Download presentation
Presentation is loading. Please wait.

1
Using Care Groups for Behavior Change in Nutrition and Health Tom Davis, MPH TOPS Senior Specialist for SBC

2
Session Objectives Participants will be able to: 1.Explain the impact of behavior change on child mortality. 2.Define Care Groups and name Care Group characteristics. 3.Explain the main result areas of Care Groups. 4.Explain the rationale behind each of the Care Group criteria. 5.List the main processes and tools used with Care Groups (Beneficiary Planning Sheet, major programmatic inputs, forming/working with CDCs, incentives, visual aids, lesson plans, worldview messages, stories, the ASPIRE method, formative research [BA and LDM Studies], Mini-KPCs, and other Care Group monitoring tools.) Five-day trainings on Care Groups and other coverage strategies will be provided in 2012/2013 for FS implementers: Three Regional Trainings and Six Country-level Trainings.
 Five-day trainings on Care Groups and other coverage strategies will be provided in 2012/2013 for FS implementers: Three Regional Trainings and Six Country-level Trainings..")
3
The Care Group Strategy: A Strategy for Rapid, Equitable and Lasting Impact for Maternal and Child Health Programs By Carolyn Wetzel (FH Director of Health Programs ) and Tom Davis Jr. (Senior Specialist for SBC, TOPS Project)
.")
4
The Goal of Care Groups Create a system whereby volunteer Community Health Workers can sustainably do effective behavior change with pregnant women and mothers of children 0-23m Reduce U5MR, MMR, and malnutrition to contribute to the accomplishment of MDGs: 1:Eradice extreme hunger and poverty 3: Promoter Gender Equality & Empower Women 4: Reduce child mortality rates 5: Improve maternal health 6: Combat HIV/AIDS, malaria and other diseases

5
Household-level Behavior Change is Key A major key to successful and sustainable community health interventions is household-level behavior change. Improvements in health facilities, the quality of care provided in health facilities and the availability of commodities are important to community health. However… These factors will not lead to long-term impact on health outcomes unless there are innovative delivery strategies using evidence-based, community-informed solutions that lead to individual behavior change.

6
Do you agree? A child death is a food security failure

7
Cumulative Impact of Household Behavior Change Interventions on Child Mortality Reduction: 13% 7% 6% 5% 4% 3% 2% 15% 57% Jones G, Steketee R, Bhutta Z, Morris S. and the Bellagio Child Survival Study Group. "How many child deaths can we prevent this year?" Lancet 2003; 362: 65-71.

8
What are Care Groups? Developed by Dr. Pieter Ernst with World Relief/ Mozambique, and pioneered by FH and WR for the past decade. Now used by at least 22 organization in 20 countries. Focuses on building teams of volunteer women who represent, serve, and do health promotion with blocks of <15 households each A community-based strategy for improving coverage and behavior change

9
15 minute mark

10
Small Group Activity: Care Group Criteria Divide into groups of about 5 people. Go through the Care Group Criteria Small Group Questions. Write your responses on newsprint. Small groups will report out responses when we come back to plenary. 30 mins for this small group work. You don’t have to finish all questions.

11
60 minute mark

12
This example: “9x12x14 structure” 1 Supervisor

13
CGV #10 CGV #1 CGV #7 CGV #11 CGV #12 CGV #4 CGV #2 CGV #3 CGV #9 CGV #8 CGV #6 CGV #5 Care Group Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #1 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #12 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #11 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #10 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #9 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #8 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #7 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #6 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #5 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #4 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #3 Mum #10 Mum #1 Mum #7 Mum #11 Mum #12 Mum #4 Mum #2 Mum #3 Mum #9 Mum #8 Mum #6 Mum #5 Small Group #2 CGV #1 CGV #2 CGV #3 CGV #4 CGV #5 CGV #6 CGV #7 CGV #8 CGV #9 CGV #10 CGV #11 CGV #12 Prom

