Download presentation
Presentation is loading. Please wait.

1
Marilene B. Wang, MD, FACS Professor UCLA Division of Head Neck Surgery Chief of Otolaryngology VA Greater Los Angeles Healthcare System

4
From Anterior Nasal Spine ◦ To Sphenoid Ostium7 cm ◦ To Pituitary Fossa8.5 cm

5
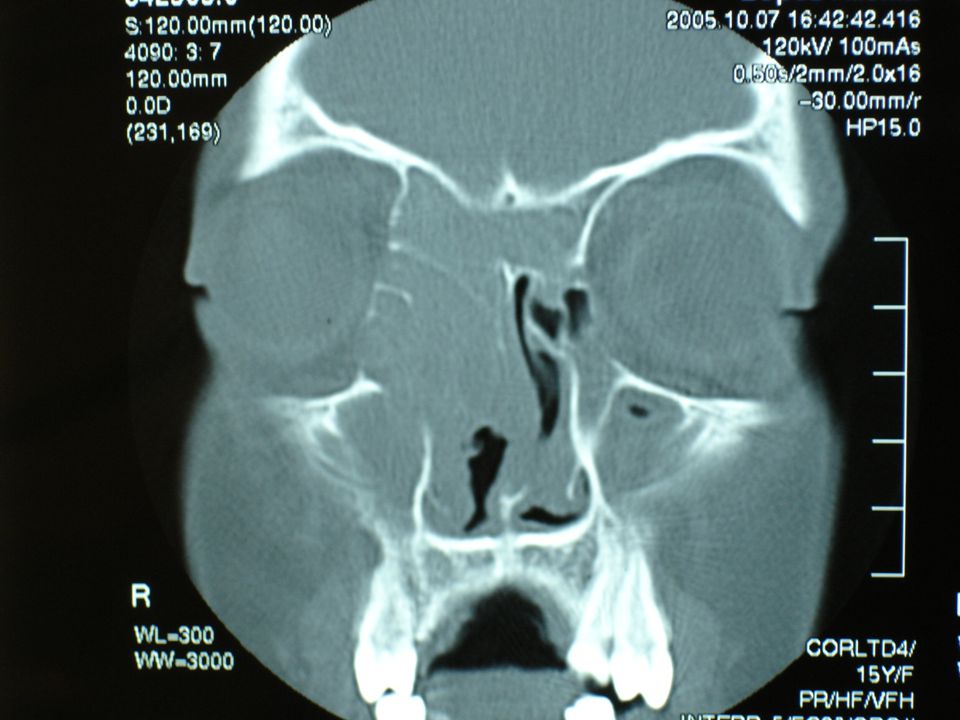
Middle turbinate Lamina papyracea Ethmoid fovea Cribriform plate Sphenoid

6
Facial pain/pressure Nasal obstruction/blockage Nasal discharge/purulence/discolo red postnasal drip

7
Hyposmia/anosmia Purulence in nasal cavity on examination Fever (acute rhinosinusitis only)
")
8
Headache Fever Halitosis Fatigue

9
Dental pain Cough Ear pain/pressure/fullness

10
Acute Subacute Chronic Recurrent, acute Acute exacerbations of chronic

11
Duration up to 4 weeks > 2 major factors 1 major factor + 2 minor factors Nasal purulence on exam

12
Duration 4-12 weeks >2 major factors 1 major factor + 2 minor factors, or nasal purulence on exam Complete resolution after effective medical therapy

13
Duration > 12 weeks History same as for subacute Facial pain does not constitute suggestive history in absence of other nasal symptoms or signs

14
>4 episodes/year + each episode last >7-10 days. Absence of intervening signs of chronic rhinosinusitis

15
Sudden worsening of chronic rhinosinusitis Return to baseline after treatment

16
Allergies Immunodeficiency Genetic/congenital

17
Endocrine Neuromechanism

18
Anatomic Neoplastic Acquired mucociliary dysfunction

19
Microorganisms—viral, bacterial, fungal Noxious chemicals, pollutants, smoke Medications Trauma Surgery

20
S. pneum (20-43%) H. influenzae (22-35%) Strep spp. (3-9%) Anaerobes (0-9%) M. catarrhalis (2-10%) S. aureus (0-8%) Other (4%)
 Anaerobes (0-9%) M. catarrhalis (2-10%) S. aureus (0-8%) Other (4%).")
21
S. pneum (25-30%) H. influenzae (15-20%) M. catarrhalis (15-20%) S. pyogenes (2-5%) Anaerobes (2-5%) Sterile (20-35%)
 S. pyogenes (2-5%) Anaerobes (2-5%) Sterile (20-35%).")
22
Mild disease with no recent antimicrobial use Augmentin, Amoxicillin Vantin Ceclor Omnicef

