Download presentation
Presentation is loading. Please wait.

1
25-26 et 27 janvier 2012 – Marseille - Palais des Congrès RAC et dysfonction VG Docteur Bertrand CORMIER

2
25-26 et 27 janvier 2012 – Marseille - Palais des Congrès Conflit d’Intérêt : aucun Docteur Bertrand CORMIER

3
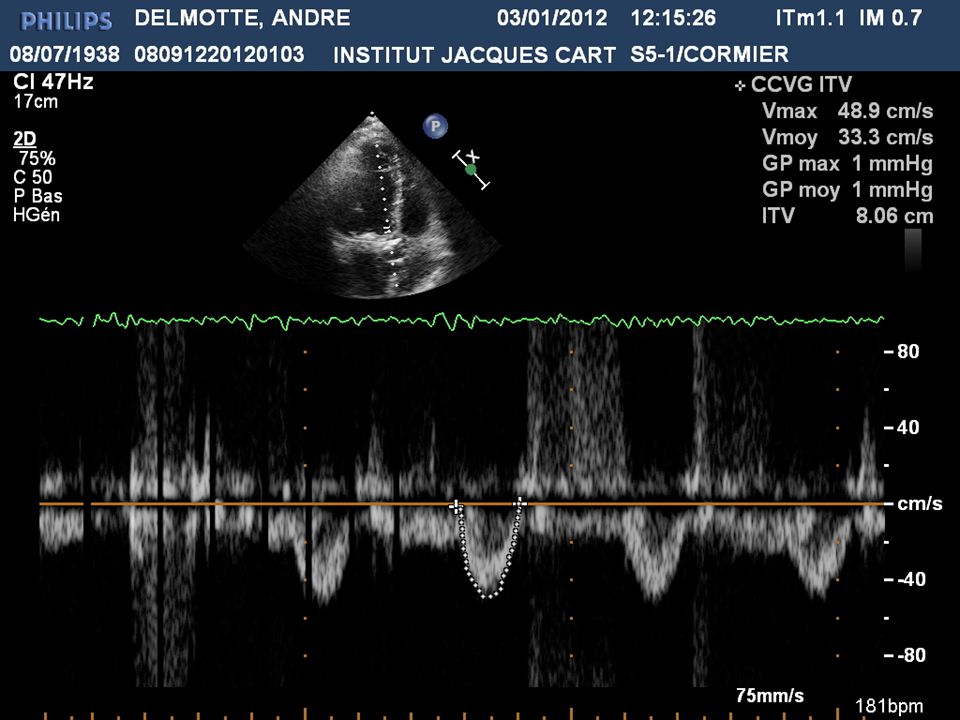
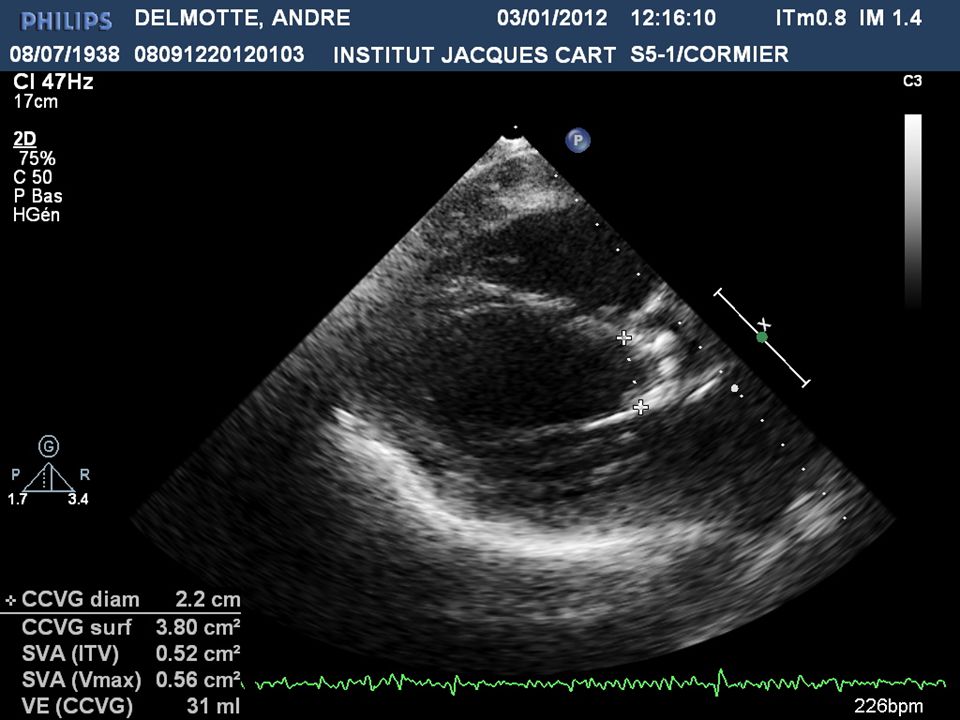
Cas clinique n°1 Mr DEL. André, 73 ans HTA ancienne – Tabac modéré RA connu de longue date, jugé modéré Poussée récente d’insuffisance cardiaque Auscultation pauvre ECG : RS, QRS fins – Coro normale Echo VG 58/47 SIV/PP = 10/10 FE 20 % VTi sous Ao = 8 cm – gradient moyen 15 – Sa0 =0.7 Dobutamine = O réserve contractile Dilatation aortique : O résultat fonctionnel