14
Who is Using Care Groups? International Aid International Medical Corps International Rescue Committee International Rescue Committee Medical Teams Interenational Medical Teams Interenational Pathfinder PLAN Salvation Army World Service Salvation Army World Service Save the Children World Relief World Vision ACDI/VOCA ADRA Africare American Red Cross CARE Concern Worldwide Catholic Relief Services Curamericas Emmanuel International Food for the Hungry Future Generations GOAL

15
Where are Care Groups being Used? Bangladesh Bolivia Burkina Faso Burundi Cambodia DRC Ethiopia Guatemala Haiti Indonesia Kenya Liberia Malawi Mozambique Niger Peru Philippines Rwanda Sierra Leone Zambia

16
What works in behavior change? Findings from Powerful to Change Studies CORE SBCWG compared low and high performers for several behaviors (e.g., exclusive BF, hand washing with soap) – what works? 1. 1. Using formative research (e.g., positive deviance studies, Barrier Analysis, Trials of Improved Practices) to find the determinants of behaviors and to choose the right messages/activities; and 2. 2. Using a comprehensive coverage strategy: Using systematic home visitation or Care Groups to reach almost all beneficiaries very often (e.g., 95% every two weeks).
 – what works Using formative research (e.g., positive deviance studies, Barrier Analysis, Trials of Improved Practices) to find the determinants of behaviors and to choose the right messages/activities; and Using a comprehensive coverage strategy: Using systematic home visitation or Care Groups to reach almost all beneficiaries very often (e.g., 95% every two weeks)..")
17
Care Groups Outperform in Behavior Change: Indicator Gap Closure: Care Group Projects vs. CSHGP Average Gap closure range for Care Group projects: ~35 – 70% (Avg = 57% ) Gap closure range in non-CG projects ~25 – 45% (Avg. = 37%)
 Gap closure range in non-CG projects ~25 – 45% (Avg. = 37%).")
18
Care Groups and Estimated Reduction in Child Deaths

19
Target 60% Care Groups Can Bring about Rapid and Significant Changes in BF Behavior (22m)
")
20
Care Groups Can Bring about Rapid and Significant Changes in Health Service Coverage Target 75%

21
Target 80% Care Groups Can Bring about Rapid and Significant Changes in Feeding Behavior

22
Care Groups Can Bring about Significant Changes in Feeding Behavior 80% of these are statistically-significant changes

23
Source: Moz MOH Care Groups Can Bring about Rapid and Significant Changes in Health Service Utilization (FH/Moz)
")
24
Over a five year period 34% reduction 22% reduction Over a 20 month period Care Groups Can Bring about Rapid and Significant Changes in Impact (Underweight reduction, Feb ‘06-July ’10, FH/Moz)
")
25
Previous Title II Care Group Program, Mozambique Moderate & Severe Stunting (25% decrease [p<0.05])...
![Previous Title II Care Group Program, Mozambique Moderate & Severe Stunting (25% decrease [p<0.05])...](http://images.slideplayer.com/12/3527720/slides/slide_25.jpg "Previous Title II Care Group Program, Mozambique Moderate & Severe Stunting (25% decrease [p<0.05])...")
26
Severe Stunting (48% decrease [p<0.05])...
![Severe Stunting (48% decrease [p<0.05])...](http://images.slideplayer.com/12/3527720/slides/slide_26.jpg "Severe Stunting (48% decrease [p<0.05])...")
27
What about sustainability?? The plan: Interventions phased in then responsibilities slowly shifted from project-paid Promoters to MOH staff or Care Group leaders. Actuality: CG Volunteers continue home visits on their own, and sometimes meet together. WR Data from Gaza Province, Mozambique: 93% of the 1,457 volunteers active at the end of WR’s Care Group project were active meeting with mothers or doing home visits with flipchart 20 months after end of project. Out of the vacant roles, communities replaced 1/3 of them and trained them on their own. Changes brought about in the original program were maintained: A full 45 months after the end of the project (all interventions and funding ceased), final program goals on eight key indicators continued to be exceeded.
, final program goals on eight key indicators continued to be exceeded..")
28
Sustainability of Final Indicator Levels Four-Years Post-Project in the WR-Mozambique Care Group Project: Home Care of Sick Children (Note: Black line is project goal. Red line is actual indicator levels.) End of Project 45m post- project
 End of Project 45m post- project.")
29
Sustainability of Final Indicator Levels Four-Years Post-Project (WR-Mozambique Care Group Project): Preventive Services End of Project 45m post- project
: Preventive Services End of Project 45m post- project")
30
85 minute mark

