Download presentation
Presentation is loading. Please wait.

1
Newborn Pearls-Evidence Based
Ann Soenen, D.O. May 16, 2014 Photo of epstein perls Large phone baby- prezi Unique findings that are still relatively common for a family doctor to see and know what to do with

2
Objectives Become familiar with the Stanford online photo gallery
Recognize unique newborn exam findings Formulate a treatment plan for these issues Provide valuable instructions to the parents through use of a post-nursery discharge checklist Focus on my own top 10 questions- will assume you know what is normal on exam Newborn vitals- what is normal? BP? Subgaleal protocol– what to do? Heart murmurs- when do I need to echo? What is CHD screening? Tongue-tied, trim or not indicated? Red reflex- see or not? Goopy eyes- when to cx, when to probe dacrocystitis? Sacral dimple? Ortho-Extra digits? Club foot? DDH- Hip click? Mgmt Undescended testicle and circ stuff Skin Abdomen -- Handouts- Iowa NMS (what all included?) Discharge instructions (laminated card)
 Discharge instructions (laminated card)")
4
Gimme the vitals Apgars Temp HR RR BP Know how to calculate
axilla of 36.1 to 37°C (97 to 98.6°F) in an open crib HR 120 to 160 RR 40 to 60 BP depends on gestational age, weight You just delivered this baby- Apgars- know how to calculate for boards HR ? RR? Normal or abnormal? Consult NICU? Temperature measured with the thermometer in the axilla of 36.1 to 37°C (97 to 98.6°F) in an open crib [1]. ●Respiratory rate of 40 to 60 breaths per minute, which should be counted over a full minute. ●Heart rate of 120 to 160 beats per minute. The heart rate may decrease to 85 to 90 beats per minute in some term infants during sleep. In these infants, an increase of heart rate with stimulation is reassuring.
 in an open crib. HR. 120 to 160. RR. 40 to 60. BP. depends on gestational age, weight. You just delivered this baby- Apgars- know how to calculate for boards. HR RR Normal or abnormal Consult NICU Temperature measured with the thermometer in the axilla of 36.1 to 37°C (97 to 98.6°F) in an open crib [1]. ●Respiratory rate of 40 to 60 breaths per minute, which should be counted over a full minute. ●Heart rate of 120 to 160 beats per minute. The heart rate may decrease to 85 to 90 beats per minute in some term infants during sleep. In these infants, an increase of heart rate with stimulation is reassuring.")
5
Apgars

6
Newborn Hypertension? 40 weeks 50% 95% 99% SBP 80 95 100 DBP 50 65 70
MAP 60 75 38 weeks 77 92 97 59 74 79 36 weeks 72 87 57 BP- 50, 95, 99% UTD In summary, the following observations about normal neonatal BP can be concluded from the above studies: The primary determinant of neonatal BP is postconceptional age. In neonates admitted to the NICU, BP varies with gestational age, postconceptional age, and birth weight. In all infants regardless of gestation, the rise in BP is higher during the first week of life. The rate of rise is more rapid in preterm compared with term infants. In healthy term infants, BP does not vary based on growth parameters or gestational age. BP does increase over the first three to four days of life, but levels off sooner than what is observed in preterm infants. These results demonstrate how challenging it is to establish normative values for neonatal BP, especially in preterm infants, because of the effects of gestational age and maturation on BP values. These issues, plus the lack of large scale, prospective, multicenter studies of neonatal BP, further complicate the problem of defining normative BP data for neonates, especially premature and ill term infants. Nevertheless, based on a review of these data, a reference table of normal BP values at or after two weeks of age in infants between 26 and 44 weeks postconceptional age has been published (table 1) [6]. This table, which is based on the best available data through 2010, can be used clinically to identify infants with hypertension defined as persistent BP elevation greater than the 95th percentile. These infants require further evaluation and/or treatment. (See 'Evaluation' below and "Management of hypertension in infants".)
 [6]. This table, which is based on the best available data through 2010, can be used clinically to identify infants with hypertension defined as persistent BP elevation greater than the 95th percentile. These infants require further evaluation and/or treatment. (See Evaluation below and Management of hypertension in infants .)")
7
Newborn Skin Rashes-Birthmarks
CONGENITAL MELANOCYTIC NEVI DERMAL MELANOSIS HEMANGIOMAS NEVUS FLAMMEUS NEVUS SIMPLEX AFP

8
Newborn Skin Rashes- Common Rashes
Transient Vascular Phenomenon CUTIS MARMORATA HARLEQUIN COLOR CHANGE Erythema Toxicum Neonatorum Transient Neonatal Pustular Melanosis Acne Neonatorum Milia Miliaria (crystallina and rubra) Seborrheic Dermatitis AFP Pustules/vesicles Scale (differentiate from atopic dermatitis) Tx of Seborrheic Dermatitis
 Seborrheic Dermatitis. AFP. Pustules/vesicles. Scale (differentiate from atopic dermatitis) Tx of Seborrheic Dermatitis.")
9
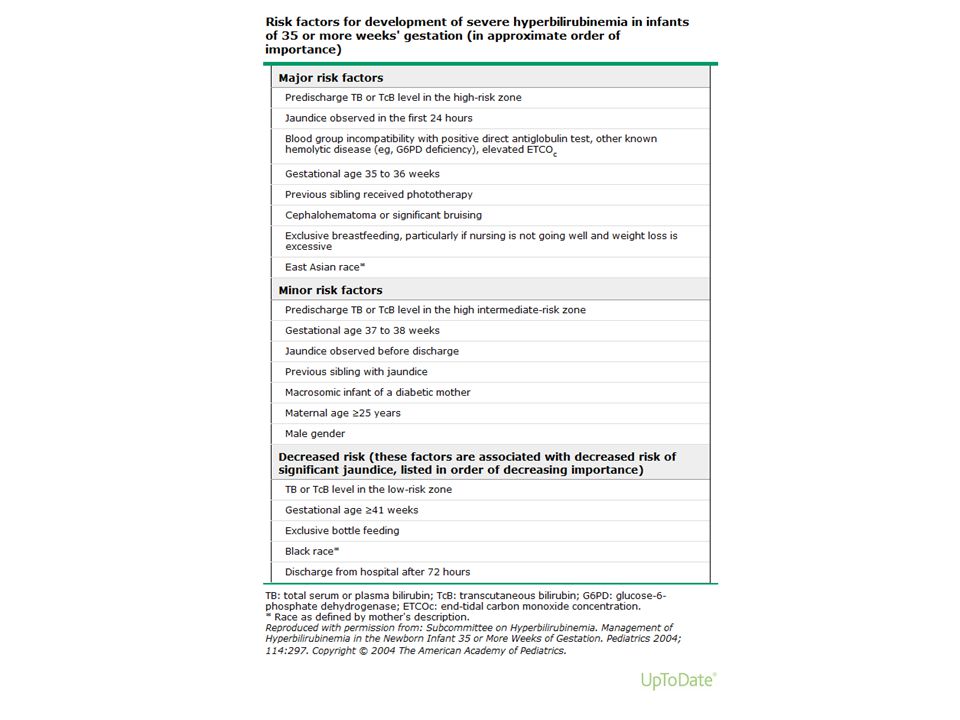
Yellow? Never normal in 1st 24 hours Eyeball vs TcB vs TsB?
Visual assessment not as reliable TcB not reliable during phototherapy, ?darkly pigmented skin TcB can replace TB in most circumstances when TB is <15 mg/dL Universal screening or Selective screening? If intermediate-risk zone -> now what? Yellow song- How good are we clinically in guessing level? Visual assessment is not as reliable as measurement of TB to detect significant hyperbilirubinemia [10,11]. As a result, in our practice, universal screening includes bilirubin testing prior to discharge. Is visual assessment of jaundice reliable as a screening tool to detect significant neonatal hyperbilirubinemia? Riskin A, Tamir A, Kugelman A, Hemo M, Bader D J Pediatr. 2008;152(6):782 Visual assessment of jaundice in term and late preterm infants. Keren R, Tremont K, Luan X, Cnaan A Arch Dis Child Fetal Neonatal Ed. 2009;94(5):F317. If yellow in 1st 24 hours- worry about hemolysis. We are going to talk about healthy, term baby. USPSTF not support universal screening, but kernicterus rare – so unlikely to be able to study. Bilirubin measurement for neonates: comparison of 9 frequently used methods. Grohmann K, Roser M, Rolinski B, Kadow I, Müller C, Goerlach-Graw A, Nauck M, Küster H Pediatrics. 2006;117(4):1174 When to confirm with TB — A confirmatory TB should be measured in the following settings [22,46]: When TcB exceeds the 75th percentile on the TB nomogram for phototherapy (figure 1). When the TcB exceeds the 95th percentile on the TcB nomogram. At follow-up after discharge, if the TcB >13 mg/dL (222 micromol/L). When therapeutic intervention is being considered. Therapy should be initiated while awaiting confirmatory results. If the management plan would be altered by considering the TB to be equal to TcB + 3 mg/dL (51 micromol/L). ADDITIONAL EVALUATION — Infants who have total serum or plasma bilirubin (TB) values ≥95th percentile or suspicion of hemolytic disease require subsequent measurement(s) of TB and further evaluation to determine the etiology of jaundice. (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn".) Initial tests that should be obtained are [8]: Blood type and direct Coombs’ test Complete blood count and smear Reticulocyte count Glucose-6-phosphate dehydrogenase (G6PD) measurement, if clinically appropriate Direct or conjugated bilirubin End-tidal CO concentration (ETCOc) (if available) TB should be repeated in 4 to 24 hours depending upon the infant's age, TB value, and anticipated rate of TB rise
:782. Visual assessment of jaundice in term and late preterm infants. Keren R, Tremont K, Luan X, Cnaan A. Arch Dis Child Fetal Neonatal Ed. 2009;94(5):F317. If yellow in 1st 24 hours- worry about hemolysis. We are going to talk about healthy, term baby. USPSTF not support universal screening, but kernicterus rare – so unlikely to be able to study. Bilirubin measurement for neonates: comparison of 9 frequently used methods. Grohmann K, Roser M, Rolinski B, Kadow I, Müller C, Goerlach-Graw A, Nauck M, Küster H. Pediatrics. 2006;117(4):1174. When to confirm with TB — A confirmatory TB should be measured in the following settings [22,46]: When TcB exceeds the 75th percentile on the TB nomogram for phototherapy (figure 1). When the TcB exceeds the 95th percentile on the TcB nomogram. At follow-up after discharge, if the TcB >13 mg/dL (222 micromol/L). When therapeutic intervention is being considered. Therapy should be initiated while awaiting confirmatory results. If the management plan would be altered by considering the TB to be equal to TcB + 3 mg/dL (51 micromol/L). ADDITIONAL EVALUATION — Infants who have total serum or plasma bilirubin (TB) values ≥95th percentile or suspicion of hemolytic disease require subsequent measurement(s) of TB and further evaluation to determine the etiology of jaundice. (See Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn .) Initial tests that should be obtained are [8]: Blood type and direct Coombs’ test. Complete blood count and smear. Reticulocyte count. Glucose-6-phosphate dehydrogenase (G6PD) measurement, if clinically appropriate. Direct or conjugated bilirubin. End-tidal CO concentration (ETCOc) (if available) TB should be repeated in 4 to 24 hours depending upon the infant s age, TB value, and anticipated rate of TB rise.")
