Download presentation
Presentation is loading. Please wait.

1
From the desk of: Dr. Asha Jain Senior Gynecologist NHMC & H

2
It is a process of spontaneous per vaginum expulsion of mature fetus with vertex presentation followed by after births and which ends without any artificial aids, complications and which is not delayed. Abnormal labor is complicated labor

3
There are 3 stages Stage 1: from onset of labor to full dilatation of cervix. Duration is 5-10 hours. Stage 2: from full dilatation to expulsion of fetus. Duration ½ to 1 hour. Stage 3: Stage of expulsion of after births. Duration is 5 min -1/2 hour. Total duration of normal labor Primi: 12-16 hours Multi: 6-8 hours

4
The series of movements which a fetus undergoes while passing through the maternal birth canal. 1. Flexion and descent 2. Engagement 3. Internal rotation 4. Extension 5. Restitution 6. External rotation 7. Lateral flexion

5
Incidence of normal labor: it varies from community to community and generally normal labor and operative labor is 85% and 15% respectively. incidence of hospital and domiciliary delivery in India: 65:35% Comparison between hospital and home delivery Safety factors Hospital deliveryHome delivery safety saferLess safe Availability of facilities GoodPoor Skilled personnel PresentNot available Incidence of normal labor More operativeMore normal delivery Management of complications ProperImproper Psychological care LackingPresent Cross infection Does occurLess likely New born care BetterPoorer Post natal care BetterPoorer cost MoreLess

6
1 st stage: 1. Admission of woman 2. Thorough general and obstetric examination 3. Preparation of the parts 4. Enema 5. General advise 6. Food in labor 7. Pain relief in labor 8. Monitoring of labor- PARTOGRAPHY

9
2 nd stage: 1. Observe signs of 2 nd stage of labor 2. Woman taken to the delivery table 3. Continuous monitoring of the vitals and fetal heart rate every 15 minutes 4. Position of the woman and vaginal examination after cleaning and draping 5. Preparation by the birth attendant 6. Evacuation of bladder 7. Patient is encouraged to bear down with further progress of labor 8. Perineal infilteration with episiotomy before crowning of the head 9. Observe crowning 10. Head is delivered by supporting perineum and flexing the coming head 11. Once head is delivered eyes are cleaned, looked for cord around the neck 12. Delivery of the shoulders and trunk 13. Care of new born – APGAR SCORE

10
3 rd stage: Active management 1. Watch for the signs of separation of placenta 2. Delivery of placenta by control cord traction 3. Receive and inspect placenta 4. Watch for any signs of PPH and obtain proper hemostasis 5. Suturing of episiotomy

11
4 th stage: 1. Observation of the female after delivery for at least ½ an hour

12
Post partum hemorrhage: (Atonic 80% and traumatic 20%) excessive hemorrhage from genital tract after the birth of baby amounting to a degree affecting general condition of the patient. Statistically if blood loss is more than 500 ml. Incidence 0.5 % of hospital delivery. Maternal morbidity 10% Types: primary and secondary Primary Diagnosis and management: a) Atonic: Prolonged labor, over distended uterus, abnormal presentations, abnormal uterine contractions b) Traumatic: cervical and perineal tears, ppt labor Secondary Retained placental pieces Subinvolution of uterus Deep lacerations of cervix Infections Choriocarcinoma Management: General : IV fluid, blood transfusion and uterotonic drugs Surgical: Exploration of the genital tract, uterine compression Late stage: ligation of uterine artery, ligation of anterior division of internal iliac artery, hysterectomy
 Atonic: Prolonged labor, over distended uterus, abnormal presentations, abnormal uterine contractions b) Traumatic: cervical and perineal tears, ppt labor Secondary Retained placental pieces Subinvolution of uterus Deep lacerations of cervix Infections Choriocarcinoma Management: General : IV fluid, blood transfusion and uterotonic drugs Surgical: Exploration of the genital tract, uterine compression Late stage: ligation of uterine artery, ligation of anterior division of internal iliac artery, hysterectomy.")
13
Retained placenta: When the placenta is retained for more than 15 min Causes: 1) atonic uterus 2) Morbid adhesions of placenta- placenta accreta, placenta increta and placenta percreta 3) Constriction ring Incidence: 0.4% amongst hospital deliveries Dangers: PPH and shock, puerperal sepsis, thrombophlebitis, embolism and placental polyp later on. Proper management of 3 rd stage may prevent retention of placenta.