31
Small Group Brainstorm Divide into same small groups and brainstorm a list of WHY you think Care Groups are outperforming other behavior change methods. This list can include anything that we can/should apply to other behavior change approaches. 15 mins for this small group work.

32
115 minute mark

33
Time Contribution (in hours) by Type of Project Staff FH/Mozambique Care Group Project October 2005 – September 2010 80% of the work was done by Care Group Volunteers, and 97% by community members (CGVs + Promoters). Community driven …

34
Other Care Group Best Practices Have the neighbors in the 5-14 households that the CGV will serve (visit and teach) elect the CGV. Contact with beneficiary mothers by the CGV can be through group meetings but also through individual home visits. (In FH/Moz CG Project, 70% of CGVs had contact with their mothers mostly or exclusively in group settings, and 30% had contact with beneficiary mothers mostly/exclusively through individual home visits.) Regardless, home visits are made to meeting defaulters. Groups should be facilitated by paid Promoters or other health/nutrition staff.
 Regardless, home visits are made to meeting defaulters. Groups should be facilitated by paid Promoters or other health/nutrition staff..")
35
Other Care Group Best Practices Care Group Volunteers should not be paid, but only receive very infrequent small non-monetary incentives like wrap-around skirts every two years. Respect is probably the most important incentive. (See www.CareGroupInfo.org) Turnover of Care Group Promoters and Volunteers has generally been very low when incentives are used in this way. Training of Care Group members should be done in the community (at low cost). A Care Group Promoter
. A Care Group Promoter.")
36
Other Care Group Best Practices Messages – including gender messaging – should also be communicated to other family members, daughters in particular. Changes in relationships and gender- based violence are sometimes seen. Low Cost: By using this cascading structure, for the entire FH/Mozambique CG project, the cost per beneficiary per year was USD $2.78. (The cpb range for nine CG projects was $2.78 - $7.91; average was $5.77.) A Beneficiary Mother
 A Beneficiary Mother.")
37
Selected Gender Indicators measured in the Care Group O.R. KPC Mother Leader % of CGVs who say they have gained more respect from.. since they began participating in the project … from health facility personnel 25% …from their extended family 41% … from their parents or husbands’ parents 48% … from their husbands 61% … from their community leaders 64% … from their mothers / other women / mother beneficiaries 100% % of CGVs who say that it is okay for a husband to hit his wife if he is not satisfied with her (final level shown; baseline was ~64%) 3% Gender Equity Improvements: Respect Wetzel, C, Davis Jr., T. Results of Care Group Operational Research conducted April to May 2010 as part of the project: Achieving Equity, Coverage, and Impact through a Care Group Network. Funded by USAID, Cooperative Agreement: GHS- A-00-05-00014-00.
 3% Gender Equity Improvements: Respect Wetzel, C, Davis Jr., T. Results of Care Group Operational Research conducted April to May 2010 as part of the project: Achieving Equity, Coverage, and Impact through a Care Group Network. Funded by USAID, Cooperative Agreement: GHS- A")
38
125 minute mark