11
Phototherapy Plot the curve or online calculator- bilitool.org NNT
It is estimated that 5 to 10 infants with TB between 15 and 20 mg/dL must receive phototherapy to prevent one patient from developing a TB >20 mg/dL. Decline of TB at least 2 to 3 mg/dL within four to six hours Result in 30-40% decrease in 24 hours Additional evaluation or not? Home Bili-blankets? It is estimated that 5 to 10 infants with TB between 15 and 20 mg/dL must receive phototherapy to prevent one patient from developing a TB >20 mg/dL. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia Pediatrics. 2004;114(1):297. Intensive phototherapy results in a decline of TB of at least 2 to 3 mg/dL (34 to 51 micromol/L) within four to six hours. A decrease in TB can be measured as soon as two hours after initiation of treatment. In infants ≥35 weeks GA, 24 hours of intensive phototherapy can result in a 30 to 40 percent decrease in the initial TB [22]. With conventional phototherapy, a decline of 6 to 20 percent can be expected in the first 18 to 24 hours [11,23,24]. Home phototherapy — As an alternative to readmission to the hospital, phototherapy can be administered to term infants at home. Home phototherapy is less disruptive to the family and can be considered for otherwise healthy term infants (>38 weeks gestational age [GA]) without hemolysis or other risk factors who have TB levels 2 to 3 mg/dL (34 to 51 micromol/L) below the recommended threshold level for initiation of hospital phototherapy, are feeding well, and can be closely followed [2].
:297. Intensive phototherapy results in a decline of TB of at least 2 to 3 mg/dL (34 to 51 micromol/L) within four to six hours. A decrease in TB can be measured as soon as two hours after initiation of treatment. In infants ≥35 weeks GA, 24 hours of intensive phototherapy can result in a 30 to 40 percent decrease in the initial TB [22]. With conventional phototherapy, a decline of 6 to 20 percent can be expected in the first 18 to 24 hours [11,23,24]. Home phototherapy — As an alternative to readmission to the hospital, phototherapy can be administered to term infants at home. Home phototherapy is less disruptive to the family and can be considered for otherwise healthy term infants (>38 weeks gestational age [GA]) without hemolysis or other risk factors who have TB levels 2 to 3 mg/dL (34 to 51 micromol/L) below the recommended threshold level for initiation of hospital phototherapy, are feeding well, and can be closely followed [2].")
14
24 hours of age: >12 mg/dL 48 hours of age: >15 mg/dL
For infants at low risk (≥38 weeks GA and without risk factors), phototherapy is started at the following TB values. 24 hours of age: >12 mg/dL 48 hours of age: >15 mg/dL 72 hours of age: >18 mg/dL Infants in this category who have TB levels 2 to 3 mg/dL below the recommended levels may be treated with fiberoptic or conventional phototherapy at home. Photo of bili-blanket
, phototherapy is started at the following TB values. 24 hours of age: >12 mg/dL. 48 hours of age: >15 mg/dL. 72 hours of age: >18 mg/dL Infants in this category who have TB levels 2 to 3 mg/dL below the recommended levels may be treated with fiberoptic or conventional phototherapy at home. Photo of bili-blanket.")
15
Murmurs Innocent or not? Guess the problem? (Stanford audio file)
In the first few days after birth, most newborns have murmurs that are transient and benign. They usually are caused by a patent ductus arteriosus (PDA), or pulmonary branch stenosis [10,20]. The latter is more likely if the murmur persists after 24 hours when most PDAs have closed. The PDA murmur is continuous, often described as "machinery-like" or harsh in quality. It usually is loudest under the left clavicle (second intercostal space), but may radiate down the left sternal border. Features associated with innocent murmurs are [24]: ●Murmur intensity grade II or less, heard at left sternal border ●Normal second heart sound ●No audible clicks ●Normal pulses ●No other abnormalities Signs that suggest congenital heart disease are: ●Murmur intensity grade III or higher ●Harsh quality ●Pansystolic duration ●Loudest at upper left sternal border ●Abnormal second heart sound ●Absent or diminished femoral pulses ●Other abnormalities
, or pulmonary branch stenosis [10,20]. The latter is more likely if the murmur persists after 24 hours when most PDAs have closed. The PDA murmur is continuous, often described as machinery-like or harsh in quality. It usually is loudest under the left clavicle (second intercostal space), but may radiate down the left sternal border. Features associated with innocent murmurs are [24]: ●Murmur intensity grade II or less, heard at left sternal border. ●Normal second heart sound. ●No audible clicks. ●Normal pulses. ●No other abnormalities. Signs that suggest congenital heart disease are: ●Murmur intensity grade III or higher. ●Harsh quality. ●Pansystolic duration. ●Loudest at upper left sternal border. ●Abnormal second heart sound. ●Absent or diminished femoral pulses. ●Other abnormalities.")
16
Congenital Heart Disease
Didn’t you hear it? Often Missed CHD O2 screening (Lancet 2012-universal) Postductal (NOT R arm) SpO2 <95 % Detection rate on prenatal ultrasound Highly variable Better if 4-chamber view w/ outflow tracts or fetal echo U/s in utero- how often pick up? CHD O2 screening--A cutoff SpO2 <95 percent is generally used as it provides a sensitivity around 75 percent and specificity of 90 percent or greater [82]. Pulse oximetry screening for critical congenital heart defects in asymptomatic newborn babies: a systematic review and meta-analysis. Thangaratinam S, Brown K, Zamora J, Khan KS, Ewer AK Lancet Jun;379(9835): Epub 2012 May 2. one report, a murmur had been detected in the neonatal period in 38 percent of infants who presented with heart failure due to a left heart obstructive lesion by six weeks of age [54]. In another study, a neonatal murmur was heard in 57 percent of infants who died with CHD after discharge [55]. However, many infants with murmurs do not have structural lesions, and CHD occurs in infants who do not have murmurs. This was illustrated by a study in which echocardiography was performed in all 46 of 7204 newborns (0.6 percent) with murmurs detected during routine examination by obstetric or pediatric house officers [56]. ●Of 46 newborns with a murmur, 13 had normal hearts and 8 had normal hearts with physiologic findings that would account for a murmur (eg, patent ductus arteriosus [PDA] or mild pulmonary artery branch stenosis). Of the 25 infants (54 percent) with cardiac malformations, all of whom were asymptomatic, ventricular septal defect (VSD) occurred in 15, coarctation of the aorta in 3, tetralogy of Fallot in 3, atrial septal defect in 2, and pulmonary stenosis and aortic valve stenosis in 1 each. ●CHD was also detected before 12 months of age in 32 infants who had no murmur on the initial examination. In another report, echocardiography was performed in 170 of 20,323 newborns (0.8 percent) between one and five days of age, who were referred for evaluation of murmur with an otherwise normal examination [57]. Structural heart disease was identified in 146 (86 percent). The most common lesions were VSD (n = 54) and patent ductus arteriosus (n = 34). Seven had complex cardiac disease, and stenosis of the pulmonary or aortic valve occurred in six and three infants, respectively. Prevalence and clinical significance of cardiac murmurs in neonates. Ainsworth S, Wyllie JP, Wren C Arch Dis Child Fetal Neonatal Ed. 1999;80(1):F43. The majority of innocent murmurs in term infants are due to benign pulmonary branch stenosis (PBS), also known as peripheral pulmonary stenosis. This condition is usually detected as a grade 1-2/6, mid-systolic, high-pitched or blowing ejection murmur heard best in the pulmonary area with radiation to the axilla and back after the infant is 24 hours of age, when most PDAs have closed [58]. The murmur may be due to the relative hypoplasia at birth of the branch pulmonary arteries compared with the main pulmonary artery (which is large because it feeds the PDA and systemic circulation in utero) and its sharp angle of origin [59-63]. Another innocent finding on auscultation in infants is a Still's murmur thought to arise from the vibrations of the attachments of the pulmonic valve leaflets. These low pitched, vibratory, musical, grade 1-2/6 systolic ejection murmurs are usually best heard between the lower left sternal border and apex. They typically decrease in intensity or resolve with a Valsalva maneuver, which can be induced in infants by gentle pressure on the abdomen. Still's murmurs tend to vary with heart rate, becoming more evident as the heart rate slows; however, they are relatively uncommon in the newborn. Thus, the American Academy of Pediatrics (AAP), the American Heart Association (AHA), and the American College of Cardiology Foundation (ACCF) [27] have recommended universal screening of all newborns with pulse oximetry to improve the recognition of CHD. Variability of prenatal ultrasound — The sensitivity of prenatal screening with echocardiography for major heart disease is highly variable, ranging from 0 to 80 percent detection rates. Factors affecting sensitivity include operator training and experience, gestational age, maternal weight, fetal position, and type of defect. The efficacy of prenatal sonographic screening for CHD is discussed separately. (See "Prenatal sonographic diagnosis of fetal cardiac anomalies", section on 'Efficacy'.) Performance of four chamber screening has been assessed in numerous studies. Unfortunately, the sensitivity for major heart disease has been highly variable, ranging from 0 to 80 percent detection rates [14-17]. Factors affecting sensitivity include operator experience, gestational age, maternal weight, fetal position, and type of defect [18-20]. In 1997, a review of 13 published screening studies described over 100,000 screened pregnancies and reported a composite sensitivity of only 23 percent [14]. The largest study performed in the United States was also included in the above review. The RADIUS Trial randomly assigned 15,000 low-risk women to have either two scans routinely during pregnancy or scans only for indications. Among women scanned at primary care sites, there were no cases of fetal congenital heart disease correctly identified, including a failure to detect any of eight cases of complex heart defects. Among those women seen at referral practices, 5/11 cases of complex heart