23
Tequin, Levaquin, Avelox Augmentin Combination (Amox or clinda + Suprax)
")
24
Bactrim Doxycycline Zithromax, Biaxin, Erythromycin Switch to quinolone if no improvement in 72 hours

25
Quinolone Augmentin Clindamcin + rifampin Consider IV abx

26
Augmentin, Amoxicillin Vantin Ceclor Omnicef Switch if no improvement after 72 hours

27
Bactrim Macrolide

28
Augmentin Rocephin Bactrim, macrolide Consider IV abx if no improvement

29
Afrin for 3 days Normal saline sprays Decongestants Antihistamines ?Steroids

30
Periorbital cellulitis Preseptal cellulitis/abscess Orbital cellulitis Orbital abscess Cavernous sinus thrombosis

31
Widespread affliction—the most common allergic disease Affects 10-30% of American adults— >20 million people, adults and children Results in missed work and school days, poor quality of life

32
Allergic salute Shiners Itchy, red conjunctiva Sneezing Post-nasal drip, rhinorrhea, congestion

33
Dust Mold, mildew Plants Animal dander Feathers/down

34
Pollen Smog Trees, grasses, weeds Dust, fertilizer, chemicals

35
Asthma Allergic fungal sinusitis Cystic fibrosis Mucociliary dysfunction Connective tissue disorders (Wegener’s granulomatosis, sarcoid)
")
36
Nasal polyposis Samter’s triad (aspirin sensitivity, nasal polyps, asthma) Cocaine use
 Cocaine use")
37
Antibiotics Antihistamines Nasal steroids Normal saline irrigations Allergy evaluation +/- immunotherapy

38
Sinus CT scan Consider anatomic factors— septal deviation, nasal polyps, concha bullosa, ostio-meatal blockage

39
Nasal polyposis Anatomic blockage—deviated septum, enlarged turbinate, concha bullosa Mucocele Orbital abscess

40
Fungal sinusitis—allergic vs. invasive (mucor) Tumor of nasal cavity or sinus
 Tumor of nasal cavity or sinus")
41
Chronic, recurrent sinusitis Failure to respond to maximal medical therapy Obtain cultures

42
Nasal congestion Headache/sinus pain Fatigue Prolonged bleeding/crusting

43
Breach of lamina papyracea— damage to extraocular muscles, periorbital ecchymoses Damage to optic nerve— blindness Breach of cribriform—CSF leak Meningitis

44
May be a lifelong disease Allergy control— antiihistamines, nasal steroids, immunotherapy Oral steroids—judiciously Antibiotics for acute exacerbations

45
Environmental control—avoid carpet, damp, mold, older homes, smog Saline irrigations

46
Alternative therapies— acupuncture, stress management, herbal remedies Pain management Multi-disciplinary effort—work with allergy, infectious disease, neurology/pain management services

47
4 types of allergic reactions (Gell and Coombs) Type 1 – IgE Type 2 - IgG--antigen Type 3 – Immune complex Type 4 – Delayed hypersensitivity
 Type 1 – IgE Type 2 - IgG--antigen Type 3 – Immune complex Type 4 – Delayed hypersensitivity")
48
Mast cells bind IgE via their Fc(ε) receptors Mast cell degranulates and releases mediators--produce allergic reactions Hypersensitivity usually appears on repeated contact with the allergen. Examples of type I allergic reactions – Anaphylaxis, atopic asthma, atopic eczema, drug allergy, hay fever

49
Antibody (IgG or IgM) directed against antigen on an individual's own cells, or against foreign antibody (after blood transfusion) Cytotoxic action by killer cells, or to lysis mediated by the complement system. – Autoimmune hemolytic anemia, Goodpasture's syndrome, hemolytic disese of the newborn, myasthenia gravis, pemphigus

50
Immune complexes (antigen and usually IgG or IgM) deposited in the tissue Complement is activated and polymorphonuclear cells are attracted, causing local tissue damage and inflammation. – Polyarteritis nodosa, post-streptococcal glomerulonephritis, systemic lupus erythematosus

51
T cells, sensitized to antigen, release lymphokines following secondary contact with the antigen Cytokines induce an inflammatory response, activate and attract macrophages, release inflammatory mediators. Antibodies produced against fixed cellular or tissue antigens are usually autoantibodies – Crohn's disease, leprosy, tuberculosis, sarcoidosis, schistosomiasis

