Download presentation
1
UPDATE ON RENAL BONE DISEASE Dr Jo Taylor July, 2006

2
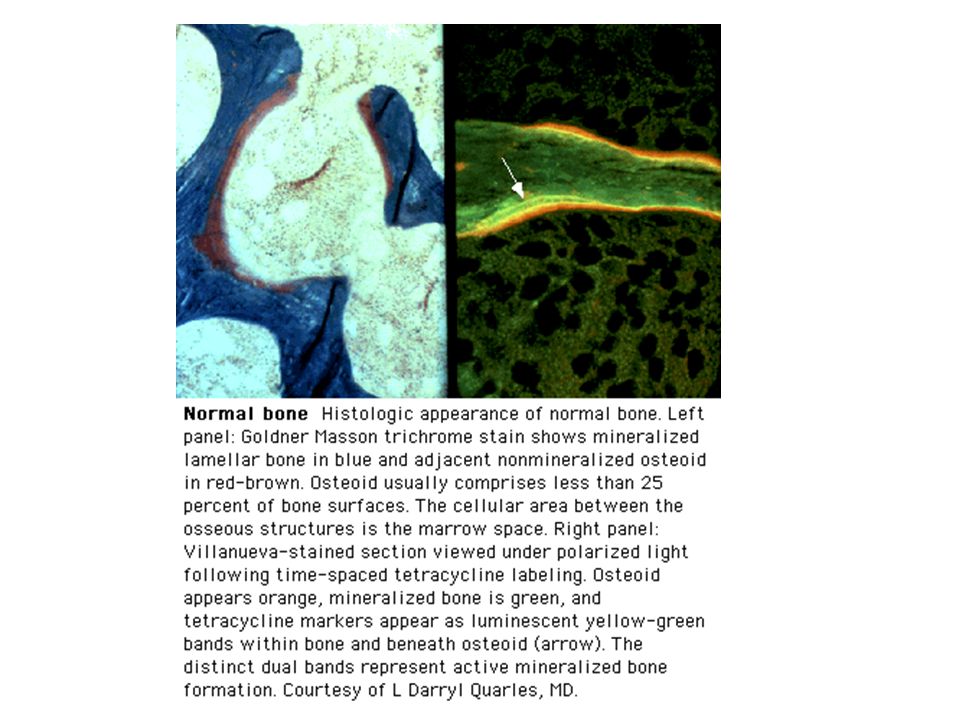
Normal Bone Production of organic matrix by osteoblasts Matrix maturation Mineralisation of mature matrix Osteoclastic resorption of mineralised bone Normal bone undergoes constant remodelling

3
Bone disease in patients with renal failure Osteoporosis (post-transplant, vasculitis) Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)
 Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)")
4
Bone disease in patients with renal failure Osteoporosis (post-transplant, vasculitis) Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)
 Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)")
5
Osteoporosis 200 million world wide USA – 25 million – costing over 10 billion to treat! Decreased bone mass with disruption of normal architecture Primary and Secondary

6
Changes with Age

7
Secondary Osteoporosis Corticosteroids – second commonest cause of osteoporosis Cumulative dose correlates with severity and incidence of fracture Trabecular bone more sensitive than cortical bone Rib and vertebral fractures

8
Osteoporosis – Inx/Rx Laboratory values normal Bone densitometry more sensitive than x-rays Exercise, avoid alcohol and smoking Calcium and Vitamin D Bisphosphonates Others (calcitonin, fluoride, raloxifine, PTH)
")
10
Bone disease in patients with renal failure Osteoporosis (post-transplant, vasculitis) Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)
 Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)")
11
Osteomalacia Disorder of mineralisation of newly formed bone matrix Vitamin D deficiency Hypophosphatemia (Fanconi syndrome, X-linked hypophosphatemic rickets) Bone matrix disorders (Fibrogenesis imperfecta, Hypophosphatasia) Aluminium
 Bone matrix disorders (Fibrogenesis imperfecta, Hypophosphatasia) Aluminium")
13
Vitamin D Metabolism