disease (45 percent) were detected by prenatal ultrasound [21]. However, experienced ultrasonographers go beyond the standard four chamber examination by expanding the views obtained to include the cardiac outflow tracts. This adds to sensitivity in the detection of fetal cardiac anomalies, resulting in detection rates of 50 to 90 percent [22]. In 2006, the Italian group described above conducted another multicenter prospective observational study in 15 obstetric units in the Piedmont Region of Italy [23]. Over 7000 women were screened and complete follow-up information was available for 90 percent. Fifty-eight cases of congenital heart disease were observed at birth or postmortem; 38 of which were diagnosed in utero. Sensitivity of ultrasound for detection of congenital heart disease was 65.5 percent. The authors attributed the higher sensitivity to inclusion of the outflow tract view in the examination, technological developments, and better training of the operators. Attempts to perform full cardiac studies as part of routine second trimester fetal ultrasound have yielded high sensitivity rates, approximately 90 percent at 20 to 22 weeks [24,25]. The practicality of this approach for routine application has yet to be proven. Fetal cardiac assessment should include a four chamber view; viewing the outflow tracts in an extended basic cardiac examination is also important. The optimum time for visualization of the fetal heart and outflow tracts is 18 to 22 weeks of gestation If risk factor- maternal diabetes, FHx CHD, cardiac teratogenic med exposure (lithium)- then get fetal echo
 Postductal (NOT R arm) SpO2 <95 % Detection rate on prenatal ultrasound. Highly variable. Better if 4-chamber view w/ outflow tracts or fetal echo. U/s in utero- how often pick up CHD O2 screening--A cutoff SpO2 <95 percent is generally used as it provides a sensitivity around 75 percent and specificity of 90 percent or greater [82]. Pulse oximetry screening for critical congenital heart defects in asymptomatic newborn babies: a systematic review and meta-analysis. Thangaratinam S, Brown K, Zamora J, Khan KS, Ewer AK. Lancet Jun;379(9835): Epub 2012 May 2. one report, a murmur had been detected in the neonatal period in 38 percent of infants who presented with heart failure due to a left heart obstructive lesion by six weeks of age [54]. In another study, a neonatal murmur was heard in 57 percent of infants who died with CHD after discharge [55]. However, many infants with murmurs do not have structural lesions, and CHD occurs in infants who do not have murmurs. This was illustrated by a study in which echocardiography was performed in all 46 of 7204 newborns (0.6 percent) with murmurs detected during routine examination by obstetric or pediatric house officers [56]. ●Of 46 newborns with a murmur, 13 had normal hearts and 8 had normal hearts with physiologic findings that would account for a murmur (eg, patent ductus arteriosus [PDA] or mild pulmonary artery branch stenosis). Of the 25 infants (54 percent) with cardiac malformations, all of whom were asymptomatic, ventricular septal defect (VSD) occurred in 15, coarctation of the aorta in 3, tetralogy of Fallot in 3, atrial septal defect in 2, and pulmonary stenosis and aortic valve stenosis in 1 each. ●CHD was also detected before 12 months of age in 32 infants who had no murmur on the initial examination. In another report, echocardiography was performed in 170 of 20,323 newborns (0.8 percent) between one and five days of age, who were referred for evaluation of murmur with an otherwise normal examination [57]. Structural heart disease was identified in 146 (86 percent). The most common lesions were VSD (n = 54) and patent ductus arteriosus (n = 34). Seven had complex cardiac disease, and stenosis of the pulmonary or aortic valve occurred in six and three infants, respectively. Prevalence and clinical significance of cardiac murmurs in neonates. Ainsworth S, Wyllie JP, Wren C. Arch Dis Child Fetal Neonatal Ed. 1999;80(1):F43. The majority of innocent murmurs in term infants are due to benign pulmonary branch stenosis (PBS), also known as peripheral pulmonary stenosis. This condition is usually detected as a grade 1-2/6, mid-systolic, high-pitched or blowing ejection murmur heard best in the pulmonary area with radiation to the axilla and back after the infant is 24 hours of age, when most PDAs have closed [58]. The murmur may be due to the relative hypoplasia at birth of the branch pulmonary arteries compared with the main pulmonary artery (which is large because it feeds the PDA and systemic circulation in utero) and its sharp angle of origin [59-63]. Another innocent finding on auscultation in infants is a Still s murmur thought to arise from the vibrations of the attachments of the pulmonic valve leaflets. These low pitched, vibratory, musical, grade 1-2/6 systolic ejection murmurs are usually best heard between the lower left sternal border and apex. They typically decrease in intensity or resolve with a Valsalva maneuver, which can be induced in infants by gentle pressure on the abdomen. Still s murmurs tend to vary with heart rate, becoming more evident as the heart rate slows; however, they are relatively uncommon in the newborn. Thus, the American Academy of Pediatrics (AAP), the American Heart Association (AHA), and the American College of Cardiology Foundation (ACCF) [27] have recommended universal screening of all newborns with pulse oximetry to improve the recognition of CHD. Variability of prenatal ultrasound — The sensitivity of prenatal screening with echocardiography for major heart disease is highly variable, ranging from 0 to 80 percent detection rates. Factors affecting sensitivity include operator training and experience, gestational age, maternal weight, fetal position, and type of defect. The efficacy of prenatal sonographic screening for CHD is discussed separately. (See Prenatal sonographic diagnosis of fetal cardiac anomalies , section on Efficacy .) Performance of four chamber screening has been assessed in numerous studies. Unfortunately, the sensitivity for major heart disease has been highly variable, ranging from 0 to 80 percent detection rates [14-17]. Factors affecting sensitivity include operator experience, gestational age, maternal weight, fetal position, and type of defect [18-20]. In 1997, a review of 13 published screening studies described over 100,000 screened pregnancies and reported a composite sensitivity of only 23 percent [14]. The largest study performed in the United States was also included in the above review. The RADIUS Trial randomly assigned 15,000 low-risk women to have either two scans routinely during pregnancy or scans only for indications. Among women scanned at primary care sites, there were no cases of fetal congenital heart disease correctly identified, including a failure to detect any of eight cases of complex heart defects. Among those women seen at referral practices, 5/11 cases of complex heart disease (45 percent) were detected by prenatal ultrasound [21]. However, experienced ultrasonographers go beyond the standard four chamber examination by expanding the views obtained to include the cardiac outflow tracts. This adds to sensitivity in the detection of fetal cardiac anomalies, resulting in detection rates of 50 to 90 percent [22]. In 2006, the Italian group described above conducted another multicenter prospective observational study in 15 obstetric units in the Piedmont Region of Italy [23]. Over 7000 women were screened and complete follow-up information was available for 90 percent. Fifty-eight cases of congenital heart disease were observed at birth or postmortem; 38 of which were diagnosed in utero. Sensitivity of ultrasound for detection of congenital heart disease was 65.5 percent. The authors attributed the higher sensitivity to inclusion of the outflow tract view in the examination, technological developments, and better training of the operators. Attempts to perform full cardiac studies as part of routine second trimester fetal ultrasound have yielded high sensitivity rates, approximately 90 percent at 20 to 22 weeks [24,25]. The practicality of this approach for routine application has yet to be proven. Fetal cardiac assessment should include a four chamber view; viewing the outflow tracts in an extended basic cardiac examination is also important. The optimum time for visualization of the fetal heart and outflow tracts is 18 to 22 weeks of gestation. If risk factor- maternal diabetes, FHx CHD, cardiac teratogenic med exposure (lithium)- then get fetal echo.")
18
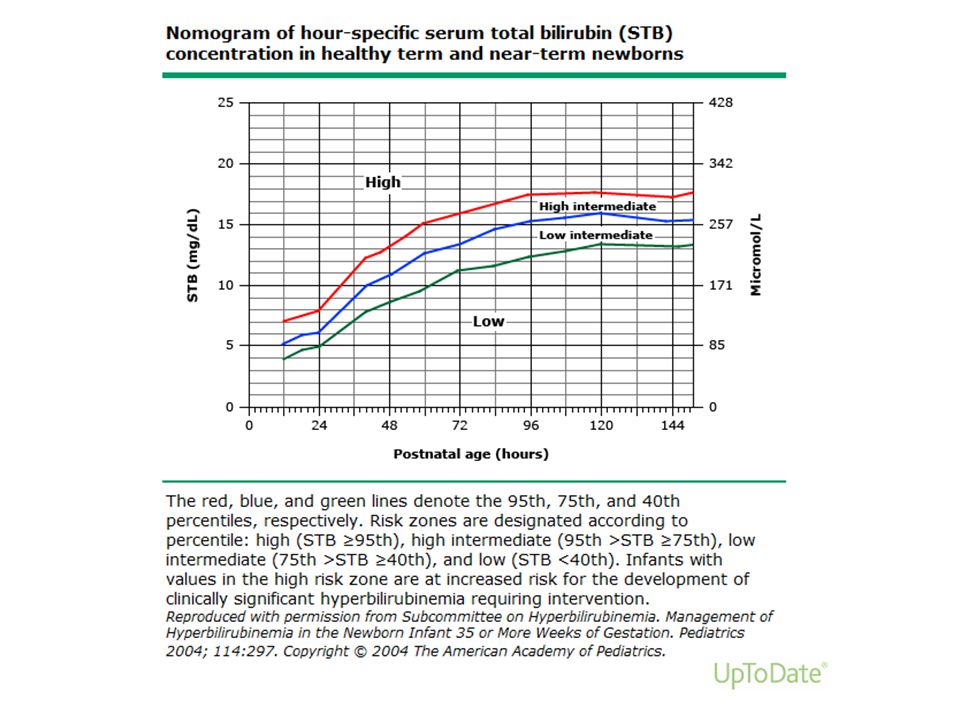
Head The Abnormal Fontanel Caput vs cephalohematoma
Large anterior fontanel or delayed closure Achondroplasia, Hypothyroidism, Down Syndrome, Rickets, Increased intracranial pressure Caput vs cephalohematoma When will it improve? Subgaleal protocols Craniosynostosis Start at head Diamond vs triangle ●Caput succedaneum is an area of edema over the presenting part of the head. This common condition typically is present at birth, crosses suture lines, and resolves within a few days. ●Cephalohematomas are subperiosteal collections of blood that are present in 1 to 2 percent of newborns. On palpation, they form a fluctuant mass that does not cross suture lines, which may increase in size after birth, and usually take weeks to months to resolve. ●Subgaleal hemorrhages are collections of blood between the aponeurosis covering the scalp and the periosteum. Subgaleal hemorrhages extend across suture lines, but feel firm and fluctuant. Blood loss from these hemorrhages can be extensive and life threatening. Common medical condtions associated with a large anterior fontanel or delayed fontanel closure include all the following except? Achondroplasia Congenital hypothyroidism Down Syndrome Rickets Increased Intracranial pressure A list of the medical conditions associated with a large fontanel or delayed fontanel closure can be found in Table 1.20,21 Achondroplasia, congenital hypothyroidism, Down syndrome, rickets, and increased intracranial pressure are among the most common conditions. AAFP article 2003

20
At two months of age, the posterior fontanelle closes, followed by anterior fontanelle closure at approximately two years. The anterolateral and posterolateral fontanelles close at three months and one year, respectively. While the metopic suture typically closes at two years of age, all remaining patent sutures close in adulthood following completion of craniofacial growth.

