Download presentation
Presentation is loading. Please wait.

1
Hypertension arterielle Cours de DCEM Rabih R. Azar, MD, MSc, FACC Division of Cardiology Hotel-Dieu de France Hospital

2
Morbidity and mortality rates according to blood pressure level

4
Hypertensive Patients Are at Increased Risk for Cardiovascular Events Framingham Heart Study - Risk of Cardiovascular Events by Hypertensive Status in Patients Aged 35-64 Years; 36-Year Follow-Up Risk Ratio2.02.2 3.8 2.6 2.0 3.7 4.0 3.0 Excess Risk 22.711.8 9.1 3.8 4.9 5.3 10.4 4.2 Coronary DiseaseStroke Peripheral Artery Disease Cardiac Failure Biennial Age-Adjusted Rate per 1000 Kannel WB JAMA 1996;275(24):1571-1576.
:")
5
Cumulative Number of Endpoints* *Including deaths, thrombotic or hemorrhagic cerebrovascular disease, myocardial infarction, and renal failure The Management Committee Lancet 1980;1:1261-1267 Effect of Hypertensive Treatment in Mild Hypertension Placebo (n=1706) Treatment (n=1721) Total (fatal and non-fatal) endpoints All fatal endpoints Days in trial 130 120 110 100 90 80 70 60 50 40 30 20 10 0 400 800 1200 1600 2000
 Treatment (n=1721) Total (fatal and non-fatal) endpoints All fatal endpoints Days in trial")
6
Hypertension remains a major problem world-wide

8
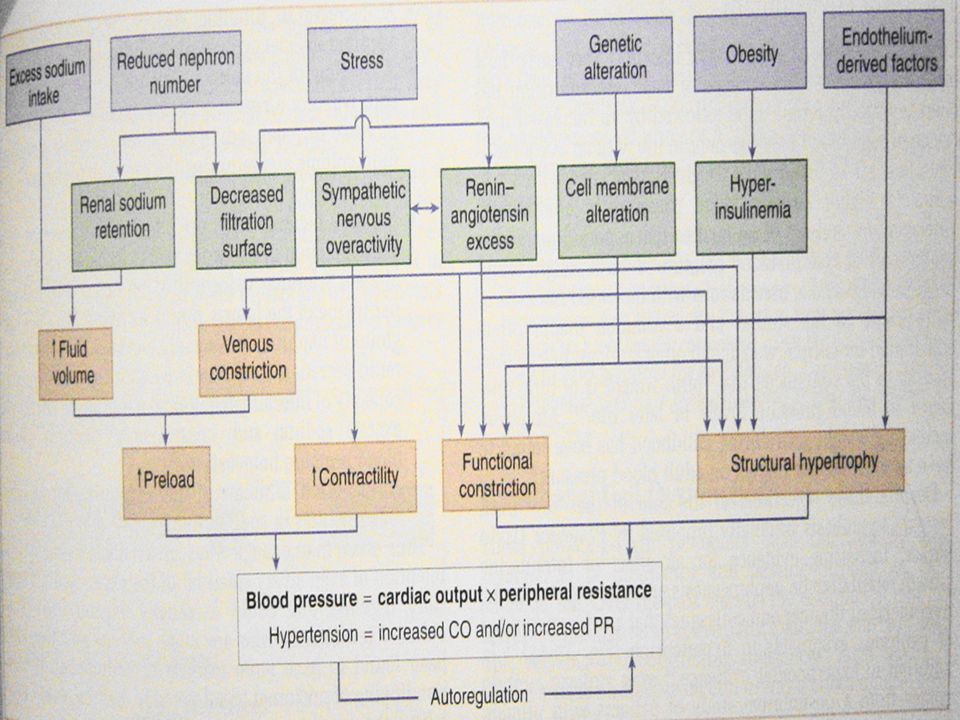
How is blood pressure regulated? BP = CO x TVR CO = SV x HR 3 systems are directly responsible for BP control: –The heart: pumping pressure –Blood vessel tone: determines systemic vascular resistance –Kidney: regulate intravascular volume The maintenance of chronic hypertension requires renal participation, even though the factors responsible may lie outside of the renal parenchyma. No matter how high the cardiac output and how constricted the blood vessels, renal excretion has the capacity to completely return blood pressure to normal levels by reducing intravascular volume

9
Essential hypertension 95% of hypertensive patients have blood pressures that are elevated for no readily definable reason This is called essential HTN The diagnosis of essential HTN is one of exclusion after ruling out of all the causes of secondary HTN It results from the synergy of multiple defects of blood pressure regulation that interact with environmental stressors It is usually not severe and approximately 80% of patients have stage 1 HTN

10
Genetics and environmental factors of HTN

11
Urinary sodium excretion and blood pressure

12
Role of sodium retention in HTN

13
Genetics in HTN: the slavery hypothesis

14
High autonomic nervous system response in essential HTN Microneurographic recordings in a normotensive and a borderline hypertensive subject. Microneurography permits recording of the rate of sympathetic bursts in the peroneal nerve. This method is excellent for evaluation of reflex responses within the same individual and it has been recognized recently to be a sufficiently sensitive and reproducible technique to allow comparison between groups. These recordings show increased rates of sympathetic bursts in the patient with borderline hypertension. They also show a higher rate of discharge on a low-sodium diet in both normotensive and hypertensive subjects.