14
Osteomalacia Skeletal pain, proximal muscle weakness X-ray – Looser’s zones Laboratory – low PO4-, (vitamin D deficiency: low Ca2+, increased alkaline phosphatase) Treat underlying deficiency
 Treat underlying deficiency")
17
Osteomalacia Skeletal pain, proximal muscle weakness X-ray – Looser’s zones Laboratory – low PO4-, (vitamin D deficiency: low Ca2+, increased alkaline phosphatase) Treat underlying deficiency
 Treat underlying deficiency")
18
Aluminium toxicity Aluminium absorption from diet enhanced by citrate and iron deficiency Other sources – dialysate, aluminium hydroxide Effects:1.Anaemia (microcytic) 2.Encephalopathy(apraxia, dementia) 3.PTH suppression (adynamic bone) 4.Bone (impaired mineralisation osteomalacia; impaired cell proliferation – adynamic bone)
 2.Encephalopathy(apraxia, dementia) 3.PTH suppression (adynamic bone) 4.Bone (impaired mineralisation osteomalacia; impaired cell proliferation – adynamic bone)")
23
Aluminium toxicity Normal: less than 20 mcg/l Desferioxamine test: 5mg/kg in 100 ml saline over last hour of dialysis; measure aluminium levels pre-dialysis, and 40 hours later Aluminium toxicity: increase in aluminium level of > 50 mcg/l Desferioxamine infusions – note side effects High flux dialysis if level > 200 mcg/l Care with parathyroidectomy!

24
Aluminium toxicity Post-DFO test Al rise: 50 – 299 mcg/l: DFO infusion (5mg/kg) during last hour of dialysis, weekly for 2 months Post DFO test Al rise: > 300 mcg/l: DFO infusion 5 hours pre-dialysis, weekly for 4 months (also if side effects with DFO) Follow DFO infusion with High Flux Dialysis session
 during last hour of dialysis, weekly for 2 months Post DFO test Al rise: > 300 mcg/l: DFO infusion 5 hours pre-dialysis, weekly for 4 months (also if side effects with DFO) Follow DFO infusion with High Flux Dialysis session")
25
Bone disease in patients with renal failure Osteoporosis (post-transplant, vasculitis) Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)
 Osteomalacia – Aluminium related, or Vitamin D deficiency (CRF, Dialysis) Hyperparathyroidism (CRF, Dialysis) Adynamic bone disease (low or suppressed PTH)")
26
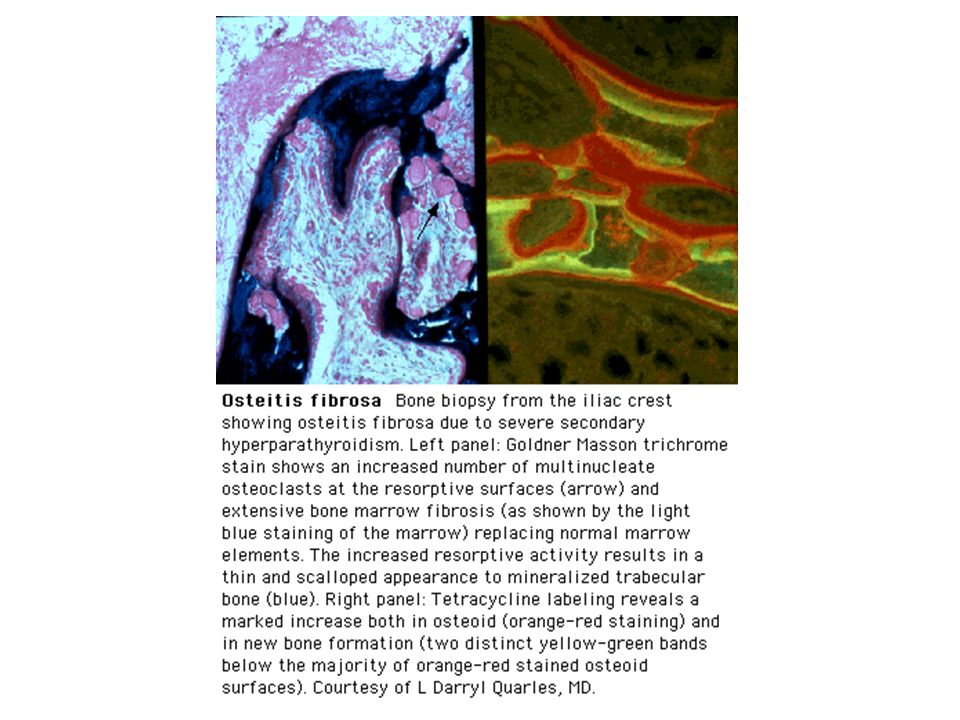
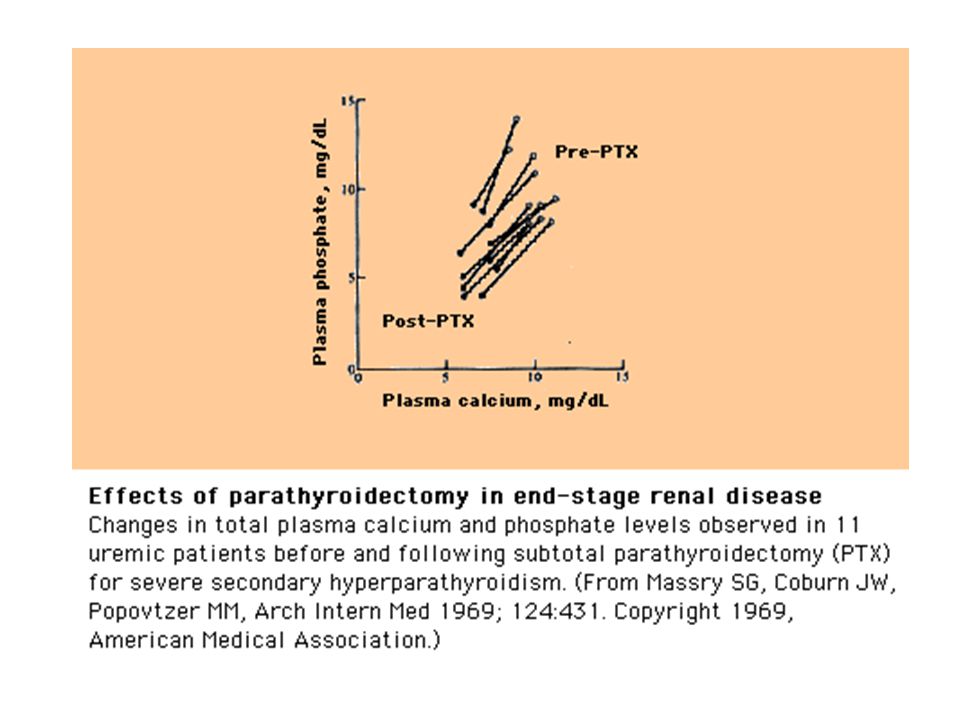
Hyperparathyroidism Osteitis Fibrosa Cystica Excess of Parathyroid Hormone causing marrow fibrosis, expansion of osteoid surfaces, and numerous osteoclasts with resorptive surfaces