21
Red Reflex- now I see it now I don’t
Leukocoria DDx: retinoblastoma, congenital cataract How soon to see ophthalmology? Darker pigmented skin? The normal red reflex is seen if the lens and underlying structures are clear. Dark spots in the red reflex, a markedly diminished reflex, presence of a white reflex, or asymmetry of the reflex are indications for referral to an ophthalmologist. Abnormalities of the lens (eg, cataract), vitreous (eg, persistent fetal vasculature), or retina (eg, retinoblastoma) produce a white pupil (leukocoria). UTD Should see opthalmology in 1 wk for dilated eye exam – often under anesthesia
, vitreous (eg, persistent fetal vasculature), or retina (eg, retinoblastoma) produce a white pupil (leukocoria). UTD. Should see opthalmology in 1 wk for dilated eye exam – often under anesthesia.")
22
Dacro- what? Dacryostenosis Dacrocystocele or dacryocele or NLD cyst
Nasolacrimal duct obstruction, m/c cause of tearing in infants Spontaneous resolution by 6 months in 90% Tx: Lacrimal cyst massage Probing Dacrocystocele or dacryocele or NLD cyst Refer to opthalmology urgently Dacrocystitis Systemic antibiotics Nasolacrimal duct (NLD) obstruction (dacryostenosis) is the most common cause of persistent tearing and ocular discharge in children. Spontaneous resolution occurs by six months of age in up to 90 percent of children with congenital nasolacrimal duct (NLD) obstruction [2]. The chance of spontaneous resolution decreases between 6 and 12 months of age, but still occurs. By some accounts, fewer than 1 percent of NLD obstructions that are present at 12 months of age resolve spontaneously Dacryocystocele — A dacryocystocele (also known as dacryocele, amniotocele, or nasolacrimal duct cyst) is produced when both the proximal and distal portions of the nasolacrimal system are obstructed. The distal obstruction is generally at the level of the membrane of Hasner. The proximal obstruction typically occurs in the common canaliculus or at the valve of Rosenmuller (figure 1). The proximal obstruction is a one-way valve that permits tears to enter, but not to reflux out of the canaliculi of the lacrimal drainage system. Dacryocystoceles usually are noted at or shortly after birth. A bluish swelling of the skin overlying the lacrimal sac and superior displacement of the medial canthal tendon is typical (picture 3). The diagnosis can be confirmed by neuroimaging (image 1), though it is usually obvious clinically and further work-up generally is not necessary.
 obstruction (dacryostenosis) is the most common cause of persistent tearing and ocular discharge in children. Spontaneous resolution occurs by six months of age in up to 90 percent of children with congenital nasolacrimal duct (NLD) obstruction [2]. The chance of spontaneous resolution decreases between 6 and 12 months of age, but still occurs. By some accounts, fewer than 1 percent of NLD obstructions that are present at 12 months of age resolve spontaneously. Dacryocystocele — A dacryocystocele (also known as dacryocele, amniotocele, or nasolacrimal duct cyst) is produced when both the proximal and distal portions of the nasolacrimal system are obstructed. The distal obstruction is generally at the level of the membrane of Hasner. The proximal obstruction typically occurs in the common canaliculus or at the valve of Rosenmuller (figure 1). The proximal obstruction is a one-way valve that permits tears to enter, but not to reflux out of the canaliculi of the lacrimal drainage system. Dacryocystoceles usually are noted at or shortly after birth. A bluish swelling of the skin overlying the lacrimal sac and superior displacement of the medial canthal tendon is typical (picture 3). The diagnosis can be confirmed by neuroimaging (image 1), though it is usually obvious clinically and further work-up generally is not necessary.")
23
Tongue-Tied History of Frenotomy for Ankyloglossia:
Popularity of casual frenotomy in the early 20th century Procedure fraught with complications: bleeding, infection, scarring, "regenerating" Fell into disrepute in the mid 20th century Concurrent popularity of formula feeding Older and recent text books claimed frenotomy unnecessary Current resurgence of breastfeeding demands revisit of topic “Cat’s Got Your Tongue” Tongue-tie occurs in approximately 4% of newborns. Many babies with this condition can breastfeed without difficulty, but in some cases, a tight frenulum makes latching on difficult. In those cases, frenotomy may be indicated. The Hazelbaker Assessment Tool for Lingual Frenulum Function is one tool that may be used to grade the severity of the tongue-tie objectively. (Video clip of assessment being done). There are no prospective trials on the outcome of speech in those infants identified at birth, so this is not currently an evidence based reason to clip the frenulum in the nursery. The impact on breastfeeding, however, is well documented.
. There are no prospective trials on the outcome of speech in those infants identified at birth, so this is not currently an evidence based reason to clip the frenulum in the nursery. The impact on breastfeeding, however, is well documented.")
24
Frenotomy or Frenulectomy
Maternal complications- sore nipples Infant complications- FTT Pediatric complications- speech, orthodontic, social Hazelbaker Assessment Tool for Lingual Frenulum Function No anesthesia if performed under 3-4 months, can do in office References : Jeanne L. Ballard, Christine E. Auer and Jane C. Khoury Ankyloglossia: Assessment, Incidence, and Effect of Frenuloplasty on the Breastfeeding Dyad J Pediatrics 2002;110;63-DOI: /peds e63

25
Abdominal masses Normal or not? Umbilical hernia Umbilical cord
Diastasis recti Umbilical hernia Management Umbilical cord Single umbilical artery Care & Normal detachment (in 1 wk) Umbilical granuloma tx? Many normal infants have diastasis recti, resulting from the nonunion of the two rectus muscles, which may result in an umbilical hernia. Cord separation normally occurs one week after birth [25]. This was illustrated in a subsequent study of the previously mentioned Nepalese community-based trial that demonstrated a mean umbilical separation time of 4.2, 4.3, and 5.3 days in infants who received dry care, soap/water, or chlorhexidine umbilical cord care, respectively [25]. In addition, multiple cleansings with chlorhexidine increased the time for cord separation to a mean duration of 7.5 days [26]. Longer time periods to separation are associated with other antiseptic topical agents used in cord care including salicylate sugar powder (mean 5.6 days) [27], 70 percent alcohol (mean 16.9 days) [27], and triple dye (range three to eight weeks) [28]. A single umbilical artery (SUA) is present in approximately 0.2 to 0.6 percent of singleton live births, and at a higher incidence in twin gestations [25]. SUA is associated with an increased rate of chromosomal and other congenital anomalies, including renal abnormalities 20-30%[26]. Currently available data demonstrate there is a low risk of a significant renal abnormality in infants with an isolated SUA. As a result, we do not perform further imaging for healthy term infants with a SUA if there is no other identified abnormality. (See "Care of the umbilicus and management of umbilical disorders", section on 'Single umbilical artery'.) Umbilical hernias are commonly found in children, generally easily reducible, and usually resolve without intervention over the first five years of life. Surgical repair is required in those patients with incarcerated hernia. We suggest surgical repair for patients with large defects (>1.5 cm in diameter) that fail to decrease in size or are symptomatic (Grade 2C). In the newborn, the most common cause of umbilical drainage is umbilical granuloma. Other causes of umbilical drainage include omphalitis and umbilical anomalies, such as omphalomesenteric duct and urachal abnormalities. The most common treatment for umbilical granuloma is topical 75 percent silver nitrate, usually applied by a wooden applicator with premounted silver nitrate. The lesion is treated once or twice a week for several weeks, but generally only a few applications are required for successful treatment. Caution should be exercised in applying silver nitrate because it can cause chemical burns or staining of the surrounding skin. In cases that fail to respond to topical silver nitrate, ligation can be performed in the office without discomfort [49]. Before ligation, the umbilicus should be carefully examined to rule out other causes of umbilical masses, such as umbilical polyp. Failure of the granuloma to resolve with ligation and/or silver nitrate should also increase the suspicion that the lesion is actually an umbilical polyp.
 Umbilical granuloma tx Many normal infants have diastasis recti, resulting from the nonunion of the two rectus muscles, which may result in an umbilical hernia. Cord separation normally occurs one week after birth [25]. This was illustrated in a subsequent study of the previously mentioned Nepalese community-based trial that demonstrated a mean umbilical separation time of 4.2, 4.3, and 5.3 days in infants who received dry care, soap/water, or chlorhexidine umbilical cord care, respectively [25]. In addition, multiple cleansings with chlorhexidine increased the time for cord separation to a mean duration of 7.5 days [26]. Longer time periods to separation are associated with other antiseptic topical agents used in cord care including salicylate sugar powder (mean 5.6 days) [27], 70 percent alcohol (mean 16.9 days) [27], and triple dye (range three to eight weeks) [28]. A single umbilical artery (SUA) is present in approximately 0.2 to 0.6 percent of singleton live births, and at a higher incidence in twin gestations [25]. SUA is associated with an increased rate of chromosomal and other congenital anomalies, including renal abnormalities 20-30%[26]. Currently available data demonstrate there is a low risk of a significant renal abnormality in infants with an isolated SUA. As a result, we do not perform further imaging for healthy term infants with a SUA if there is no other identified abnormality. (See Care of the umbilicus and management of umbilical disorders , section on Single umbilical artery .) Umbilical hernias are commonly found in children, generally easily reducible, and usually resolve without intervention over the first five years of life. Surgical repair is required in those patients with incarcerated hernia. We suggest surgical repair for patients with large defects (>1.5 cm in diameter) that fail to decrease in size or are symptomatic (Grade 2C). In the newborn, the most common cause of umbilical drainage is umbilical granuloma. Other causes of umbilical drainage include omphalitis and umbilical anomalies, such as omphalomesenteric duct and urachal abnormalities. The most common treatment for umbilical granuloma is topical 75 percent silver nitrate, usually applied by a wooden applicator with premounted silver nitrate. The lesion is treated once or twice a week for several weeks, but generally only a few applications are required for successful treatment. Caution should be exercised in applying silver nitrate because it can cause chemical burns or staining of the surrounding skin. In cases that fail to respond to topical silver nitrate, ligation can be performed in the office without discomfort [49]. Before ligation, the umbilicus should be carefully examined to rule out other causes of umbilical masses, such as umbilical polyp. Failure of the granuloma to resolve with ligation and/or silver nitrate should also increase the suspicion that the lesion is actually an umbilical polyp.")