15
Natural history of HTN: hemodynamic transition from increased cardiac output to increased vascular resistance With time the hemodynamics of hypertension change from an increase of the cardiac output to an increase of vascular resistance

16
The renin angiotensin system in HTN

17
ARB: Site and Mechanism of Action Renin Angiotensinogen ACE Angiotensin I Angiotensin II Non-ACE alternate pathways (CAGE, chymase, cathepsin G) Reduces blood pressure Valsartan AT 1 receptors Vasoconstriction Aldosteronesecretion Renal tubular reabsorption of sodium and water Antidiuretic hormone (vasoprressin) secretion Stimulation of thirst center Catecholaminesecretion X X X X X X
 Reduces blood pressure Valsartan AT 1 receptors Vasoconstriction Aldosteronesecretion Renal tubular reabsorption of sodium and water Antidiuretic hormone (vasoprressin) secretion Stimulation of thirst center Catecholaminesecretion X X X X X X")
18
Vascular mechanisms: Defective endothelium- dependent relaxation in the coronary arteries in hypertension

19
Role of insulin and obesity in HTN 4 postulated mechanisms by which insulin can increase BP: - stimulation of renal Na reabsorption and increase in intravascular volume - increase in activity of sympathetic nervous system - stimulation of arterial vascular smooth muscle hypertrophy - alteration of membrane ion transport, increase in intracellular Ca and increased vascular tone

21
Natural history of HTN Essential HTN arises after young adulthood. Its prevalence increases with age such that > 60% of americans over age 60 have THN In young patients (<40) BP tends to be driven hy high cardiac output in the setting of normal total peripheral resistance With time, CO tends to decline while vascular resistance increases Thus older patients have elevated vascular resistance as the principal abnormality with a normal or reduced CO
 BP tends to be driven hy high cardiac output in the setting of normal total peripheral resistance With time, CO tends to decline while vascular resistance increases Thus older patients have elevated vascular resistance as the principal abnormality with a normal or reduced CO.")
22
Secondary HTN 5% of patients Due to a structural or hormonal cause The condition may be curable Clinical clues of secondary HTN –Age ( 50) –Severity: tends to be severe –Onset: may present abruptly in a patient who was previously normotensive –Absence of family history –Associated signs and symptoms
 –Severity: tends to be severe –Onset: may present abruptly in a patient who was previously normotensive –Absence of family history –Associated signs and symptoms")
23
Causes of HTN

24
Renal parenchymal disease as a cause of secondary HTN Diverse pathological processes may lead to damage to the kidneys Major mechanism of HTN = increased intravascular volume Damaged nephrons are unable to excrete normal amounts of Na and water, leading to a rise in volume, elevated CO and increased BP Excessive production of renin is also incriminated

25
Clinical clues suggesting renovascular HTN

27
Coarctation of the aorta Occurs distal to the origin of the left subclavian artery Flow is increased in upper extremities and head and decreased in lower extremities Mechanisms of HTN: –Reduced blood flow to the kidney with increased renin –Medial hyperplasia in the aortic arch with blunting of normal baroreceptor response to elevated intravascular BP Clinical clues: –Symptoms of inadequate perfusion to the legs –Midsystolic murmur over the back –CXR: indentation of the aorta; notched appearance of the ribs

28
Cushing syndrome

29
Mineralocorticoids excess as a cause of HTN Increased Na reabsorption Increased intravascular volume Decreased K Confirmed by measurment of excessive aldosterone secretion and suppressed plasma renin levels Caused by adrenal adenoma or bilateral hyperplasia of the adrenal glands

30
Clues for the presence of pheochromocytma

31
Strategies for the diagnosis of pheochromocytoma

32
Consequences of HTN

33
Lifestyle Modifications to Manage HTN ModificationRecommendationAverage SBP reduction Weight reduction BMI 18.5-24.9 5-20 mmHg/10 kg loss DASH eating high fruits, vegetables 8-14 mm Hg low fat dairy products Na restriction2.4 g Na or 6 g NaCl2-8 mm Hg Physical activityaerobic; 30 mn/d4-9 mm Hg Limit alcohol< 1-2 drinks/day2-4 mm Hg Combination of > 2 lifestyle modifications can achieve better results