11
Cas clinique n°1 Scanner cardique:valve tricuspide calcifiée,anneau:23 TAVI prothese Edwards 26

17
cas clinique n°1 Suites simples; O SF Retour à domicile sous traitement medical Pronostic?(def à discuter)
")
18
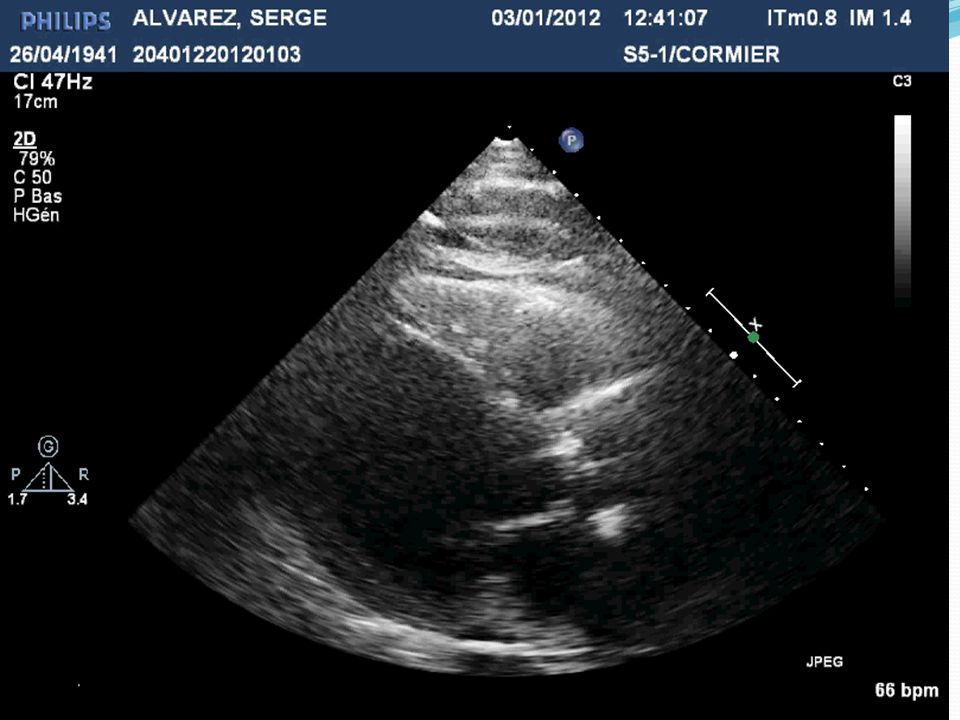
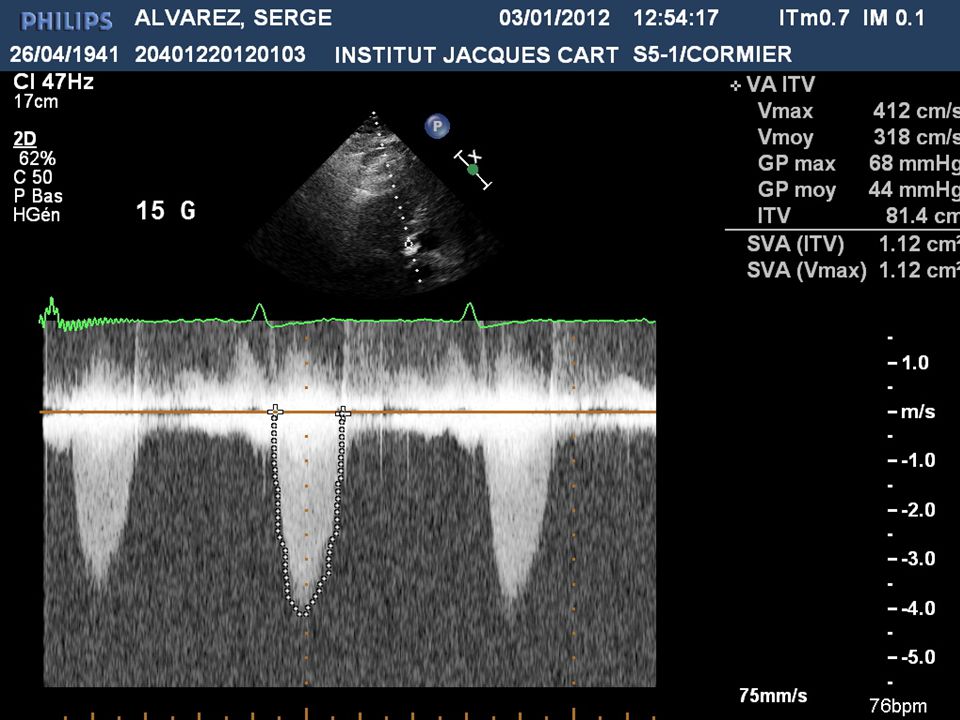
Cas Clinique n°2 Mr ALV. Serge, 70 ans Tabac sevré – DNID – 112 kg, 1m78 CMD connue depuis 2006 coro : sténose D1 Sclérose mitro-aortique - FEVG = 35 % 2011 : 2 poussées d’IC globale Echo FEVG = 35 % - gradient moyen 25 – Sao = 0.8 cm²