26
Preauricular Skin tags/pits
Do all need screened for renal anomalies? Screen for hearing impairment Evaluation of Newborns with Preauricular Skin Lesions REX DANCEL, MD, MPH, University of North Carolina School of Medicine, Chapel Hill, North Carolina DAVID PRICE, MD, and LEONORA KAUFMANN, MLIS, Carolinas Medical Center, Charlotte, North Carolina Am Fam Physician. 2012 May 15;85(10): Evidence-Based Answer All newborns should be screened for hearing loss, whether or not they have preauricular skin lesions. Newborns with these anomalies may be at increased risk of hearing impairment. (Strength of Recommendation [SOR]: C, based on small observational studies and expert opinion.) Although there is a reported association between renal tract abnormalities and isolated preauricular skin lesions in infants, studies that have used renal ultrasonography to evaluate these patients are inconclusive. Physicians should not perform renal imaging on newborns with preauricular skin lesions unless they have other congenital malformations. (SOR: C, based on small, observational, disease-oriented studies.) From AAFP FPIN In addition, external ear malformations often are associated with syndromes of multiple congenital anomalies that include renal malformations [14]. However, patients with isolated minor external ear anomalies (eg, preauricular skin tags or pits) do not appear to have a significant increased risk of renal anomalies. As a result, although controversial, routine renal imaging for patients with isolated minor ear abnormalities appears to be unnecessary unless accompanied by other major malformations or multiple congenital anomaly syndromes [15]. (See "Congenital anomalies of the ear", section on 'Preauricular pits'.) Children with preauricular pits or tags are at five times the risk of the general population for permanent hearing impairment [23]. Preauricular pits do not require surgery unless they become repeatedly infected or discharge squamous material (picture 4) [21]. If surgery is performed, it should include excision of the pit, the squamous-lined cyst usually present beneath the skin (picture 6), and the cartilage at the root of the helix en bloc to avoid recurrence (picture 7) [27]. Accessory auricular appendage/preauricular tag — Accessory hillocks composed of skin, subcutaneous fat, and/or cartilage may occur near the auricle or anywhere along the anterior border of the sternocleidomastoid muscle (picture 8). These accessory auricular appendages are called preauricular tags when they are present in the preauricular area. Such appendages usually are removed in childhood for cosmetic purposes. Children with accessory auricular appendages may have associated unilateral hearing loss [23]. They should have complete audiologic testing, preferably at birth. Accessory auricular appendages, particularly at the tragus, may appear as part of the oculo-auriculo-vertebral spectrum (also called Goldenhar syndrome, hemifacial microsomia, facio-auriculo-vertebral spectrum, and first and second branchial arch syndrome). (See "Syndromes with craniofacial abnormalities", section on 'Craniofacial microsomia (CFM)'.)
: Evidence-Based Answer. All newborns should be screened for hearing loss, whether or not they have preauricular skin lesions. Newborns with these anomalies may be at increased risk of hearing impairment. (Strength of Recommendation [SOR]: C, based on small observational studies and expert opinion.) Although there is a reported association between renal tract abnormalities and isolated preauricular skin lesions in infants, studies that have used renal ultrasonography to evaluate these patients are inconclusive. Physicians should not perform renal imaging on newborns with preauricular skin lesions unless they have other congenital malformations. (SOR: C, based on small, observational, disease-oriented studies.) From AAFP FPIN. In addition, external ear malformations often are associated with syndromes of multiple congenital anomalies that include renal malformations [14]. However, patients with isolated minor external ear anomalies (eg, preauricular skin tags or pits) do not appear to have a significant increased risk of renal anomalies. As a result, although controversial, routine renal imaging for patients with isolated minor ear abnormalities appears to be unnecessary unless accompanied by other major malformations or multiple congenital anomaly syndromes [15]. (See Congenital anomalies of the ear , section on Preauricular pits .) Children with preauricular pits or tags are at five times the risk of the general population for permanent hearing impairment [23]. Preauricular pits do not require surgery unless they become repeatedly infected or discharge squamous material (picture 4) [21]. If surgery is performed, it should include excision of the pit, the squamous-lined cyst usually present beneath the skin (picture 6), and the cartilage at the root of the helix en bloc to avoid recurrence (picture 7) [27]. Accessory auricular appendage/preauricular tag — Accessory hillocks composed of skin, subcutaneous fat, and/or cartilage may occur near the auricle or anywhere along the anterior border of the sternocleidomastoid muscle (picture 8). These accessory auricular appendages are called preauricular tags when they are present in the preauricular area. Such appendages usually are removed in childhood for cosmetic purposes. Children with accessory auricular appendages may have associated unilateral hearing loss [23]. They should have complete audiologic testing, preferably at birth. Accessory auricular appendages, particularly at the tragus, may appear as part of the oculo-auriculo-vertebral spectrum (also called Goldenhar syndrome, hemifacial microsomia, facio-auriculo-vertebral spectrum, and first and second branchial arch syndrome). (See Syndromes with craniofacial abnormalities , section on Craniofacial microsomia (CFM) .)")
27
Extra digits Polydactyly vs Syndactyly Tie off or leave? Associations?
Look for the Simian crease, Sandal toe Hands and feet − The hands and feet are inspected for syndactyly (fusion of digits) and polydactyly (extra digits). Syndactyly and polydactyly can be normal variants in a newborn with an otherwise normal exam or may be associated with various syndromes AFP Polydactyly The incidence of polydactyly (supernumerary digits of hands or feet) is the same in both sexes, with simultaneous polydactyly of the hands and feet present in about one third of cases.14 It is more common in blacks than whites (3.6 to 13 cases per 1,000 live births versus 0.3 to 1.3 cases per 1,000 live births, respectively).15 The primary cause of polydactyly is thought to be genetic. Polydactyly usually involves border digits, especially the fifth. Although some cases involve only a distal phalanx, other cases are much more complex, involving the entire digit, with duplication of nails, tendons, and vascular structures. Treatment of complex cases involving bone requires removal of duplicated structures, whereas cases involving soft tissue can be treated with only ligation sutures applied in the nursery. Surgery generally is performed at six to nine months of age, before the child is ambulatory but able to tolerate general anesthesia.10,15 Syndactyly Syndactyly (webbed toes or fingers) occurs in approximately one in 2,000 to 2,500 live births.15 There are various levels of syndactylization, from partial to complete. The most frequent site is between the second and third toes. Syndactyly is thought to be genetic, with an autosomal dominant pattern of inheritance. Simple syndactyly is more of a cosmetic problem than a functional one, and rarely requires treatment.10 A radiographic evaluation is not indicated unless radical treatment is being contemplated. If the parents desire surgery, it is advisable to wait until the child is old enough to take part in the decision and participate in postoperative care. The most common complication of the surgery is skin-flap slough, leading to a recurrence of the problem
 and polydactyly (extra digits). Syndactyly and polydactyly can be normal variants in a newborn with an otherwise normal exam or may be associated with various syndromes. AFP. Polydactyly. The incidence of polydactyly (supernumerary digits of hands or feet) is the same in both sexes, with simultaneous polydactyly of the hands and feet present in about one third of cases.14 It is more common in blacks than whites (3.6 to 13 cases per 1,000 live births versus 0.3 to 1.3 cases per 1,000 live births, respectively).15. The primary cause of polydactyly is thought to be genetic. Polydactyly usually involves border digits, especially the fifth. Although some cases involve only a distal phalanx, other cases are much more complex, involving the entire digit, with duplication of nails, tendons, and vascular structures. Treatment of complex cases involving bone requires removal of duplicated structures, whereas cases involving soft tissue can be treated with only ligation sutures applied in the nursery. Surgery generally is performed at six to nine months of age, before the child is ambulatory but able to tolerate general anesthesia.10,15. Syndactyly. Syndactyly (webbed toes or fingers) occurs in approximately one in 2,000 to 2,500 live births.15 There are various levels of syndactylization, from partial to complete. The most frequent site is between the second and third toes. Syndactyly is thought to be genetic, with an autosomal dominant pattern of inheritance. Simple syndactyly is more of a cosmetic problem than a functional one, and rarely requires treatment.10 A radiographic evaluation is not indicated unless radical treatment is being contemplated. If the parents desire surgery, it is advisable to wait until the child is old enough to take part in the decision and participate in postoperative care. The most common complication of the surgery is skin-flap slough, leading to a recurrence of the problem.")
28
Newborn Foot Metatarsus adductus
m/c, medial deviation forefoot Most resolve, exercises, rare splinting Positional calcaneovalgus feet (talipes calcaneovalgus) hyperdorsiflexion of the foot with the abduction of the forefoot Most resolve, exercises, splinting Clubfoot (talipes equinovarus) Most spontaneous, can be genetic manipulation that includes casting and bracing (referred to as the Ponseti method Metatarsus adductus is the most common congenital foot deformity [3,4]. It is characterized by medial deviation (adduction) of the forefoot while the hindfoot remains in a normal position, thus forming a "C" shape, or concavity of the medial aspect of the foot (picture 1). The reported incidence is about 1 to 2 per 1,000 live births and is increased in families with a history of metatarsus adductus [3,5]. It appears to occur more commonly in first-born children due to the increased molding effect from the primigravida uterus and abdominal wall. The incidence is higher in twin compared to singleton births but the frequency of metatarsus adductus appears to be similar in premature and term infants [6]. Clinical findings and assessment — Metatarsus adductus is characterized by medial deviation of the forefoot, which is usually slightly supinated while the hindfoot remains neutral. A deep medial crease is generally present. Metatarsus adductus is often bilateral; when unilateral, it occurs more often on the left than on the right (for unknown reasons) [7]. It is the most common cause of in-toeing gait in the infant [8]. In the walking child, abnormal shoe wear may occur. Positional calcaneovalgus feet, also referred to as talipes calcaneovalgus, is a common foot deformity [3]. It is characterized by hyperdorsiflexion of the foot with the abduction of the forefoot, which often results in the forefoot resting on the anterior surface of the lower leg (picture 2 and picture 3). External tibial torsion is a common associated finding. It is a deformity that is thought to be more common in first-born children due to the increased molding effects of the primigravida uterus. Differentiating calcaneovalgus feet, which is generally benign, from the following more severe conditions is mandatory [ Clubfoot (talipes equinovarus) refers to a developmental deformity of the foot in which one or both feet are excessively plantar flexed, with the forefoot swung medially and the sole facing inward. It occurs bilaterally in 30 to 50 percent of cases. We suggest an amniocentesis for karyotype if there are associated abnormalities or indications for invasive prenatal diagnoses (eg, abnormal maternal analytes), given the increased risk of aneuploidy. We perform amniocentesis in the setting of isolated clubfoot because associated abnormalities may not be detected by ultrasound and small numbers of karyotypic results from these cases limit the reliability of published estimates of risk. Runs in families.