39
How can your Organization Use Care Groups?

40
Design and Implementation of Care Groups Projects By Carolyn Wetzel (FH Director of Health Programs ) and Tom Davis Jr. (Senior Specialist for SBC, TOPS Project)
.")
41
“How To” Topics Major Programmatic Inputs Use of the Care Group Beneficiary Worksheet Use of Community Development Committees Use of visual aids Use of worldview messages Use of lesson plans Use of stories Use of the ASPIRE health promotion method Use of formative research Use of Mini-KPC surveys NOTE: The Care Group Difference manual is available at CORE Group website and www.CareGroupInfo.org.www.CareGroupInfo.org Three Coverage Strategies / Care Group Regional Trainings and six country-level trainings to be offered by TOPS in the coming years (beginning FY13).
.")
42
What you Need: Major Programmatic Inputs One paid Promoter minimum (7 th grade education or higher) per 2,016 beneficiary households, and one Supervisor (nurse) per 7-10 Promoters. 4-5 day training on each module (module taught in Care Groups in a 2-3m period), 3-4 trainings/year for first two years. Often 8-12 modules. C-IMCI training, optional. Color health promotion materials (e.g., flipcharts or cards) for Promoters and CGVs, bicycles for Promoters, Motorcycles for Supervisors, and some supplies for beneficiaries (e.g., vitamin A, deworming meds). One Program Manager, 0.5 FTE M&E staff, 1 FTE Trainer is helpful, 0.25-0.75 FTE HQ backstop is common. MOH involvement (coordination, joint supervision, etc.) is very helpful and may increase sustainability.
, 3-4 trainings/year for first two years. Often 8-12 modules. C-IMCI training, optional. Color health promotion materials (e.g., flipcharts or cards) for Promoters and CGVs, bicycles for Promoters, Motorcycles for Supervisors, and some supplies for beneficiaries (e.g., vitamin A, deworming meds). One Program Manager, 0.5 FTE M&E staff, 1 FTE Trainer is helpful, FTE HQ backstop is common. MOH involvement (coordination, joint supervision, etc.) is very helpful and may increase sustainability..")
43
Planning Care Group Staffing/Volunteers Click to Open

44
Forming or working with Community Development Committees Formed in each area with a Care Group – comprised of men, women, religious leaders, political leaders, etc. Try to include at least one CGV if not one from each CGV in the area. Leadership training provided, often includes Participatory Rural Appraisal and the development of a community workplan. Role: – Taking responsibility and ownership in planning and implementing community development activities – Encouraging and supporting existing community groups (Care Groups, Farmer Field School groups, others) – Advocacy for community needs to wider community and district governance structures May require additional staffing
 – Advocacy for community needs to wider community and district governance structures May require additional staffing.")
45
Purpose of Visual Aids used in Care Groups Purpose of the visual aids is NOT primarily to teach new facts, but to change BEHAVIOR and help GUIDE THE CGV in what they promote. To assure this happens, you should: – Teach Promoters and CGVs in the use of simple non-formal education techniques, and – Conduct Formative Research to modify the curricula according to (1) what is driving malnutrition and (2) what barriers exist to behavior change.
 what is driving malnutrition and (2) what barriers exist to behavior change..")
46
Use of Worldview Messages Worldview messages relate to how one views life including the environment, germs and people, and can block people from practicing healthy behaviors. Teaching people new prevention practices sometimes will not be enough – sometimes new perspectives on life are needed. Example: “I can change, and I can and should be an agent of change in my community.”