34
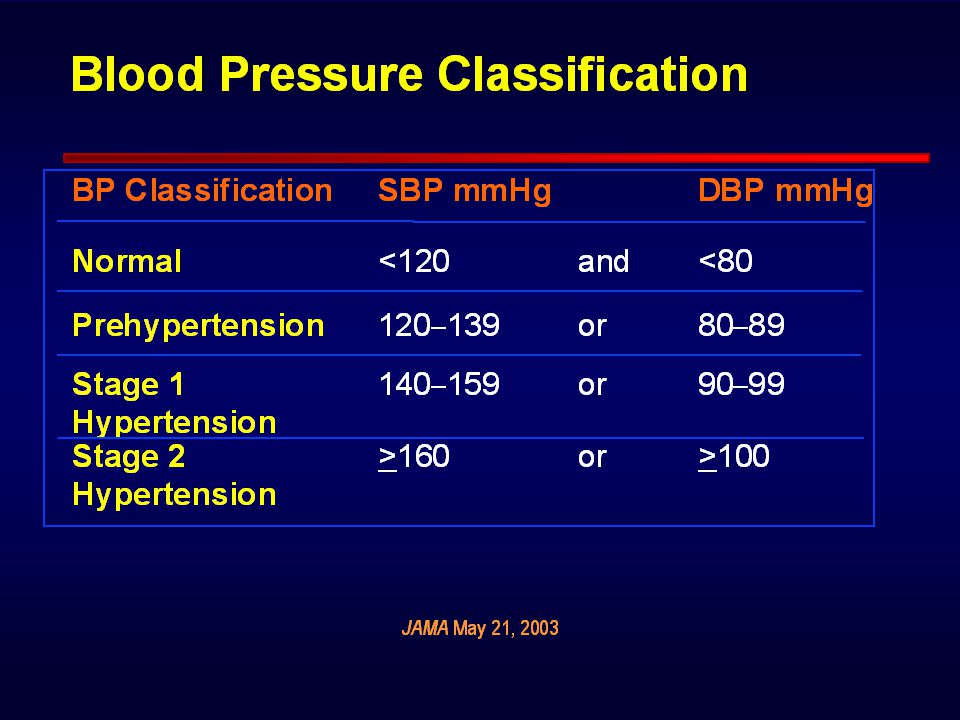
JNC VII: Management of Hypertension by Blood Pressure Classification ACE-I = angiotensin-converting enzyme inhibitor; ARB = angiotensin-receptor blocker; BB = beta blocker; CCB, = calcium channel blocker. Chobanian AV et al. JAMA. 2003;289:2560-2572. Drug(s) for the compelling indications; other antihypertensive drugs (diuretics, ACE-I, ARB, BB, CCB) as needed BP Classification Lifestyle Modification Initial Drug Therapy Without Compelling Indication With Compelling Indication Normal <120/80 mm Hg Prehypertension 120-139/80-89 mm Hg Stage 1 hypertension 140-159/90-99 mm Hg Stage 2 hypertension 160/100 mm Hg Encourage Yes No drug indicatedDrug(s) for the compelling indications Thiazide-type diuretics for most; may consider ACE-I, ARB, BB, CCB, or combination 2-drug combination for most (usually thiazide-type diuretic and ACE-I, ARB, BB, or CCB)
 for the compelling indications; other antihypertensive drugs (diuretics, ACE-I, ARB, BB, CCB) as needed BP Classification Lifestyle Modification Initial Drug Therapy Without Compelling Indication With Compelling Indication Normal <120/80 mm Hg Prehypertension /80-89 mm Hg Stage 1 hypertension /90-99 mm Hg Stage 2 hypertension 160/100 mm Hg Encourage Yes No drug indicatedDrug(s) for the compelling indications Thiazide-type diuretics for most; may consider ACE-I, ARB, BB, CCB, or combination 2-drug combination for most (usually thiazide-type diuretic and ACE-I, ARB, BB, or CCB).")
35
Sites of Action of Major Antihypertensive Drug Classes Diuretics ACEI Calciumchannelblockers + -Blockers ARB Juxtaglomerular cells HeartKidney tubules Vascular smooth muscle JNC VI, 1997; PDR, 1998; Benowitz NL. Basic & Clinical Pharmacology. 1995:147-170. Angiotensin I Angiotensin II AT 1 receptors Renin-angiotensin system xxx

36
Absolute effects of treatment on cardiovascular risk A reduction of 10-14 mm Hg in sys BP and 5-6 mm Hg in diastolic BP confers about 2/5 less stroke, 1/6 less CAD and in Western populations, 1/3 fewer major cardiovascular events overall

Similar presentations


>")


