14
Inversion of uterus: it is the turning inside out of the uterus. It is one of the rare but serious complications. Causes: mismanagement of the 3 rd stage, pull on the cord while uterus is atonic, short cord Maternal mortality is high if immediate management is not given.

15
Amniotic fluid embolism is spontaneous embolism of amniotic fluid debris in small pulmonary artery leading to varying degree of respiratory distress and circulatory collapse. It is rare but dramatic and deadliest complication. Risk factors: 1)vigorous labor contractions 2) Rent through fetal membranes as in marginal separation of placenta Prognosis varies on the severity and fatal for mother in severe cases.
vigorous labor contractions 2) Rent through fetal membranes as in marginal separation of placenta Prognosis varies on the severity and fatal for mother in severe cases..")
16
Shock is a state of collapse of circulation so that there is a critical deduction of perfusion of tissues by blood with oxygen Causes: Hemorrhagic- all 3 rd stage complications Non hemorrhagic- trauma of obstetric operations like breech extraction, MRP, internal podalic version etc., obstetric accidents like rupture of uterus, abruptio placenta, acute inversion etc., due to anesthesia and drugs, pulmonary embolism

17
Sepsis- delayed complication Puerperal sepsis and septic shock

18
It is defined as when 1 st and 2 nd stage of labor lasts for more than 24 hours. Incidence: it occurs 25% in primi and 2%in multi Risk factors: 1) age and parity- elderly primi 2) CPD and fetal malposition 3) Uterine distention- twins, hydramnios 4) Uterine defects- fibroid, malformation 5) Injudicious use of analgesics 6) Injudicious induction of labor 7) Unknown cases like genetic, familial, nutrition etc. Complications: maternal and fetal distress, 3 rd satge complications and high perinatal morbidity and mortality.
 age and parity- elderly primi 2) CPD and fetal malposition 3) Uterine distention- twins, hydramnios 4) Uterine defects- fibroid, malformation 5) Injudicious use of analgesics 6) Injudicious induction of labor 7) Unknown cases like genetic, familial, nutrition etc. Complications: maternal and fetal distress, 3 rd satge complications and high perinatal morbidity and mortality..")
19
It is extremely fast labor due to over efficient uterine action and labor may end within 3 hours. Causes: 1) common in multigravida rarely in primi 2) Injudicious use of oxytocin 3) Unusual lack of resistance in cervix and lower uterine segment Dangers: maternal and fetal injuries
 common in multigravida rarely in primi 2) Injudicious use of oxytocin 3) Unusual lack of resistance in cervix and lower uterine segment Dangers: maternal and fetal injuries.")
20
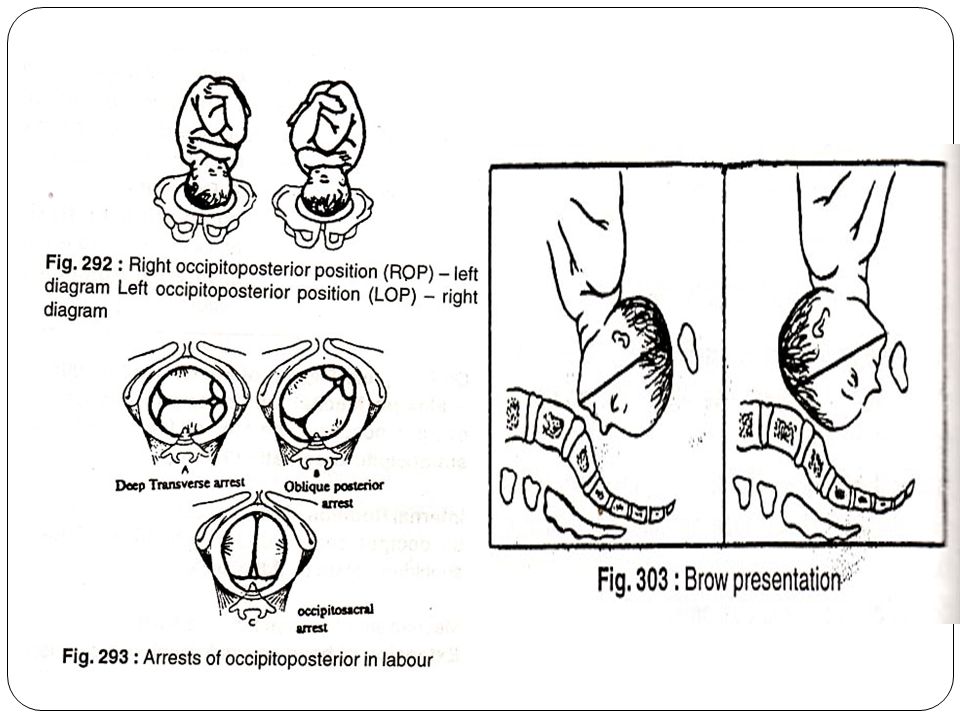
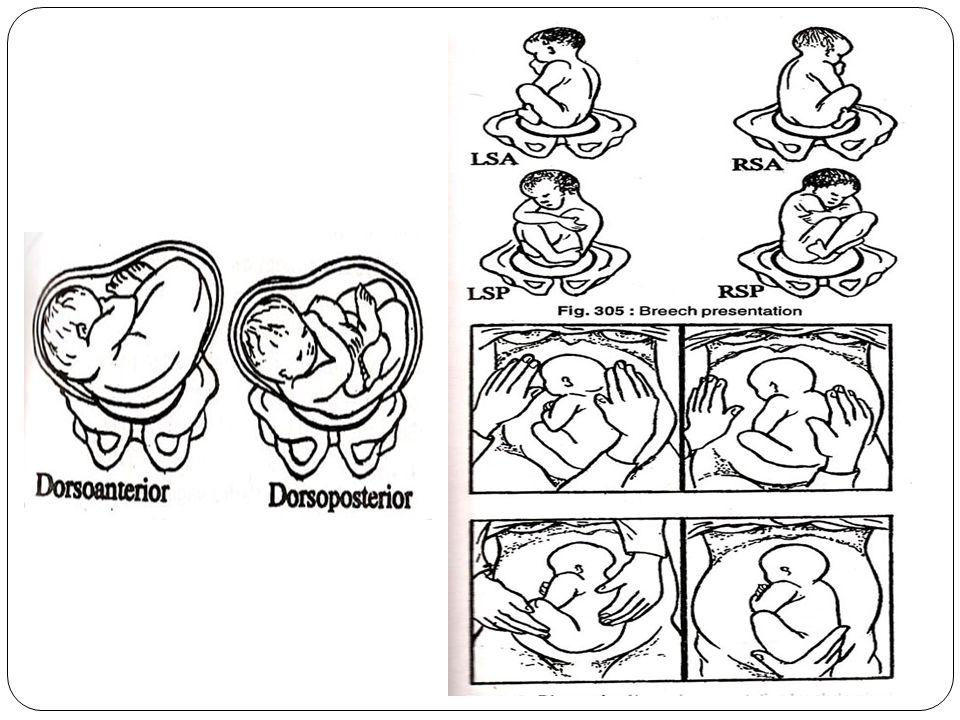
Total 14% of pregnancies have abnormal presentations 1. Occipito posterior 2. Face 0.2% 3. Brow 0.1% 4. Breech 3.2% 5. Shoulder 0.5%