47
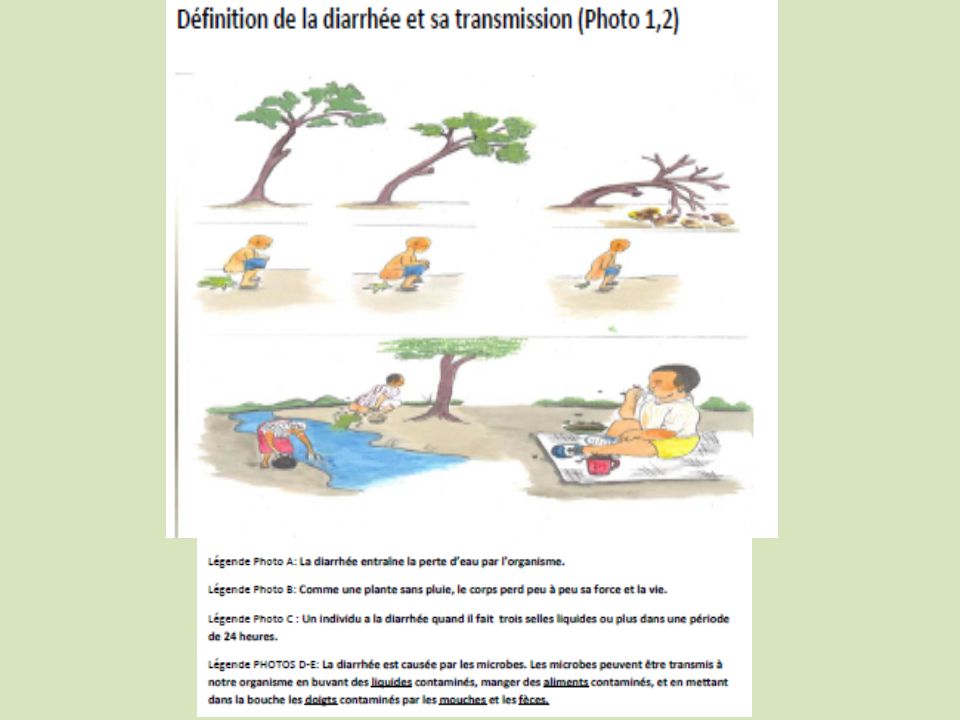
What is done in the CG Meeting? Example Lesson Plan Outline Game (e.g., Germ in the Circle; blindfolded tag game) Take attendance and Troubleshooting Share the story and ask about current practices: Hardship (boy’s name) Has Diarrhea Show pictures and share key messages on flipchart pages 6-11 about diarrhea transmission, care and treatment. Activity: Dehydration Demonstration (with water in bag) Probe about possible barriers and help them to find solutions (inform) Practice with flipchart and Coaching in a small group Request a commitment Examine previously promoted practices (e.g., going to a GM/P post).
 Take attendance and Troubleshooting Share the story and ask about current practices: Hardship (boy’s name) Has Diarrhea Show pictures and share key messages on flipchart pages 6-11 about diarrhea transmission, care and treatment. Activity: Dehydration Demonstration (with water in bag) Probe about possible barriers and help them to find solutions (inform) Practice with flipchart and Coaching in a small group Request a commitment Examine previously promoted practices (e.g., going to a GM/P post)..")
49
Use of Open-ended Stories Open-ended stories are usually used in FH’s Care Groups. The ending is provided by the participants. Open-ended stories get people to imagine their response to a situation, and to reflect on what they know and believe. Open-ended stories help people to talk about difficult situations without people taking the discussion personally. Consider using a wise mother and a new mother in stories. Lessons usually begin with a story: Usually Mother B practicing an unhealthy behavior or having a problem and needing help. The discussion after the story gives participants a chance to discuss Mother B’s behavior and give her advice.