52
Parents with allergy greater likelihood of producing allergic children Food allergies Environment— air pollution Smoking

53
History—environmental exposure, smoking, seasonal occurrence, pets, foods Examination ◦ Allergic shiners ◦ Allergic salute ◦ Supratip crease ◦ Dennie’s lines (skin fold under eyes) ◦ Adenoid facies
 ◦ Adenoid facies")
54
Skin testing ◦ Prick/puncture (scratch or patch) ◦ Intradermal ◦ Dilutional intradermal (skin end-point titration-SET) In vitro testing ◦ RAST (radioactive marker) ◦ ELISA (enzymatic marker)
 ◦ Intradermal ◦ Dilutional intradermal (skin end-point titration-SET) In vitro testing ◦ RAST (radioactive marker) ◦ ELISA (enzymatic marker)")
55
Prick—few drops of purified allergen pricked onto skin surface (dust, dander, pollen) Patch—large patch with different allergens (latex, medications, metal, fragrances, preservatives) Histamine or glycerin used as positive controls
 Patch—large patch with different allergens (latex, medications, metal, fragrances, preservatives) Histamine or glycerin used as positive controls")
56
Intradermal injection of allergens at increasing concentrations to measure allergic response Start with a very dilute solution If 2mm of growth noted, then second injection at a higher concentration is given to confirm the response End point is concentration of antigen that causes an increase in the size of the wheal followed by confirmatory whealing Stop at 13 mm

57
Avoid medications which may interfere ◦ Antihistamines ◦ Antidepressants ◦ Antacids

58
Anaphylaxis ◦ Low-grade fever ◦ Lightheadedness or dizziness ◦ Wheezing or Shortness of breath ◦ Extensive skin rash ◦ Swelling of face, lips or mouth ◦ Difficulty swallowing or speaking

59
RAST -radioallergosorbent test—detect specific IgE antibodies to allergens Improved sensitivity without loss of specificity Excellent reproducibility across the full measuring range of the calibration curve Not always necessary to remove patient from an anthihistamine medication regimen If skin conditions (such as eczema) are so widespread that allergy skin testing can not be done
 are so widespread that allergy skin testing can not be done")
60
ELISA – enzyme linked immunosorbent assay Used more for food allergies Not as sensitive as skin tests

61
Environmental control ◦ Stop smoking, clean house, avoid mold, indoor plants, pets, HEPA filter Pharmacotherapy ◦ Antihistamines, anti-leukotrienes, mast-cell stabilizers, topical and systemic steroids

62
Specific allergens Vial test ◦ Intradermal test ◦ Smallest measurable dose Once or twice weekly injections Dose escalated Continue treatment 3-5 years

63
Invasive ◦ Acute fulminant ◦ Chronic invasive ◦ Granulomatous invasive

64
Noninvasive ◦ Saprophytic fungal infestation ◦ Fungal ball, “mycetoma” ◦ Allergic fungal rhinosinusitis

65
Corollary to allergic bronchopulmonary aspergillosis (ABPA) AFRS cycle ◦ Immune and eosinophilic response to protein components of fungi ◦ Sinonasal inflammation, viscid allergic fungal mucin, obstruction, stasis
 AFRS cycle ◦ Immune and eosinophilic response to protein components of fungi ◦ Sinonasal inflammation, viscid allergic fungal mucin, obstruction, stasis")
66
Bony remodeling Inflammatory mediators ◦ Major basic protein ◦ Eosinophilic peroxidase ◦ Tumor necrosis factor ◦ Interleukins ◦ Interferons

67
Evidence of Type I hypersensitivity (IgE mediated) Nasal polyposis Characteristic CT findings Eosinophilic mucous Positive fungal smear Kuhn and Javer: Otolaryngol Clin North Am 2000,33:2;419-432
 Nasal polyposis Characteristic CT findings Eosinophilic mucous Positive fungal smear Kuhn and Javer: Otolaryngol Clin North Am 2000,33:2;")
68
Asthma Unilateral predominance Radiographic bone erosion Fungal culture Charcot-Leyden crystals Serum eosinophilia Kuhn and Javer: Otolaryngol Clin North Am 2000,33:2;419-432

69
Not all 5 criteria for diagnosis Gradual nasal airway obstruction Thick nasal mucous/crusts May take years to manifest AFS-like syndrome