29
Effect of Renal Failure PHOSPHATE RETENTION Reduced synthesis of 1,25-dihydroxy-D3 (also, suppression of 1-hydroxylase enzyme by hyperphosphataemia, uric acid, ?uraemic toxins) Stimulation of parathyroid glands (low calcium, low vitamin D, raised phosphate)
 Stimulation of parathyroid glands (low calcium, low vitamin D, raised phosphate)")
30
Parathyroid Hormone Increases tubular reabsorption of calcium Increases renal phosphate excretion Increases renal synthesis of 1,25-dihydroxy-D3 Increases intestinal calcium absorption Increases osteoclastic reabsorption of bone Stimulates osteoblast maturation Parathyroid glands have calcium and vitamin D sensing receptors

32
Hyperparathyroidism Primary:High Ca2+, Low PO4- (Adenoma, normal U&Es) Secondary:Low Ca2+, High PO4- (Early CRF) Tertiary:High Ca2+, High PO4- (Late CRF)
 Secondary:Low Ca2+, High PO4- (Early CRF) Tertiary:High Ca2+, High PO4- (Late CRF)")
35
Adynamic bone disease Lack or suppression of PTH Aluminium toxicity Reduced trabecular bone formation and resorption Unlike osteomalacia – no increase in osteoid formation or unmineralised bone

37
Adynamic Bone Disease Risk factors: Calcium and Vitamin D Parathyroidectomy Age Diabetes Aluminium Fractures, hypercalcaemia (following calcium load)
")
38
Other factors in Renal Bone Disease Metabolic acidosis – bone carbonate buffer Strontium? Bone morphogenetic protein 7 (induces osteoblast growth and differentiation – high levels in normal kidneys)
.")
39
Monitoring of Acidosis CKD 3:12 monthly CKD 4:3 monthly CKD 5:3 monthly Dialysis:Monthly Aim for Bicarbonate > 22 mmol/l

40
Prevalence of Bone Disease in Dialysis Patients Thai Study – 56 patients, bone biopsy 41% adynamic bone disease 29% hyperparathyoidism 20% mixed 4% osteomalacia Changsirikulchai S et al, J Med Assoc Thai 2000; 83: 1223

41
Increased Ca P product Parathyroid gland hyperplasia Increased intact PTH levels (direct and indirect) Coronary artery calcification –Morbidity and mortality –Conduction defects, arrhythmias –Mitral and aortic valve calcification Other calcification, eg, pulmonary, periarticular Myocardial fibrosis 1. Block GA, et al. Am J Kidney Dis. 2000;35:1226-1237. Consequences of Elevated Serum Phosphorus 1

42
70% of Patients Have Elevated Phosphorus Block GA, et al. Am J Kidney Dis. 1998;31:607-617.