51
Non-formal education techniques: The ASPIRE Method A– Ask about mothers’ current practices based on a discussion about Mother B’s situation. S – Show/Share key messages from the flipchart pages. P – Probe, asking the mothers and families what they think about these practices and barriers to adoption. Is there anything that would prevent you from doing [these practices]? I – Inform them of ways to overcome the barriers mentioned; clarify misunderstandings. R – Request a verbal commitment to the new practices (however, they can say NO – it is their choice to decide; don’t’ ask unless they sound interested). E – Evaluate their past behaviors related to the last session – sees how they are doing keeping these commitments.
. E – Evaluate their past behaviors related to the last session – sees how they are doing keeping these commitments..")
52
How ASPIRE is Integrated into the Lesson Plan Section nameTime needed for this section Game Attendance and Troubleshooting Ask about current practices after Story (pic. 1) Show/share key msgs and Explain (picture 2) Show and Explain (pic.3) Show and Explain (picture 4) Activity (e.g., demonstration) Probe (about ideas on behavior and barriers) Inform(on ways to overcome barriers) Practice and Coaching Request (a commitment) Examine (previously promoted practices) 10 minutes 15 minutes 10 minutes 5 minutes 15 minutes 10 minutes 5 minutes 20 minutes 2 minutes 5 minutes 1 hour, 50 minutes
 Show/share key msgs and Explain (picture 2) Show and Explain (pic.3) Show and Explain (picture 4) Activity (e.g., demonstration) Probe (about ideas on behavior and barriers) Inform(on ways to overcome barriers) Practice and Coaching Request (a commitment) Examine (previously promoted practices) 10 minutes 15 minutes 10 minutes 5 minutes 15 minutes 10 minutes 5 minutes 20 minutes 2 minutes 5 minutes 1 hour, 50 minutes.")
53
Ask about mothers’ current practices Show/Share key messages Probe mother’s ideas and barriers Request a verbal commitment Pictures in Flipchart Remind CGV of ASPIRE Steps

54
Alternative to ASPIRE 1.Ask about Current Behaviors 2.Show/Share key messages 3.Prober for Barriers 4.Request Commitments

55
Using the Curricula See Sample Care Group Lesson Plan List Handout – Many lesson plans available on curricula page of www.CareGroupInfo.org. www.CareGroupInfo.org In most Care Group projects one lesson is covered every two weeks, so if you have six lessons in a module it will take three months to teach the module. In rural areas, seasons of rain or harvest may affect the ability of Care Groups to meet. It is recommended that your teaching schedule be adapted to allows for time periods of low CG activity.

56
Using Formative Research to adapt curricula to local context What sort of formative research studies do you think are the most helpful in developing behavior change curricula, whether you are using Care Groups or not? Positive Deviance Inquiries can be useful (e.g., Local Determinants of Malnutrition Studies) to identify the most important behaviors to change (those linked with malnutrition). Barrier Analysis or Doer/NonDoer Analysis to help staff to better understand how to successfully promote behavior change by identifying the most important barriers to change. (Also used Verbal Autopsy and HF Assessment in Moz.) Barrier Analysis will be discussed on Thursday, 2:00p, as part of the Designing for Behavior Change session. Narrated presentations on Care Groups, LDM Studies, and Barrier Analysis available at www.CareGroupInfo.org.www.CareGroupInfo.org
 to identify the most important behaviors to change (those linked with malnutrition). Barrier Analysis or Doer/NonDoer Analysis to help staff to better understand how to successfully promote behavior change by identifying the most important barriers to change. (Also used Verbal Autopsy and HF Assessment in Moz.) Barrier Analysis will be discussed on Thursday, 2:00p, as part of the Designing for Behavior Change session. Narrated presentations on Care Groups, LDM Studies, and Barrier Analysis available at")
57
155 minute mark