28
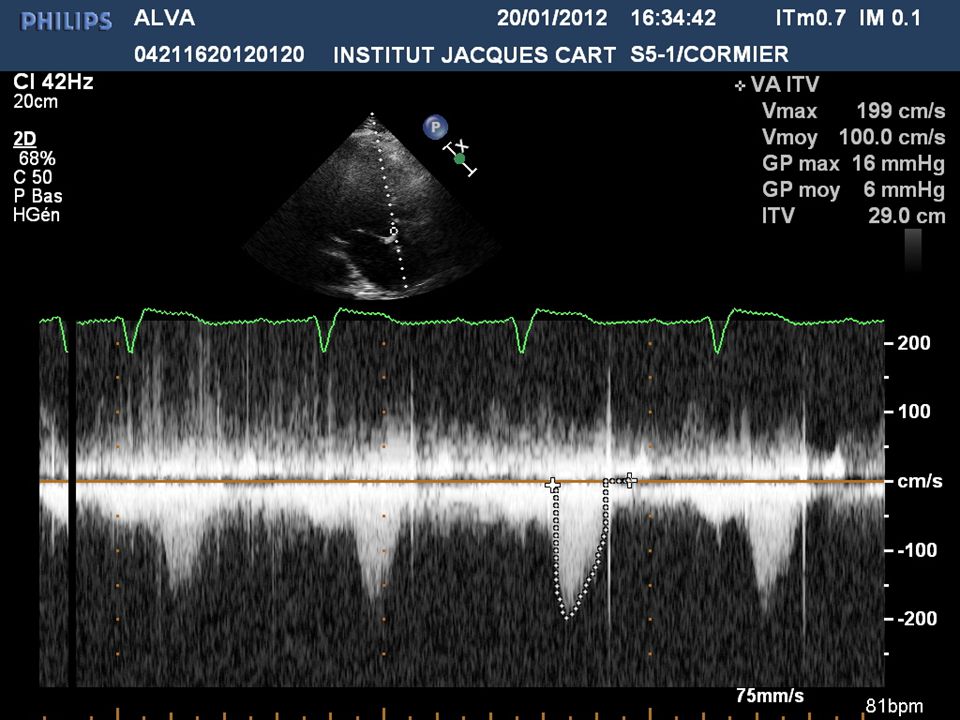
Cas Clinique n°2 Mr ALV. Serge, 70 ans – 2 Echo Dobu RC + gradient moyen = 45 Scanner = valve tricuspide calcifiée – Sao = 0.9 cm² RVA BP 23 – Suites simples, sortie à J+8