24
1. Narrow midpelvis- antropoid or platypeloid 2. Deflexion of head or large fetus 3. Uterine inertia 4. Pendulous abdomen 5. Malformed fetus 6. Uterine anomalies and uterine tumors 7. Placenta praevia 8. Hydramnios

25
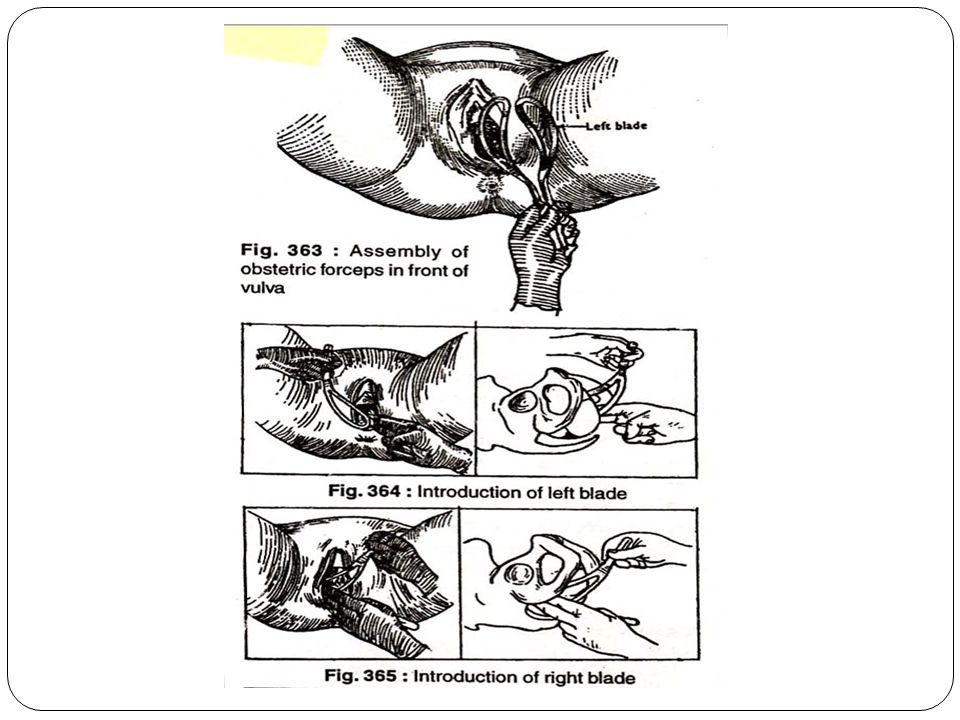
Obstetric forceps is the instrument designed for the extraction of fetus when presenting by vertex or face or the after coming head of breech. Indications: 1) delayed 2 nd stage 2) Fetal distress 3) Maternal distress 4) Elective forceps in high risk patients like eclampsia, heart disease, severe PET 5) After coming head of breech Complications: 1) maternal injuries- tears of cervix and vagina, 3 rd degree perineal tear, bladder injury, PPH, nerve injuries 2) Fetal injuries- neonatal asphyxia, tentorial tear, cephalhematoma, facial paralysis, late complications like mental retardation and cerebral palsy. Perinatal mortality can be 2%
 delayed 2 nd stage 2) Fetal distress 3) Maternal distress 4) Elective forceps in high risk patients like eclampsia, heart disease, severe PET 5) After coming head of breech Complications: 1) maternal injuries- tears of cervix and vagina, 3 rd degree perineal tear, bladder injury, PPH, nerve injuries 2) Fetal injuries- neonatal asphyxia, tentorial tear, cephalhematoma, facial paralysis, late complications like mental retardation and cerebral palsy. Perinatal mortality can be 2%.")
27
This is the abdominal delivery of the baby by laprotomy and section of the uterus after 28 weeks of pregnancy. Indications: 1) Absolute: when vaginal delivery is impossible a. severe degree of CPD b. central placenta praevia c. pelvic mass obstructing the passage d. advanced CA cervix e. vaginal obstruction like atresia, stenosis 2) Relative: here vaginal delivery may be possible with or without aids but maternal and fetal risk is very high. a. CPD b. previous caesarean 2 or more c. ante partum hemorrhage d. mal presentations e. failed induction of labor f. bad obstetric history g. hypertensive disorders h. other medical disorders i. fetal distress
 Absolute: when vaginal delivery is impossible a. severe degree of CPD b. central placenta praevia c. pelvic mass obstructing the passage d. advanced CA cervix e. vaginal obstruction like atresia, stenosis 2) Relative: here vaginal delivery may be possible with or without aids but maternal and fetal risk is very high. a. CPD b. previous caesarean 2 or more c. ante partum hemorrhage d. mal presentations e. failed induction of labor f. bad obstetric history g. hypertensive disorders h. other medical disorders i. fetal distress.")
28
Time of operation: elective and emergency Types: 1. lower segment section 2. classical or upper segment section Caesarean hysterectomy: this is an abdominal delivery of the baby by CS followed by hysterecomy. Indiacations are uncontrollable PPDH placenta accreta Risks and complications: 1. Hemorrahge 20%, 2. Anesthetic complication: aspiration pneumonitis, cardiac arrest 3. Infections: puerperal sepsis, wound infection, paralytic ilieus, burst abdomen, septic shock 4. Leg vein thrombosis 5. Remote gynecological: menstrual disorders, chronic pelvic pain, infertility, scar endometriosis, VVF, incisional hernia, scar rupture in future pregnancy 6. Maternal mortality is 0.2-0.5% Main causes of death: infection, hemorrhage, thromboembolism and anesthetic accidents Mortality is more in cases of late referral and high risk labors Perinatal mortality: 5-10% due to high incidence of emergency CS and high risk pregnancies Causes of perinatal death: asphyxia or hypoxia, RDS, prematurity, intracranial hemorrhage, infections

Similar presentations







: leading cause of maternal mortality worldwide Prevalence rate: 6% Africa has highest prevalence.>")
 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")