58
Important BF Results of a Local Determinants of Malnutrition Study (Mozambique) 45% of mothers of PD children said that they usually or always completely emptied their breasts when breastfeeding their PD child. Only 10% of mothers of malnourished children said that they did usually or always do so. (p=0.006) The odds ratio for this variable was 7.09 (1.36 < OR < 46.45) meaning that mothers of PD children were about seven times more likely to do this. KEY Message: When breastfeeding a child, it is important to always completely empty each breast so that the child gets all of the calories and nutrients that they need.
 The odds ratio for this variable was 7.09 (1.36 < OR < 46.45) meaning that mothers of PD children were about seven times more likely to do this. KEY Message: When breastfeeding a child, it is important to always completely empty each breast so that the child gets all of the calories and nutrients that they need..")
59
KEY MESSAGE: The Milk Changes during Breastfeeding. The longer the child breastfeeds on one breast the richer the milk becomes in protein and fat. The FIRST milk (watery milk) The THIRD Milk (creamy) The SECOND Milk (normal)
 The THIRD Milk (creamy) The SECOND Milk (normal).")
60
67% of mothers of PD children vs. 32% of mothers of malnourished children took at least one month of iron supplements during the months that they were breastfeeding. 67% of mothers of PD children vs. 32% of mothers of malnourished children took at least one month of iron supplements during the months that they were breastfeeding. The odds ratio for this variable was 4.05 (0.99<OR<18.83). Mothers of PD children were more than four times as likely to take iron supplements during breastfeeding as were mothers of malnourished children. KEY Message: All mothers should take iron supplements during pregnancy and while lactating as a way to help their children grow. Important BF Results of a Local Determinants of Malnutrition Study (Mozambique)
. Mothers of PD children were more than four times as likely to take iron supplements during breastfeeding as were mothers of malnourished children. KEY Message: All mothers should take iron supplements during pregnancy and while lactating as a way to help their children grow. Important BF Results of a Local Determinants of Malnutrition Study (Mozambique).")
61
Other Important PD Findings 67% of mothers of PD children said that their child's drinking water was treated were 3.6 times more likely to be positive deviance (well nourished). [p=0.03, OR = 3.64 (CI: 0.99-13.9)]. (Role of untreated water.) Probably related: 0% of PD children were ill with diarrhea during the past two weeks vs. 29% of malnourished children. (p=0.02) (Role of diarrhea in malnutrition … and malnutrition in diarrhea.) PD nutrients: B2, potassium, and magnesium appeared to be associated with PD in this population.
]. (Role of untreated water.) Probably related: 0% of PD children were ill with diarrhea during the past two weeks vs. 29% of malnourished children. (p=0.02) (Role of diarrhea in malnutrition … and malnutrition in diarrhea.) PD nutrients: B2, potassium, and magnesium appeared to be associated with PD in this population..")
62
BARRIER ANALYSIS RESULTS What are the advantages to exclusive breastfeeding? (OR = 0.22) child grows well” (p=0.06; OR=0.44) Also, “child grows well” (p=0.06; OR=0.44) Emphasized lower cost of EBF (and other benfits) when promoting EBF
 child grows well (p=0.06; OR=0.44) Also, child grows well (p=0.06; OR=0.44) Emphasized lower cost of EBF (and other benfits) when promoting EBF.")
63
Monitoring of Care Groups: Mini-KPCs Development projects typically measure impact and progress toward targets at midterm when only 40% of the project is left to be completed. Mini-KPCs can be used to to improve program effectiveness by targeting indicators that are not improving as expected. Mini-KPC’s are short surveys that are conducted every three to twelve months. Survey results can be easily analyzed by field offices and the results quickly obtained to inform program decisions.

64
Complete vs Mini KPC Complete KPC Include many questions (+/- 60) Require large amounts of staff time for training, implementation, and analysis Attempts to provide information that allows for a program (or program area) to be completely assessed or evaluated. Mini-KPC ► Includes 12-20 question (2- 3 page questionnaire) ► Is done frequently, so after the initial training can be easily implemented and analyzed. ► Staff with little statistical training can do the analysis and quickly use the results. LQAS often used. ► Attempts to provide frequent feedback about specific aspects of a program.
 ► Is done frequently, so after the initial training can be easily implemented and analyzed. ► Staff with little statistical training can do the analysis and quickly use the results. LQAS often used. ► Attempts to provide frequent feedback about specific aspects of a program..")
65
Mini-KPC Example The results of the December 2007 mini-KPC indicated that children 6-23m receiving 3+ meals a day was below target in 2 of the 5 project districts. Decision Rule is 10 for proj. target of 65%

66
Mini-KPC Example Program management realized that unless feeding frequency was increased the project goal of decreasing malnutrition would not be reached. The team decided that more health promotion and skill building needed to be done in promoting snacks for children. Created snack recipes and shared them with mothers.