43
Dorset 69%

44
Dorset 71%

45
Dorset 87.5%

46
Dorset 74%

47
Dorset 63%

48
Dorset 71%

49
Morbid effects of Metastatic Calcification Type of CalcificationMorbid Effects Myocardial and ValvularAtrioventricular block, cardiac failure, Pulmonary hypertension,arrhythmia, left and right ventricular hypertrophy Small peripheral arteriesBone and soft tissue necrosis PulmonaryCough, dyspnea, restrictive defects, decreased diffusion, hypoxia Tumoral calcinosisSepticemia (especially after surgery)
")
50
1. Adapted from Block GA, et al. Am J Kidney Dis. 1998;31:607-617. Elevated Serum Phosphorus Increases Mortality Risk 1 * P=0.03 ** P<0.0001 (N=6407)
.")
51
Elevated Ca P Product Increases Mortality Risk 1 1. Adapted from Block GA, et al. Am J Kidney Dis. 1998;31:607-617. * P=0.01 (N=2669)
.")
52
Ischemic heart disease Left ventricle dysfunction Arrhythmia Cardiac failure Death 1. Llach F. Kidney Int. 1999;56(suppl 73):S- 31–S-37. 2. Hsu CH. Am J Kidney Dis. 1997;28:641- 649. Consequences of Cardiac Calcification 1 “Calcium and phosphate overload are perhaps the major factors leading to soft tissue calcification….” 2
:S- 31–S Hsu CH. Am J Kidney Dis. 1997;28: Consequences of Cardiac Calcification 1 Calcium and phosphate overload are perhaps the major factors leading to soft tissue calcification…. 2.")
53
USRDS Annual Data Report. 1999. Cause-Specific Death Rates in Dialysis Patients All cardiac Cerebrovasc Infection / Malignancy All others

54
Cardiovascular Disease Mortality General Population vs ESRD Dialysis Patients Foley RN, et al. Am J Kidney Dis. 1998;32:S112- S119. GP: General Population.

55
Risk factors include: 1. Foley RN, et al. Am J Kidney Dis. 1998;32:S112- S119. Cardiac Risk Is Dramatically Increased in Dialysis Patients 1 n Hypertension n LVH n Glucose intolerance n Lipid abnormalities n Cardiovascular and valvular calcification 0.3% 9.2%

56
Atherosclerotic Lesions in Dialysis Patients Slides courtesy of D. Sherrard. Moderately SevereSevere

57
Increased Risk of Cardiovascular Calcification in Dialysis Patients Adapted from Braun J, et al. Am J Kid Dis. 1996;27:394-401. (N=49)
.")
58
1. Ribeiro S, et al. Nephrol Dial Transplant. 1998;13:2037-2040. Presence of Valvular Calcification 1

59
Coronary Artery Calcification in Young Dialysis Patients Adapted from Goodman WG, et al. N Engl J Med. 2000;342:1478- 1483.

60
EBCT Scanning: A Valuable Tool for Evaluating Coronary Calcification Electron beam computed tomography (EBCT), a new noninvasive tool, allows highly sensitive quantification of calcium deposits in living patients. Using EBCT, those patients with calcifications can be diagnosed far earlier than before. Unlike angiography, EBCT can be used for whole body scanning.

61
Slide courtesy of P. Raggi. Electron Beam Computed Tomography (EBCT)
")
62
EBCT Scans Reveal Coronary Artery Calcification in a Dialysis Patient Yellow indicates calcium deposition Slide courtesy of P. Raggi.