70
Immunocompetent Normal ESR, WBC Atopic ◦ Asthma, hay fever, inhalant allergy Nasal polyposis

71
Hyperactive allergic inflammatory response Possible fungal toxin Inflammatory mediators Recurrent bacterial sinusitis

72
Role of IgE Not consistently elevated in serum Local IgE-mediated immune response in nasal mucosa IgE as cause of inflammation or merely a marker

73
Allergic response to fungus by skin testing and in vitro (radioallergosorbent) methodology Variable culture results (64-100%) from sinus contents
 methodology Variable culture results (64-100%) from sinus contents")
74
Allergic fungal mucin ◦ Sheets of eosinophils ◦ Charcot-Leyden crystals ◦ Extramucosal fungal elements

76
CT ◦ Unilateral or asymmetric ◦ Sinuses Expanded--Bony attenuation or erosion ◦ Displacement of adjacent structures ◦ Signal heterogeneity Manning S et al. Laryngoscope 1997;107:170-176

79
MRI-T1 weighted ◦ Variable signal intensity in involved sinuses ◦ Signal void at periphery (mucosal edema) MRI-T2 weighted Hypointensity of signal in sinus (dehydrated allergic fungal mucin) Enhancement of periphery of sinus (mucosal edema)
 MRI-T2 weighted Hypointensity of signal in sinus (dehydrated allergic fungal mucin) Enhancement of periphery of sinus (mucosal edema)")
83
Medical Surgical Break the Allergic Fungal Rhinosinusitis Cycle

84
Functional endoscopic sinus surgery Complete ventilation of the sinuses Wide maxillary antrostomies Complete ethmoidectomies Sphenoid sinusotomies Frontal sinusotomies

85
Complete removal of allergic fungal mucin and fungal debris Mucosal sparing Save middle turbinate Frontal sinus obliteration not advised

86
PREOPERATIVE REGIMEN ◦ Antibiotics ◦ Steroids

87
POSTOPERATIVE REGIMEN ◦ Steroid taper ◦ Intranasal steroids ◦ Antibiotics ◦ Clinic endoscopy and debridement

88
Long-term systemic steroids ◦ Effective ◦ Multiple potential complications ◦ Screen for DM, cataracts, glaucoma, + PPD, active hepatitis

89
Systemic antifungal agents Amphotericin B, itraconazole, voriconazole Mixed results Expensive Hepatotoxic Need regular evaluation of liver function tests

90
83 patients managed with ESS, itraconazole, low dose oral steroids, topical steroids 36,000 doses of itraconazole—no adverse effects Reoperation required in only 20% Rains et al. AJR 2003;17:1-8

91
Intranasal Amphotericin irrigation—chronic rhinosinusitis patients Ponikau et al. J Allergy Clin Immunol 2002:110:862-866 Reduced mucosal inflammation on CT scan Improvement in symptoms and endoscopic staging in 75% Ricchetti et al. J Laryngol Otol 2002;116:261-263 Disappearance of polyps in 62% of mild and 42% of moderate chronic rhinosinusitis

92
Beneficial ◦ Mabry, Marple et al. (1997 and 1998) ◦ Prospective study, immunotherapy after surgery, patients improved, did not require systemic steroids, recurrences decreased ◦ Retrospective study, 11 patients matched with controls, immunotherapy patients had improved quality of life and objective endoscopic measures of mucosal edema
 ◦ Prospective study, immunotherapy after surgery, patients improved, did not require systemic steroids, recurrences decreased ◦ Retrospective study, 11 patients matched with controls, immunotherapy patients had improved quality of life and objective endoscopic measures of mucosal edema.")
93
Both fungal and nonfungal antigens, administered in separate vials Weekly immunotherapy, dosage advancement as tolerated Include wide variety of mold antigens Continue for 3-5 years Regular endoscopy and cleaning

94
Caveats Ferguson (1993) reported patients who received immunotherapy prior to surgery had worsening of symptoms-ongoing antigenic load local reactions, immune complex deposits Patients who received immunotherapy after surgery improved Caution with concomitant ABPA, unable to surgically remove fungi in lower respiratory tract
 reported patients who received immunotherapy prior to surgery had worsening of symptoms-ongoing antigenic load local reactions, immune complex deposits Patients who received immunotherapy after surgery improved Caution with concomitant ABPA, unable to surgically remove fungi in lower respiratory tract")
95
Recurrence of disease common Surgical treatment mandatory Multidisciplinary management ◦ Steroids, antifungals—systemic vs. topical ◦ Immunotherapy

96
Better control with prolonged postoperative medical therapy Probably immunological disease, not infectious Therapy evolving as understanding of disease process improves Prolonged, close follow-up needed

Similar presentations