 hyperdorsiflexion of the foot with the abduction of the forefoot. Most resolve, exercises, splinting. Clubfoot (talipes equinovarus) Most spontaneous, can be genetic. manipulation that includes casting and bracing (referred to as the Ponseti method. Metatarsus adductus is the most common congenital foot deformity [3,4]. It is characterized by medial deviation (adduction) of the forefoot while the hindfoot remains in a normal position, thus forming a C shape, or concavity of the medial aspect of the foot (picture 1). The reported incidence is about 1 to 2 per 1,000 live births and is increased in families with a history of metatarsus adductus [3,5]. It appears to occur more commonly in first-born children due to the increased molding effect from the primigravida uterus and abdominal wall. The incidence is higher in twin compared to singleton births but the frequency of metatarsus adductus appears to be similar in premature and term infants [6]. Clinical findings and assessment — Metatarsus adductus is characterized by medial deviation of the forefoot, which is usually slightly supinated while the hindfoot remains neutral. A deep medial crease is generally present. Metatarsus adductus is often bilateral; when unilateral, it occurs more often on the left than on the right (for unknown reasons) [7]. It is the most common cause of in-toeing gait in the infant [8]. In the walking child, abnormal shoe wear may occur. Positional calcaneovalgus feet, also referred to as talipes calcaneovalgus, is a common foot deformity [3]. It is characterized by hyperdorsiflexion of the foot with the abduction of the forefoot, which often results in the forefoot resting on the anterior surface of the lower leg (picture 2 and picture 3). External tibial torsion is a common associated finding. It is a deformity that is thought to be more common in first-born children due to the increased molding effects of the primigravida uterus. Differentiating calcaneovalgus feet, which is generally benign, from the following more severe conditions is mandatory [ Clubfoot (talipes equinovarus) refers to a developmental deformity of the foot in which one or both feet are excessively plantar flexed, with the forefoot swung medially and the sole facing inward. It occurs bilaterally in 30 to 50 percent of cases. We suggest an amniocentesis for karyotype if there are associated abnormalities or indications for invasive prenatal diagnoses (eg, abnormal maternal analytes), given the increased risk of aneuploidy. We perform amniocentesis in the setting of isolated clubfoot because associated abnormalities may not be detected by ultrasound and small numbers of karyotypic results from these cases limit the reliability of published estimates of risk. Runs in families.")
29
V-finger Test AFP A simple test that can raise the clinician's suspicions of MTA is the “V”-finger test (Figure 4). In this test, the heel of the foot is placed in the “V” formed by the index and middle fingers, and the lateral aspect of the foot is observed from a plantar side for medial or lateral deviation from the middle finger. Medial deviation from the middle finger at the styloid process indicates MTA.3 Treatment is based on the severity of the condition and is controversial. While some authors1 advocate only observation without active intervention for mild cases, others would intervene early in all severe cases or by two months of age, if the condition is not resolved.4 Other authors3 recommend treatment as soon as possible, especially in moderate to severe cases. Based on the natural course of the condition, a more conservative approach seems reasonable. Of MTA cases identified at birth, 85 to 90 percent resolve by one year of age.1,3 Another prospective study5 confirmed these findings—87 percent of MTA cases had resolved by six years of age, with only about 4 percent remaining at age 16. Mild (flexible, passively correctable) MTA requires only parental reassurance. Moderate (semi-flexible, reducible) MTA can be treated with stretching exercises at every diaper change. First, the heel is stabilized within the notch between the thumb and index finger. Then, the forefoot is slightly pulled distally, held between the thumb and index finger of the other hand, and gently pushed into a corrected position.1 For the majority of MTA cases, the prognosis is quite good. In severe cases, excessive compensation at the level of the mediotarsal joint can lead to the development of bunions, hammertoes, and other disorders.6 Therefore, severe (rigid) MTA can be referred for serial casting and bracing. Evidence-based comparisons of splinting or casting versus manipulation alone are not yet available.4
. In this test, the heel of the foot is placed in the V formed by the index and middle fingers, and the lateral aspect of the foot is observed from a plantar side for medial or lateral deviation from the middle finger. Medial deviation from the middle finger at the styloid process indicates MTA.3. Treatment is based on the severity of the condition and is controversial. While some authors1 advocate only observation without active intervention for mild cases, others would intervene early in all severe cases or by two months of age, if the condition is not resolved.4 Other authors3 recommend treatment as soon as possible, especially in moderate to severe cases. Based on the natural course of the condition, a more conservative approach seems reasonable. Of MTA cases identified at birth, 85 to 90 percent resolve by one year of age.1,3 Another prospective study5 confirmed these findings—87 percent of MTA cases had resolved by six years of age, with only about 4 percent remaining at age 16. Mild (flexible, passively correctable) MTA requires only parental reassurance. Moderate (semi-flexible, reducible) MTA can be treated with stretching exercises at every diaper change. First, the heel is stabilized within the notch between the thumb and index finger. Then, the forefoot is slightly pulled distally, held between the thumb and index finger of the other hand, and gently pushed into a corrected position.1. For the majority of MTA cases, the prognosis is quite good. In severe cases, excessive compensation at the level of the mediotarsal joint can lead to the development of bunions, hammertoes, and other disorders.6 Therefore, severe (rigid) MTA can be referred for serial casting and bracing. Evidence-based comparisons of splinting or casting versus manipulation alone are not yet available.4.")
30
Calcaneovalgus The axis of calcaneovalgus deformity is in the tibiotalar joint, where the foot is positioned in extreme hyperextension, with its dorsum frequently touching the distal leg. Females are affected more often than males, and this deformity can be unilateral or bilateral.3 It occurs in about 5 percent of all newborns5 and is associated with external rotation of the calcaneus, an overstretched Achilles tendon, and tight anterior leg musculature, all of which warrant treatment.11 On inspection, the foot has an “up and out” appearance, with the dorsal forefoot practically touching the anterior aspect of the ankle and lower leg (Figure 8). The ankle generally can be plantarflexed to only 90 degrees or less. Radiographs can confirm clinical diagnosis. Calcaneovalgus is a positional deformity that is highly amenable to treatment. According to some authors,10,12 it has an excellent natural history and can spontaneously resolve on its own. Others3 advocate a more aggressive approach because of the possibility of future complications, such as permanent muscle imbalance, peroneal tendon dislocation, and delayed ambulation. Generally, the more severe the limitation of ankle plantar flexion, the more treatment is warranted. Treatment should begin as early as possible. Mild cases can be treated with stretching exercises performed at each diaper change. Stretching consists of gentle plantarflexion of the foot with mild inversion for a count of 10, repeated three times. In moderate cases or when stretching fails to correct the deformity, splinting or firm, high-top, lace-up shoes that prevent dorsiflexion can be used. For severe deformities with significant limitation of ankle plantarflexion, serial mobilization casting is performed until corrected, followed by nightly maintenance use of a bivalved cast or splinting of the posterior aspect of the leg for a two- to 10-week course.3
. The ankle generally can be plantarflexed to only 90 degrees or less. Radiographs can confirm clinical diagnosis. Calcaneovalgus is a positional deformity that is highly amenable to treatment. According to some authors,10,12 it has an excellent natural history and can spontaneously resolve on its own. Others3 advocate a more aggressive approach because of the possibility of future complications, such as permanent muscle imbalance, peroneal tendon dislocation, and delayed ambulation. Generally, the more severe the limitation of ankle plantar flexion, the more treatment is warranted. Treatment should begin as early as possible. Mild cases can be treated with stretching exercises performed at each diaper change. Stretching consists of gentle plantarflexion of the foot with mild inversion for a count of 10, repeated three times. In moderate cases or when stretching fails to correct the deformity, splinting or firm, high-top, lace-up shoes that prevent dorsiflexion can be used. For severe deformities with significant limitation of ankle plantarflexion, serial mobilization casting is performed until corrected, followed by nightly maintenance use of a bivalved cast or splinting of the posterior aspect of the leg for a two- to 10-week course.3.")
31
Clubfoot Clubfoot is a complex, multifactorial deformity with genetic and intrauterine factors. One popular theory postulates that a clubfoot is a result of intrauterine maldevelopment of the talus that leads to adduction and plantarflexion of the foot.7 Clubfoot occurs in one to two per 1,000 live births; however, the incidence is higher in Hispanics and lower in Asians.8 On inspection, the “down and in” appearance of the foot, which somewhat resembles that of MTA, is obvious (Figure 5).3 The foot appears smaller, with a flexible, softer heel because of the hypoplastic calcaneus. The medial border of the foot is concave with a deep medial skin furrow, and the lateral border is highly convex. The heel is usually small and is internally rotated, making the soles of the feet face each other in cases of bilateral deformities. On testing, there is pronounced tightness of the Achilles tendon with very little dorsiflexion, which differentiates clubfoot from MTA (Figure 6). Radiographs of clubfeet usually reveal roughly parallel axes of the talus and calcaneus Clubfoot can be classified into extrinsic (supple) type, which is essentially a severe positional or soft tissue deformity; and intrinsic (rigid) type, where manual reduction is impossible. The type of clubfoot determines the specific therapy. Extrinsic clubfoot can be treated by serial casting, while intrinsic clubfoot eventually may require surgery. Plaster casting should be attempted on virtually all clubfeet, supple or rigid, as soon as practical. Casts initially are changed at semiweekly to weekly intervals and are continued until the deformity responds and is corrected fully. Persistent cast treatments by experienced clinicians have been reported to be successful in most patients.9 However, if a plateau is reached in treatment, surgery by a specialist in pediatric foot deformities should be considered, usually when the child is between six and nine months of age.10 The goal is to obtain a stable, “platform-like” position of the foot for future ambulation.
