, deletion, translocation Others - Mosaic
![ 1] Genetic factors – Chromosomal abnormalities – Autosomal trisomy – 50 % - Trisomy 16 is common Polyploidy – 20 % - Presence of extra haploid number of chromosomes – 69 or 92 chromosomes – Triploidy is common Chromosomal rearrangements – Inversion, deletion, translocation Others - Mosaic](http://images.slideplayer.com/13/3846058/slides/slide_6.jpg " 1] Genetic factors – Chromosomal abnormalities – Autosomal trisomy – 50 % - Trisomy 16 is common Polyploidy – 20 % - Presence of extra haploid number of chromosomes – 69 or 92 chromosomes – Triploidy is common Chromosomal rearrangements – Inversion, deletion, translocation Others - Mosaic")
7
2] Endocrine factors: Luteal Phase defect Deficient Progesterone Hyper & Hypothyroidism Uncontrolled Diabetes Mellitus
![ 2] Endocrine factors: Luteal Phase defect Deficient Progesterone Hyper & Hypothyroidism Uncontrolled Diabetes Mellitus](http://images.slideplayer.com/13/3846058/slides/slide_7.jpg " 2] Endocrine factors: Luteal Phase defect Deficient Progesterone Hyper & Hypothyroidism Uncontrolled Diabetes Mellitus")
8
3] Uterine Anomalies: Cervical incompetence Bocornuate uterus Septate uterus 4] Sub-mucus Fibroid: 5] Intra-uterine synechiae: [ Asherman’s syndrome ]
![ 3] Uterine Anomalies: Cervical incompetence Bocornuate uterus Septate uterus 4] Sub-mucus Fibroid: 5] Intra-uterine synechiae: [ Asherman’s syndrome ]](http://images.slideplayer.com/13/3846058/slides/slide_8.jpg " 3] Uterine Anomalies: Cervical incompetence Bocornuate uterus Septate uterus 4] Sub-mucus Fibroid: 5] Intra-uterine synechiae: [ Asherman’s syndrome ]")
9
6] Infections: Viral – Rubella, Cytomegalo, varicella, variola Parasitic: Toxoplasmosis, Malaria Bacterial: Chlamydia, Ureaplasma, Brucella Spirochetes: Treponema pallidum
![ 6] Infections: Viral – Rubella, Cytomegalo, varicella, variola Parasitic: Toxoplasmosis, Malaria Bacterial: Chlamydia, Ureaplasma, Brucella Spirochetes: Treponema pallidum](http://images.slideplayer.com/13/3846058/slides/slide_9.jpg " 6] Infections: Viral – Rubella, Cytomegalo, varicella, variola Parasitic: Toxoplasmosis, Malaria Bacterial: Chlamydia, Ureaplasma, Brucella Spirochetes: Treponema pallidum")
10
7]Immunological disorders: Antinuclear Antibodies Anti phospholipid antibodies like Lupus anticoagulant and Anti cardiolipin antibodies
![ 7]Immunological disorders: Antinuclear Antibodies Anti phospholipid antibodies like Lupus anticoagulant and Anti cardiolipin antibodies](http://images.slideplayer.com/13/3846058/slides/slide_10.jpg " 7]Immunological disorders: Antinuclear Antibodies Anti phospholipid antibodies like Lupus anticoagulant and Anti cardiolipin antibodies")
11
8] Medical Disorders: Cyanotic heart diseases Hemoglobonopathies 9] Paternal Factors: Sperm chromosomal anomaly 10] Inherited Thrombophilia 11] Environmental - Smoking, Radiation, Teratogenic drugs, chemicals, Alcohol 12] Unexplained – 40- 60%
![ 8] Medical Disorders: Cyanotic heart diseases Hemoglobonopathies 9] Paternal Factors: Sperm chromosomal anomaly 10] Inherited Thrombophilia 11] Environmental - Smoking, Radiation, Teratogenic drugs, chemicals, Alcohol 12] Unexplained – %](http://images.slideplayer.com/13/3846058/slides/slide_11.jpg " 8] Medical Disorders: Cyanotic heart diseases Hemoglobonopathies 9] Paternal Factors: Sperm chromosomal anomaly 10] Inherited Thrombophilia 11] Environmental - Smoking, Radiation, Teratogenic drugs, chemicals, Alcohol 12] Unexplained – %")
12
1] Genetic 2] Endocrine disorders 3] Immunological disorders 4] Infections 5] Unexplained
![ 1] Genetic 2] Endocrine disorders 3] Immunological disorders 4] Infections 5] Unexplained](http://images.slideplayer.com/13/3846058/slides/slide_12.jpg " 1] Genetic 2] Endocrine disorders 3] Immunological disorders 4] Infections 5] Unexplained")
13
1] Cervical Incompetence 2] Bicornuate uterus 3] Septate uterus 4] Uterine synechiae 5] Submucus fibroid 6] Maternal Diseases 7] Unexplained
![ 1] Cervical Incompetence 2] Bicornuate uterus 3] Septate uterus 4] Uterine synechiae 5] Submucus fibroid 6] Maternal Diseases 7] Unexplained](http://images.slideplayer.com/13/3846058/slides/slide_13.jpg " 1] Cervical Incompetence 2] Bicornuate uterus 3] Septate uterus 4] Uterine synechiae 5] Submucus fibroid 6] Maternal Diseases 7] Unexplained")
14
Clinical features: Vaginal bleeding Mild lower abdominal pain Vitals stable Vaginal examination – Cervix is closed and uterus size will correspond to pregnancy Diagnosis – CBC, Ultrasound, Serum Progesterone and Serum HCG levels Treatment – Rest, sedation and synthetic progesterone and HCG injections?