67
Decision Rule is 8 or 9 Decision Rule is 10 for proj. target of 65% Mini-KPC Example One Year Later

68
How to set-up a system of Mini-KPC’s After creating your program calendar that includes the type of interventions to be carried out and content of education or behavior change promotion materials, schedule your mini-KPCs. Using your project indicator table select priority indicators that need to be tracked frequently, and trended over time. Select other indicators to track only intermittently. Decide if you would like to track additional indicators.

69
Indicate on a KPC Schedule which Indicators will be tracked when. Baseline Questionnaire content 1st Mini-KPC Questionnaire content 2nd Mini-KPC Questionnaire content 3rd Mini-KPC Questionnaire content 4th Mini-KPC Questionnaire content Covered all project areas Focused on Module #2: Sanitation and Hygiene content Focused on Module #3: Diarrhea Focused on Module #5&6: BF & Comp Feeding Focused on Module #6&7: Micronut., Nut/Care for Pregnant Women Question on hand washingEBF Water purificationInitial BF within first hourAdding oil to FoodVit. A rich foods Diarrhea, last two weeksFully emptying / giving both breasts Iron-rich foods Hand-washing station (obsBF during pregnancy Consumption of potassium, mag. and B2-rich foods Disposal of fecesBF if HIV+, K Preparation of any named snacks that FH is promoting Food covered Participation in GM/PEating more during pregnancy, K Food frequencyPostpartum danger signs K BF initiation, within first hour Vit.A supplementation Visited by CGV past two weeksVisited by CGV past 2wks Care seeking for fever Anthropometrics

70
After you’ve made your schedule: Track slow moving indicators frequently If you have consistent and repeated success with your key indicators, track them less frequently If you are using more than one questionnaire, track different indicators on the different questionnaires to keep each questionnaires short.

71
4th Mini-KPC Questionnaire content Focused on Module #6&7: Micronutrients and Nutrition and Care for Pregnant Women EBF Consumption of Vitamin A rich foods Consumption of iron-rich foods Consumption of potassium, magnesium and B2-rich foods Preparation of any named snacks that FH is promoting Importance of eating more during pregnancy, knowledge Knowledge of postpartum danger signs TT coverage DPT3 coverage Care seeking last time child had fever Anthropometry Questionnaire for Mothers of children 0-5m Questionnaire for Mothers of Children 6-23m Vitamin A supplementation Consumption of Vitamin A rich foods Consumption of iron-rich foods Consumption of potassium, magnesium and B2-rich foods Preparation of any named snacks that FH is promoting Exclusive BF Eating more during pregnancy, knowledge Postpartum danger signs, knowledge TT coverage Care seeking last time child had fever Anthropometry

72
Main monitoring tool should be the Mini-KPC looking for behavior change. Promoter Monthly Report and Program Manager Monthly Report Quality Improvement and Verification Checklists: Full session on use of QIVCs on Thursday at 4:00p Monitoring of Care Groups: Other Tools

73
166 minute mark

74
Your Questions on… When to use and not use Care Groups? Incentives? Developing lesson plans and flipcharts? Promoter’s, CGV’s, or Supervisor’s role? Monitoring CGs? Anything else?

75
Remember: Respond to the call for participants for the three regional and six country-level five-day skill-building trainings on Care Groups and other coverage strategies that will be provided in 2012/2013 for FS implementers

76
This presentation was made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Save the Children and do not necessarily reflect the views of USAID or the United States Government.

Similar presentations









 2012 Module 3: Maternity Protection at work: Why is it important?>")



 Office of Overseas Programming & Training Support (OPATS) HIV Prevention Training Package Session 1: Introduction.>")


. 3 of those 8 Goals focus on health – that being child mortality,>")