33
EuroHeart Survey on VHD B.Iung Eur Heart J, 2003 Prospective study in 92 centers from 25 countries = 5001 VHD AS = 1197 pts 512 interventions : EF ≥ 60= 56.5 % 50-60 = 24.2 % 30-50= 16.4 % < 30= 2.9 %

34
To operate or not pts with severe AS BT.Bouma, Heart 1999 205 pts prospectively evaluated; AVA < 1 cm², mean age= 78 yrs, 48% CAD 94 pts : AVR 111: medical 41 symptomatic pts no surgery : LV dysfunction 14% Advanced age 13% Comorbidity 13% Symptoms attributed to CAD 11% Functional improvement 9% Main risk factors:impaired LVF, NYHA Cl, age

35
Why are so many pts with AS denied surgery ? B.Iung, Eur Heart J 2005 EHS : 216 pts with severe symptomatic AS (angina or NYHA Cl III/IV) AVR = 67 % medical= 33 % Multivariate analysis LVEF [OR= 2.27 for EF 30-50 % = 5.15 for EF ≤ 30 % Age [OR= 1.84 for 80-85 yrs = 3.38 for ≥ 85 yrs vs 75-80 Associated with no surgery
 AVR = 67 % medical= 33 % Multivariate analysis LVEF [OR= 2.27 for EF % = 5.15 for EF ≤ 30 % Age [OR= 1.84 for yrs = 3.38 for ≥ 85 yrs vs Associated with no surgery.")
36
AS and LV systolic dysfunction In the majority of pts with mild-moderate systolic dysfunction, decrease in SV and EF is related to reversible mismatch, likely to reverse when obstruction is relieved pts with severe AS and EF < 50 % : Cl IC for AVR (ESC guidelines, 2008)
")
37
AS and LV systolic dysfunction Severe decrease in EF may be caused by decreased contractility associated with fibrosis due to hypertrophy or surimposed MI. Secondary improvement in LV function is uncertain. The subgroup of pts with severely depressed EF and low flow raises diagnostic and therapeutic difficulties

38
Guidelines for severe AS

39
Inconsistencies of echo criteria for grading AS J Minners, EHJ 2008 ; 29 : 1043-1048 3483 pts with AS

40
Flow dependence of AVA : T he Gorlin equation S = F / K P cm² ml/sec mmHg Cannon, 1985

41
The continuity equation AVA = VTI lvot / VTI AS x CSA lvot

42
Flow dependence of AV resistance and LV stroke work loss Valve resistance = 1.333 x P/Q dynes/s/cm -5 LV SWL = 100 x P/ LVP (%) (Burwash, 1994)
 (Burwash, 1994)")
43
Planimetry of the Aortic Valve Direct measurement of the aortic orifice Using TEE Using TTE (harmonic) Possibly less flow-dependent 0.2 1.0 0.4 0.6 0.8 Max Min AVA Gorlin TEE planimetry cm 2 NS p<0.005 11 pts with dobutamine echo (Tardif et al. J Am Coll Cardiol 1997;29:1296-302)
.")
44
Flow dependence of AVA Relation to valve morphology Shively, 1998 27 pts with AS. TEE planimetry and Dobutamine infusion

45
Calcific AS : time to look more closely at the valve CM OTTO, NEJM 2008

46
Aortic valve area, cm 2 EBCT Score 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 01000200030004000500060007000 8000 R=-0.79, p<0.0001 R=0.86, p<0.0001 Peak aortic valve velocity, m/sec EBCT Score 01000200030004000500060007000 8000 0 1 2 3 4 5 6 7 AVC and Hemodynamic Severity Messika-Zeitoun Circulation 2004

47
Thresholds Scanner MSCT Thresholds Score calcique Sensibilité, %Spécificité, %VPP, %VPN, % 5001003146100 7009849 98 100094655594 120091655992 165182807088 200062867279 300057917472