15
Clinical features: Vaginal Bleeding with passage of products of gestation Pain lower abdomen Vitals - disturbed according to the blood loss Vaginal examination: Cervix is dilated with hanging of fetal products and uterus size will be lesser than amenorrhea Diagnosis - Ultrasound Treatment – Stabilize vitals and Suction evacuation / curettage After 12 weeks – Under GA and IV oxytocin drip products are removed by ovum forceps / Curettage

16
Clinical features: Vaginal Bleeding with passage of products of gestation Pain may be less or absent Vitals - disturbed according to the blood loss Vaginal examination: Cervix is closed and uterus size is lesser than amenorrhea Diagnosis - Ultrasound Treatment – No active intervention

17
Clinical features: Vaginal Bleeding Pain lower abdomen Vitals - disturbed according to the blood loss Vaginal examination: Cervix is dilated with hanging of fetal products and uterus size will correspond to amenorrhea Diagnosis - Ultrasound Treatment – Stabilize vitals and Suction evacuation / curettage After 12 weeks – IV oxytocin drip

18
Fetus is dead and retained for variable period [ 4 – 6 weeks ] Clinical Features: Brownish vaginal dischage Subsidence of pregnancy symptoms Retrogression of breast changes Vaginal examination: Uterus will be less than amenorrhea and cervix is closed Diagnosis – Ultrasound
![ Fetus is dead and retained for variable period [ 4 – 6 weeks ] Clinical Features: Brownish vaginal dischage Subsidence of pregnancy symptoms Retrogression of breast changes Vaginal examination: Uterus will be less than amenorrhea and cervix is closed Diagnosis – Ultrasound](http://images.slideplayer.com/13/3846058/slides/slide_18.jpg " Fetus is dead and retained for variable period [ 4 – 6 weeks ] Clinical Features: Brownish vaginal dischage Subsidence of pregnancy symptoms Retrogression of breast changes Vaginal examination: Uterus will be less than amenorrhea and cervix is closed Diagnosis – Ultrasound")
19
Complications: Disseminated intravascular Coagulation Coagulation Profile is essential Treatment: Dialatation and Curettage – less than 12 weeks After 12 weeks – IV Oxytocin drip / Prostaglandin vaginal pessaries or Gel / IM injections of PG F2 alfa.

20
Any abortion associated with evidence of infection in the uterus and its contents Clinical features: Temperature – 100.4 degree F for 24 hrs or more Offensive or purulent vaginal discharge Lower abdominal pain and tenderness This is mostly due to incomplete and illegal abortions or also following spontaneus abortion

21
Peritonitis features may be present Vaginal examination – cervix may be closed or dilated, pus like offensive discharge Tender uterus and size of uterus will be lesser than amenorrhea Organisms responsible for sepsis: E.coli, Klebsiella, Staph.aureus, Clostridium welchi and perfringens etc., Complications - Endotoxemic shock, acute renal failure, DIC, Peritonitis and Gas gangrene

22
Investigations: Endo cervical swab for culture & sensitivity High vaginal swab for culture & Sensitivity CBC DIC profile if required Blood culture Urine Culture Ultrasound