.3 The foot appears smaller, with a flexible, softer heel because of the hypoplastic calcaneus. The medial border of the foot is concave with a deep medial skin furrow, and the lateral border is highly convex. The heel is usually small and is internally rotated, making the soles of the feet face each other in cases of bilateral deformities. On testing, there is pronounced tightness of the Achilles tendon with very little dorsiflexion, which differentiates clubfoot from MTA (Figure 6). Radiographs of clubfeet usually reveal roughly parallel axes of the talus and calcaneus. Clubfoot can be classified into extrinsic (supple) type, which is essentially a severe positional or soft tissue deformity; and intrinsic (rigid) type, where manual reduction is impossible. The type of clubfoot determines the specific therapy. Extrinsic clubfoot can be treated by serial casting, while intrinsic clubfoot eventually may require surgery. Plaster casting should be attempted on virtually all clubfeet, supple or rigid, as soon as practical. Casts initially are changed at semiweekly to weekly intervals and are continued until the deformity responds and is corrected fully. Persistent cast treatments by experienced clinicians have been reported to be successful in most patients.9 However, if a plateau is reached in treatment, surgery by a specialist in pediatric foot deformities should be considered, usually when the child is between six and nine months of age.10 The goal is to obtain a stable, platform-like position of the foot for future ambulation.")
32
Sacral dimple When do you need an ultrasound?
If visible intact base-> OK If deep/large > 0.5cm, > 2.5cm from anus, or have tuft hair/vascular lesion -> Need u/s The spine is directly visualized and palpated along the vertebral column to detect abnormalities, such as a neural tube defect. Soft tissue masses along the spine that are covered with normal skin may be lipomas or myelomeningocele. The gluteal folds should be separated to determine whether or not a sacral cleft or dimple is present. A tuft of hair, hemangioma (picture 10), or discoloration in the sacrococcygeal area may suggest an underlying vertebral or spinal cord anomaly [28]. (See "Epidemiology, pathogenesis, clinical features, and complications of infantile hemangiomas" and "Evaluation and diagnosis of infantile hemangiomas", section on 'Lumbosacral'.) Sacral dimple — Sacral midline dimples in the skin overlying the coccyx, which have a visible intact base, are typically benign with little or no clinical significance [28-32]. In contrast, sacral dimples that are deep and large (greater than 0.5 cm), fall within the superior portion or above the gluteal crease (>2.5 cm from the anal verge), or are associated with other cutaneous markers for neural tube defects (eg, hypertrichosis, and discoloration), are more likely to be associated with an underlying neural tube defect [28,33]. If a sacral dimple has any of these characteristics, an ultrasound should be performed to screen for a neural tube defect [32,34].
, or discoloration in the sacrococcygeal area may suggest an underlying vertebral or spinal cord anomaly [28]. (See Epidemiology, pathogenesis, clinical features, and complications of infantile hemangiomas and Evaluation and diagnosis of infantile hemangiomas , section on Lumbosacral .) Sacral dimple — Sacral midline dimples in the skin overlying the coccyx, which have a visible intact base, are typically benign with little or no clinical significance [28-32]. In contrast, sacral dimples that are deep and large (greater than 0.5 cm), fall within the superior portion or above the gluteal crease (>2.5 cm from the anal verge), or are associated with other cutaneous markers for neural tube defects (eg, hypertrichosis, and discoloration), are more likely to be associated with an underlying neural tube defect [28,33]. If a sacral dimple has any of these characteristics, an ultrasound should be performed to screen for a neural tube defect [32,34].")
33
DDH-Click or Clunk? Algorithm AAP Exam (until age 2) U/s use
Ortolani and Barlow maneuvers Galeazzi and Klisic signs U/s use Referral for tx Triple diapers not recommended Pavlik harness AMERICAN ACADEMY OF PEDIATRICS Clinical Practice Guideline: Early Detection of Developmental Dysplasia of the Hip Pediatrics Vol. 105 No. 4 April 1, pp The accompanying algorithm gives an overview of the recommendations for DDH screening in infants. The following summarizes the AAP recommendations: All newborns should be screened by physical examination. Ultrasonography of all newborns is not recommended. Referral to an orthopedist is recommended if a positive Ortolani or Barlow test is found on the newborn examination. Ultrasonography is not recommended in infants with positive findings, nor is radiographic examination of the pelvis and hips. Developmental Dysplasia of the Hip The rightsholder did not grant rights to reproduce this item in electronic media. For the missing item, see the original print version of this publication. Figure The use of triple diapers in infants with physical signs suggestive of DDH during the newborn period is not recommended. The guideline notes that triple-diaper use is a common practice despite the lack of data on effectiveness. If the physical examination at birth reveals “equivocally” positive findings (i.e., a soft click, mild asymmetry, but no Ortolani or Barlow sign), a follow-up hip examination should be performed when the infant is two weeks of age. If the Ortolani or Barlow test is positive at the two-week examination, the infant should be referred to an orthopedist. Referral is deemed urgent but not an emergency. If the Ortolani or Barlow test is negative at the two-week examination but other physical findings raise the suspicion of DDH, consideration should be given to referring the infant to an orthopedist or obtaining ultrasonography at age three to four weeks. If the physical examination is negative at two weeks of age, follow-up is recommended at the scheduled well-baby periodic examinations. If the results of the newborn examination are negative, consideration may be given to risk factors for DDH. These risk factors include the following: female infants, a family history of DDH and breech presentation.
, a follow-up hip examination should be performed when the infant is two weeks of age. If the Ortolani or Barlow test is positive at the two-week examination, the infant should be referred to an orthopedist. Referral is deemed urgent but not an emergency. If the Ortolani or Barlow test is negative at the two-week examination but other physical findings raise the suspicion of DDH, consideration should be given to referring the infant to an orthopedist or obtaining ultrasonography at age three to four weeks. If the physical examination is negative at two weeks of age, follow-up is recommended at the scheduled well-baby periodic examinations. If the results of the newborn examination are negative, consideration may be given to risk factors for DDH. These risk factors include the following: female infants, a family history of DDH and breech presentation.")
34
Screening for developmental hip dysplasia—clinical algorithm.
Screen all infants by trained health-care professional. Ultrasonography of all newborns is not recommended. 2. If a positive Ortolani or Barlow sign is found in the newborn examination, the infant should be referred to an orthopaedist. If the results of the physical examination at birth are “equivocally” positive (ie, soft click, mild asymmetry, but neither an Ortolani nor a Barlow sign is present), then a follow-up hip examination by the pediatrician in 2 weeks is recommended. 3. If the results of the newborn physical examination are positive (ie, presence of an Ortolani or a Barlow sign), ordering an ultrasonographic examination of the newborn is not recommended. If the results of the newborn physical examination are positive, obtaining a radiograph of the newborn's pelvis and hips is not recommended. The use of triple diapers when abnormal physical signs are detected during the newborn period is not recommended. 7. Risk factors. If the results of the newborn examination are negative (or equivocally positive), risk factors may be considered. Girl, FHX, Breech Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip Pediatrics 2000;105: ©2000 by American Academy of Pediatrics
, then a follow-up hip examination by the pediatrician in 2 weeks is recommended. 3. If the results of the newborn physical examination are positive (ie, presence of an Ortolani or a Barlow sign), ordering an ultrasonographic examination of the newborn is not recommended. If the results of the newborn physical examination are positive, obtaining a radiograph of the newborn s pelvis and hips is not recommended. The use of triple diapers when abnormal physical signs are detected during the newborn period is not recommended. 7. Risk factors. If the results of the newborn examination are negative (or equivocally positive), risk factors may be considered. Girl, FHX, Breech. Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip Pediatrics 2000;105: ©2000 by American Academy of Pediatrics.")
35
It’s a Boy or Girl? Vaginal skin tags, discharge
Hydroceles vs inguinal hernias transillumination Undescended testicle 2-5% at term When to refer? Hypospadias, epispadias Ambiguous The vaginal opening should be fully visible. Many infants have vaginal skin tags, representing the slight protrusion of vaginal epithelium at the posterior fourchette. Withdrawal from maternal hormones often results in a milky white vaginal discharge, which sometimes is blood-tinged. Female — In the female infant, the size and location of the labia, clitoris, meatus, and vaginal opening should be assessed. The appearance of the genitalia varies with gestational age. The labia minora and clitoris are prominent in preterm infants, while the labia majora becomes larger as the infant approaches term. Male — The presence of testes, size of the penis, appearance of the scrotum, and the position of the urethral opening should be evaluated. Testes should be palpable in the scrotum or inguinal canal, and be equal in size. Between 2 and 5 percent of full term and 30 percent of premature male infants are born with an undescended testicle. Testes descend before six months of age in most cases. (See "Undescended testes (cryptorchidism) in children: Clinical features and evaluation", section on 'Epidemiology and risk factors' and "Undescended testes (cryptorchidism) in children: Overview of management", section on 'Natural history'.) The penis is stretched to assess length. Normal penile length in the term male is 2.5 to 3.5 cm (figure 4) [27]. The scrotum of the term male is rugated and pigmented. Enlargement or swelling of the scrotum may be caused by hydroceles, hernias, or, rarely, testicular torsion. Hydroceles are fluid collections around the testes, and usually resolve spontaneously. They can be distinguished from hernias by transillumination of the scrotum. AFP Inguinal Hernia and Hydrocele in Newborns Inguinal hernia Incidence: term newborns, 0.5% to 1%; premature newborns, 5% to 10%; location on right side (∼60%), left side (40%), or both sides (10%), with bilateral hernias more common in premature newborns (∼62% of affected infants) Clinical features: soft, nontender, reducible bulge in the inguinal canal, off the midline, especially at times of increased intra-abdominal pressure, with possible extension into scrotum; when incarcerated, tenderness and tenseness of hernia, with discoloration of overlying skin Complications: incarceration and strangulation Treatment: elective surgical repair as soon as possible after diagnosis13 Hydrocele Clinical features: painless, tense, fluctuant scrotal mass that transilluminates; upper border usually movable away from inguinal canal; possibly, testis not palpable Treatment: none usually needed, because hydroceles generally decrease in size and resolve over the first year of life; if not resolved by the age of 1 to 2 years, consideration of elective surgical repair; for communicating hydrocele (i.e., one that fluctuates in size), same treatment as for inguinal hernia
 in children: Clinical features and evaluation , section on Epidemiology and risk factors and Undescended testes (cryptorchidism) in children: Overview of management , section on Natural history .) The penis is stretched to assess length. Normal penile length in the term male is 2.5 to 3.5 cm (figure 4) [27]. The scrotum of the term male is rugated and pigmented. Enlargement or swelling of the scrotum may be caused by hydroceles, hernias, or, rarely, testicular torsion. Hydroceles are fluid collections around the testes, and usually resolve spontaneously. They can be distinguished from hernias by transillumination of the scrotum. AFP. Inguinal Hernia and Hydrocele in Newborns. Inguinal hernia. Incidence: term newborns, 0.5% to 1%; premature newborns, 5% to 10%; location on right side (∼60%), left side (40%), or both sides (10%), with bilateral hernias more common in premature newborns (∼62% of affected infants) Clinical features: soft, nontender, reducible bulge in the inguinal canal, off the midline, especially at times of increased intra-abdominal pressure, with possible extension into scrotum; when incarcerated, tenderness and tenseness of hernia, with discoloration of overlying skin. Complications: incarceration and strangulation. Treatment: elective surgical repair as soon as possible after diagnosis13. Hydrocele. Clinical features: painless, tense, fluctuant scrotal mass that transilluminates; upper border usually movable away from inguinal canal; possibly, testis not palpable. Treatment: none usually needed, because hydroceles generally decrease in size and resolve over the first year of life; if not resolved by the age of 1 to 2 years, consideration of elective surgical repair; for communicating hydrocele (i.e., one that fluctuates in size), same treatment as for inguinal hernia.")