48
Dobutamine Echocardiography in AS with LV dysfunction (EF< 0.35) and low gradient ( P< 30 mm) De Filippi (1995) Severe AS : VTI, P, no change (<0.3 cm²) in AVA Mild AS : VTI, AVA (> 0.3 cm²), no change in P No reserve ? Nishimura (2002) Severe AS : P > 30 and AVA < 1.2 cm²
 Severe AS : P > 30 and AVA < 1.2 cm².")
49
Operative mortality surgery for valvular heart disease Guidelines, ESC 2008

50
Surgery of AS with LV dysfunction Study (n pts) AVA (cm²) EF (%) CAD/ Previous MI (%) MPG (mmHg) OM (%) 5 yrs survival (%) Predictive factors VAQUETTE (2005) 155 pts (4.1 % of 3819) < 1< 3030/10431271NYHA Cl, SPAP TOPAS (2008) 101 pts < 1.2<40 /60≤ 4018 PAI (2008) 194 Pts < 0.8< 3551/≤ 35958 LEVY (2008) 217 pts < 1< 3528/23≤ 30 16 2090-99 10 2000-05 49MPG < 20 multivessel CAD lack of CR
 AVA (cm²) EF (%) CAD/ Previous MI (%) MPG (mmHg) OM (%) 5 yrs survival (%) Predictive factors VAQUETTE (2005) 155 pts (4.1 % of 3819) < 1< 3030/ NYHA Cl, SPAP TOPAS (2008) 101 pts < 1.2<40 /60≤ 4018 PAI (2008) 194 Pts < 0.8< 3551/≤ LEVY (2008) 217 pts < 1< 3528/23≤ MPG < 20 multivessel CAD lack of CR")
51
Low gradient AS : risk stratification by DSE JL Monin Circulation 2003 Prospective multicenter study : 136 symptomatic pts, AVA = 0.7 cm² (0.6-0.8), MPG 29 mmHg (23-34), LVEF : 0.30 (0.24-0.35) – CI : 2.11 l/mn/m² (1.75-2.55) Significant CAD = 46 % (MVD = 33 %) Gr I : 92 pts with CR ( SV ≥ 20%) vs Gr 2 = 44 pts without CR AVR in 70% of each Gr ;medical tt in pts with older age, comorbidities of pseudo severe AS (9/92 pts) OM = 14 % (5% Gr I, vs 32 % Gr II, p <.002) Predictors of OM : lack of CR (OR : 10.9, p<.001) and MPG ≤ 20 mmHg (OR : 4.7, p<.04) Predictors of LT survival : AVR (p=.001) and CR (p.001)
, MPG 29 mmHg (23-34), LVEF : 0.30 ( ) – CI : 2.11 l/mn/m² ( ) Significant CAD = 46 % (MVD = 33 %) Gr I : 92 pts with CR ( SV ≥ 20%) vs Gr 2 = 44 pts without CR AVR in 70% of each Gr ;medical tt in pts with older age, comorbidities of pseudo severe AS (9/92 pts) OM = 14 % (5% Gr I, vs 32 % Gr II, p <.002) Predictors of OM : lack of CR (OR : 10.9, p<.001) and MPG ≤ 20 mmHg (OR : 4.7, p<.04) Predictors of LT survival : AVR (p=.001) and CR (p.001)")
52
Many Patients Considered too High Risk

53
Indications for AVR in AS with LV dysfunction ACC/AHA no recommendation ESC : AS with low MPG (< 40 mmHg), LV dysfunction and contractile reserve :Cl II a C and no contractile reserve: Cl II b C Decision making according to clinical condition, valve calcification, extent of CAD
, LV dysfunction and contractile reserve :Cl II a C and no contractile reserve: Cl II b C Decision making according to clinical condition, valve calcification, extent of CAD")
54
Outcome after AVR for LF/LG AS without CR C. Tribouilloy, JACC 2009 81 pts prospectively included – AVA < 1 cm², EF ≤ 40 %, MPG ≤ 40 mmHg; no contractile reserve 55 pts : AVR – 26 :medical; Mean Fu : 37 ± 41 m Operative mortality : 22%, 5 yrs survival (excluding OM) : 69 ± 8%
 : 69 ± 8%.")
55
Therapeutic decision in patients without CR BAV as a diagnostic test AVR considered in pts with calcified valve, low comorbidity, with MPG > 20 mmHg and without large scar of infarction