23
Treatment: IV Antibiotics – for aerobic, anaerobic organisms – IV Ampicillin, Gentamycina and Metronidazole Anti Gas Gangrene serum Treatment of complications Surgery – Evacuation of uterus and Laparotomy if necessary depending on peritonitis features

24
Development of gestational sac without any evidence of fetus or fetal parts Diagnosis – Ultrasound Treatment – Dilatation and Curettage Tissue should be sent for Fetal karyotyping

25
A sequence of three or more consecutive abortions before 20 weeks Incidence – 1 % Causes: First Trimester – Genetic, Endocrine and Metabolic, Infection, Inherited thrombophilia, Immunological and unexplained Second Trimester – Bicornuate uterus, Unicornuate uterus, septate uterus, Cervical incompetence.

30
Cervix is unable to with hold the fetus faulty defect in the sphincteric mechanism. Retentive power of cervix is impaired Causes: Congenital Iatrogenic – Dilatation and Curettage, Amputation of the cervix, cone biopsy Clinical features: History of recurrent mid trimester abortions where leaking followed by painless expulsion of fetus

32
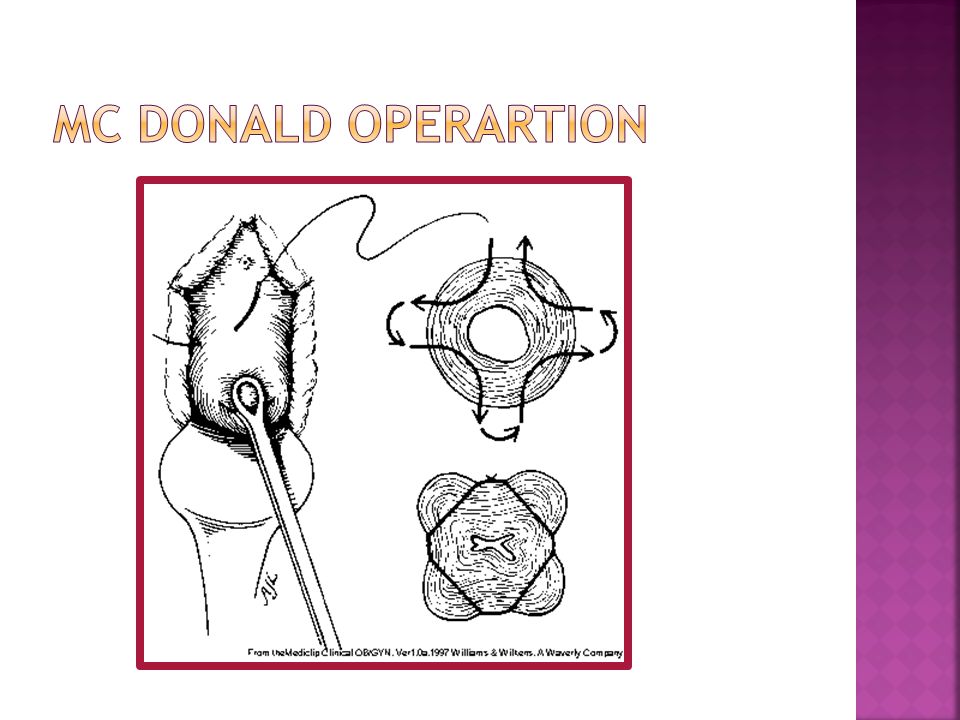
Diagnosis: Ultrasound – Cervical length less than 2.5 cm and cervical dilatation more than 1.5 cm with funneling of cervix and bulging of membranes Periodic per speculum examination Treatment: Cervical Circlage with Merseline tape at 16 – 18 weeks – Mc Donald operation Shiridkar’s operation

34
Medical Termination of Pregnancy Indications: Failure of contraception Rape Medical diseases that may deteriorate mother’s health Congenital anomalies

35
First Trimester Surgical : Manual Vacuum Aspiration Dilatation and Curettage Suction and Evacuation Medical: Prostaglandin preparations Mifepristone Misoprostol

36
Second Trimester: Intraamnitic instillation of PGF2 alfa or Hypertonic saline Extraamniotic ethacrydine lactate or PGf2 alfa Oxytocin Infusion Hysterotomy

Similar presentations
















 expulsion of the products of conception from the uterus before 20 weeks gestation At least.>")