36
The Undescended Testicle: Diagnosis and Management
STEVEN G. DOCIMO, M.D., University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania RICHARD I. SILVER, M.D., Jefferson Medical College of Thomas Jefferson University, Philadelphia, Pennsylvania WILLIAM CROMIE, M.D., University of Chicago Pritzker School of Medicine, Chicago, Illinois Am Fam Physician. 2000 Nov 1;62(9): INDICATIONS FOR REFERRAL — Indications for referral in phenotypic males with cryptorchidism include: Phenotypically male newborn infants with bilateral nonpalpable testes, unilateral nonpalpable testis with hypospadias, or suspected disorder of sexual development (including congenital adrenal hyperplasia) – Immediate consultation with or referral to a multidisciplinary team (see "Management of the infant with ambiguous genitalia", section on 'Initial stabilization') Bilateral nonpalpable testes in boys beyond infancy – Referral for exploratory surgery (as an initial step, some clinicians may perform a hormonal evaluation to exclude absent testes) (see "Undescended testes (cryptorchidism) in children: Clinical features and evaluation", section on 'Older child') Congenital unilateral nonpalpable testis – Referral for examination under anesthesia and exploratory surgery, ideally between 6 and 12 months (see 'Nonpalpable testes' below) Congenital palpable undescended testis (unilateral or bilateral) in infants – Referral for evaluation and possible orchiopexy, ideally between 6 and 12 months (see 'Palpable testes' below) Ascending testis in boys beyond infancy – Referral for evaluation and possible orchiopexy whenever the physical examination change is noted (see 'Timing of surgery' below) Palpable tissue in the scrotum that is thought to be an atrophic testis – Referral for exploratory surgery to exclude an intraabdominal testis [9] (see 'Exploratory surgery' below) Difficulty differentiating between undescended, retractile, or ectopic testis (at any age) – Refer for evaluation and possible orchiopexy, ideally between 6 and 12 months Timing of surgery — Surgical treatment of undescended testes is recommended as soon as possible after six months of age for congenitally undescended testes and definitely should be completed before the child is two years old [22,69-71]. In children with testicular ascent later in childhood, surgery generally should be performed within six months of identification. Spontaneous descent rarely, if ever, occurs after six months of age [11]. Treatment before two years (ideally before one year) of age is associated with improved testicular growth and fertility potential [39,44,52-54]. (See 'Natural history' above and 'Subfertility' above.) Nonpalpable testes Imaging — Imaging is not routinely warranted to locate nonpalpable testes. Imaging studies lack the sensitivity and the specificity to alter the need for exploratory surgery [74,76]. (See "Undescended testes (cryptorchidism) in children: Clinical features and evaluation", section on 'Imaging'.)
: INDICATIONS FOR REFERRAL — Indications for referral in phenotypic males with cryptorchidism include: Phenotypically male newborn infants with bilateral nonpalpable testes, unilateral nonpalpable testis with hypospadias, or suspected disorder of sexual development (including congenital adrenal hyperplasia) – Immediate consultation with or referral to a multidisciplinary team (see Management of the infant with ambiguous genitalia , section on Initial stabilization ) Bilateral nonpalpable testes in boys beyond infancy – Referral for exploratory surgery (as an initial step, some clinicians may perform a hormonal evaluation to exclude absent testes) (see Undescended testes (cryptorchidism) in children: Clinical features and evaluation , section on Older child ) Congenital unilateral nonpalpable testis – Referral for examination under anesthesia and exploratory surgery, ideally between 6 and 12 months (see Nonpalpable testes below) Congenital palpable undescended testis (unilateral or bilateral) in infants – Referral for evaluation and possible orchiopexy, ideally between 6 and 12 months (see Palpable testes below) Ascending testis in boys beyond infancy – Referral for evaluation and possible orchiopexy whenever the physical examination change is noted (see Timing of surgery below) Palpable tissue in the scrotum that is thought to be an atrophic testis – Referral for exploratory surgery to exclude an intraabdominal testis [9] (see Exploratory surgery below) Difficulty differentiating between undescended, retractile, or ectopic testis (at any age) – Refer for evaluation and possible orchiopexy, ideally between 6 and 12 months. Timing of surgery — Surgical treatment of undescended testes is recommended as soon as possible after six months of age for congenitally undescended testes and definitely should be completed before the child is two years old [22,69-71]. In children with testicular ascent later in childhood, surgery generally should be performed within six months of identification. Spontaneous descent rarely, if ever, occurs after six months of age [11]. Treatment before two years (ideally before one year) of age is associated with improved testicular growth and fertility potential [39,44,52-54]. (See Natural history above and Subfertility above.) Nonpalpable testes. Imaging — Imaging is not routinely warranted to locate nonpalpable testes. Imaging studies lack the sensitivity and the specificity to alter the need for exploratory surgery [74,76]. (See Undescended testes (cryptorchidism) in children: Clinical features and evaluation , section on Imaging .)")
37
Gomco Circumcision Q’s
If don’t get circumcised- do they have to retract foreskin and clean? No, just clean like rest of body Potential Benefits Potential complications When to call urology? UTD POTENTIAL BENEFITS — Circumcision has been associated with a number of medical benefits, including lower rates of urinary tract infection (UTI), penile cancer (partners lower risk of cervical cancer), penile inflammation, penile dermatoses, and sexually transmitted infections [18,19]. A lower rate of UTI is the major benefit during infancy. The rate of procedure-related complications during and after circumcision is approximately 2 to 5 per 1000 cases Most common are bleeding and infection Surgical complications are less common and include the following: Urethral complications, including urethrocutaneous fistulas and urethral meatal stenosis (see 'Urethral complications' above) Glans injury including penile amputation (see 'Glans injury' above) Removal of excessive skin that may result in a denuded penile shaft (see 'Excessive skin removal' above) Inadequate skin removal that may result in an unsatisfactory cosmetic appearance Epidermal inclusion cyst Adhesions can vary from mild adhesions of tiny areas of fusion between the foreskin and corona, which can be treated conservatively, to dense adhesions (also referred to as skin bridges) that may cause tethering of the penis and usually require surgical lysis (see 'Minor adhesions' above and 'Skin bridges' above) Cicatrix is a circumferential scar that usually develops at the incision line and is often associated with a hidden penis (see 'Cicatrix' above) Anesthetic complications of circumcision are reviewed separately Only about 4 percent of males have a completely retractable foreskin at birth, and in more than half of newborn males, the foreskin cannot be retracted far enough to visualize the urethral meatus
, penile cancer (partners lower risk of cervical cancer), penile inflammation, penile dermatoses, and sexually transmitted infections [18,19]. A lower rate of UTI is the major benefit during infancy. The rate of procedure-related complications during and after circumcision is approximately 2 to 5 per 1000 cases. Most common are bleeding and infection. Surgical complications are less common and include the following: Urethral complications, including urethrocutaneous fistulas and urethral meatal stenosis (see Urethral complications above) Glans injury including penile amputation (see Glans injury above) Removal of excessive skin that may result in a denuded penile shaft (see Excessive skin removal above) Inadequate skin removal that may result in an unsatisfactory cosmetic appearance. Epidermal inclusion cyst. Adhesions can vary from mild adhesions of tiny areas of fusion between the foreskin and corona, which can be treated conservatively, to dense adhesions (also referred to as skin bridges) that may cause tethering of the penis and usually require surgical lysis (see Minor adhesions above and Skin bridges above) Cicatrix is a circumferential scar that usually develops at the incision line and is often associated with a hidden penis (see Cicatrix above) Anesthetic complications of circumcision are reviewed separately. Only about 4 percent of males have a completely retractable foreskin at birth, and in more than half of newborn males, the foreskin cannot be retracted far enough to visualize the urethral meatus.")
38
Discharge Instructions
Properly feeding the infant Instruction on proper breastfeeding position, attachment, and adequacy of swallowing Breastfeeding mothers should consult their physicians before taking any new medications. Parents should not give their infant supplemental water or honey. Breastfed and bottle-fed infants receiving less than 500 mL of formula per day should receive 200 IU of a vitamin D supplement per day. Urination patterns Six or more wet diapers per day is normal for a breastfed infant after the mother’s milk has come in, as well as for bottle-fed infants. Bowel movements More than three bowel movements per day is normal in breastfed infants. Bottle-fed infants may have fewer bowel movements. Umbilical cord care Instruction on proper cleaning Skin care Review of common rashes Genital care Instruction on proper care of circumcised or uncircumcised penises, as well as care of newborn girls’ genitals Signs of illness Rectal temperature of 100.5˚F (38˚C) or higher Signs of dehydration, lethargy, poor feeding Prevention of sudden infant death syndrome Instruction on properly positioning the infant for sleep Discharge Checklist for Healthy Newborns handout
 or higher. Signs of dehydration, lethargy, poor feeding. Prevention of sudden infant death syndrome. Instruction on properly positioning the infant for sleep. Discharge Checklist for Healthy Newborns. handout.")
39
Discharge Instructions, cont..
Parental smoking cessation Car seat selection and proper use See Table 2 Follow-up appointment made at discharge Infants younger than 24 hours, follow up within 72 hours of age Infants 24 to 48 hours of age, follow up within 96 hours of age Infants older than 48 hours, follow up within 120 hours of age

Similar presentations