56
Survival benefit of AVR in pts with severe AS and low EF RG. Pai Ann Thorac Surg 2008 Echo Database : 194 pts with AVA ≤ 0.8 and EF ≤ 0.35

57
Symptomatic severe AS : Room for improvement ? MWA Van Geldorps – Eur J Cardiovasc Surg 2009 Echo database 2004-2007 – 179 severe symptomatic AS FU : 17 m 76 intervention : AVR 63,TAVI or apical = 10 100 (56 %) medical treatment Operative risk deemed too high = 34 % (mean Euroscore : 11.6) Mildly symptomatic pts = 19 % AS considered non-severe = 14 % Patient preference = 9 % Missing reason = 20 %
 medical treatment Operative risk deemed too high = 34 % (mean Euroscore : 11.6) Mildly symptomatic pts = 19 % AS considered non-severe = 14 % Patient preference = 9 % Missing reason = 20 %.")
58
PARTNER T.Lefevre, Eur Heart J 2011

59
Hemodynamics results and changes in myocardial function after TAVI M. Gotzmann, Am Heart J 2010 39 TAVI (Medtronic CoreValve) before, 30 d and 6 m Before30 days6 monthsp NYHA III/IV %921518<.001 BNP (pg/ml)744±708367±273279±186- Aortic MPg47.4±13.810.2±410±3.2- AVA0.83±0.162.01±0.32.08±0.3- AR III/IV (%)23108 LV Mi (g/m²)158±46147±40138±45- EF (%)44.1±654±7.656.8±9.5- E/E’20±6.718.1±517.2±5NS
 before, 30 d and 6 m Before30 days6 monthsp NYHA III/IV %921518<.001 BNP (pg/ml)744±708367±273279±186- Aortic MPg47.4± ±410±3.2- AVA0.83± ± ±0.3- AR III/IV (%)23108 LV Mi (g/m²)158±46147±40138±45- EF (%)44.1±654± ±9.5- E/E’20± ±517.2±5NS.")
60
Comparison of hemodynamic performance of percutaneous and surgical BP in AS MA Clavel, JACC 2009 50 PAVI (femoral : 38 ; apical 12)matched with 50 CE Magna (ST gr) or freestyle (SL gr) for sex, aortic annulus diameter, LVEF, BSA and BMI
matched with 50 CE Magna (ST gr) or freestyle (SL gr) for sex, aortic annulus diameter, LVEF, BSA and BMI")
61
Long-term outcomes after TAVI in high-risk pts The UK registry – NE MOAT JACC 2011 ; 58 : 2130-8 All TAVI prospectively collected (2007-2009) within the UK (25 centers), mortality status in 100% by December 2010 870 pts = TF route : 599 (69 %) other 271 (31 %) Medtronic Corevalve = 452 (52 %) Edwards Sapien = 410 (48 %) 213 pts alive at 2 years FU
 within the UK (25 centers), mortality status in 100% by December pts = TF route : 599 (69 %) other 271 (31 %) Medtronic Corevalve = 452 (52 %) Edwards Sapien = 410 (48 %) 213 pts alive at 2 years FU")
62
NE Moat JACC 2011

64
AS and poor LV function Conclusion - 1 LV dysfunction is an uncommon consequence of AS (< 10 %) MPG > 30 mmHg despite low EF in favor of mismatch and represents an indication for AVR
 MPG > 30 mmHg despite low EF in favor of mismatch and represents an indication for AVR")
65
Conclusion - 2 The subgroup of pts with severe LV dysfunction, LF, LMPG poses diagnostic and therapeutic difficulties : due to the flow dependence of the main hemodynamic criteria, the diagnosis of severe AS is based on anatomy and the response to Dobutamine infusion Patients with CR should undergo valve intervention as well as patients without CR but with low comorbidity, MPG > 20 mmHg and no extensive scar of MI

66
Conclusion - 3 Despite the recommendations and a risk-benefit ratio in favor of surgery,a large proportion of symptomatic pts remains not operated on and referral to surgical departments should be encouraged to have more interdisciplinary discussions and to optimize therapeutic indications

Similar presentations





































>")