63
Calcification: Normal vs ESRD NormalESRD Scan courtesy of P. Raggi.

64
Mitral Valve Calcification in a Dialysis Patient Scan courtesy of P. Raggi.

65
Extensive Triple Vessel (Coronary Arteries) Calcification in a Dialysis Patient Scan courtesy of P. Raggi.

66
Calcification of the Lung Sanders C, et al. Am J Roentgenol. 1987;149:881- 887. Kuzela DC, et al. Am J Pathol. 1977;86:403-424. Slide courtesy of E. Slatopolsky. Calcified Noncalcified

67
Periarticular Calcification Slide courtesy of D. Sherrard.

73
Cutaneous/Subcutaneous Calcification Slide courtesy of H. Malluche.

78
Phosphate – Target levels in CRF Stage 3 and 4 CKD: 0.87 – 1.49mmol/l Stage 5 CKD:1.13 – 1.78mmol/l (only 44% stage 5 CKD achieved this in DOPPS II Study)
")
79
Management of phosphate Dietary phosphate restriction Dialysis Phosphate binders:Aluminium-based Calcium-based Non Ca2+/Al

80
Management of phosphate – limitations of diet Compliance: 800 - 1000 mg/day Phosphate restriction compromises protein intake and nutritional status Highly processed foods contain more easily absorbed phosphate

82
Management of phosphate - dialysis Adequate dialysis Nocturnal dialysis Low calcium dialysis fluid (1.25 mmol/l) to reduce calcium-phosphate product Very low calcium dialysate may exacerbate hyperparathyroidism
 to reduce calcium-phosphate product Very low calcium dialysate may exacerbate hyperparathyroidism")
83
Management of phosphate – phosphate binders Aluminium-based – risk of toxicity Calcium-based – risk of metastatic calcification (due to inability to excrete calcium, and low turnover bone disease in some cases) Non-Ca2+/Al-based – effective, but costly and large numbers of tablets required - Sevelemer hydrochloride (Renegel); Lanthanum (Fosrenol)
 Non-Ca2+/Al-based – effective, but costly and large numbers of tablets required - Sevelemer hydrochloride (Renegel); Lanthanum (Fosrenol)")
84
Sevelemer Lower hypercalcaemia (5% vs 16%) Lower LDL-cholesterol (1.68 vs 2.66 mmol/l) Lower percentage increase in coronary artery (5% vs 25%), and aorta calcification (5% vs 28%) Decrease in CRP
 Lower LDL-cholesterol (1.68 vs 2.66 mmol/l) Lower percentage increase in coronary artery (5% vs 25%), and aorta calcification (5% vs 28%) Decrease in CRP")
85
Vitamin D Therapy Suppress PTH secretion in low calcium states Avoid if Ca2+ > 2.37 or PO4- > 1.49mmol/l Ergocalciferol, Cholecalciferol One-alpha calcidol – requires 25 hydroxylation in liver, Calcitriol (1,25 dihydroxy-D3) Vitamin D analogues (Paricalcitol, Doxercalciferol, 22-oxacalcitriol)
 Vitamin D analogues (Paricalcitol, Doxercalciferol, 22-oxacalcitriol)")
86
Vitamin D Therapy - Monitoring CKD Stages 3 and 4: If PTH raised, measure Vitamin D level and supplement (non-active Vitamin D preparation) if low (< 75 nmol/l). If normal, measure Vitamin D annually. If Vitamin D level > 75 nmol/l, and PTH still high, use active Vitamin D preparation Patients on Vitamin D should have calcium and phosphate levels measured 3 monthly, and annual Vitamin D levels. PTH levels 3 monthly if on active Vitamin D

88
Management of tertiary hyperparathyroidism Risk of metastatic calcification Subtotal/total parathyroidectomy – PTH > 88 pmol/l with raised Ca2+ and/or PO4- Calcimimetics (calcium receptor agonists) Risk of low turnover (adynamic) bone disease in absence of PTH
 Risk of low turnover (adynamic) bone disease in absence of PTH")
89
Calcimimetics Increases the sensitivity of the calcium sensing receptor in the parathyroid glands Dose 30 – 180 mg/day Reduced PTH, Ca2+, and PO4- Less likely to have parathyroidectomy Less likely to fracture Cunningham J et al. Kidney Int 2005; 68: 1794

92
Treatment goals Phosphate – CKD 3/4 (0.87 – 1.49 mmol/l) CKD 5 (1.13 – 1.78 mmol/l) Calcium – low normal (2.1 – 2.37 mmol/l) PTH – CKD 3 (3.85 – 7.7 pmol/l) CKD 4 (7.7 – 12.1 pmol/l) CKD 5 (16.5 – 33 pmol/l) Ensure calcium-phosphate product does not exceed 4.44 mmol 2 /l 2
 CKD 5 (1.13 – 1.78 mmol/l) Calcium – low normal (2.1 – 2.37 mmol/l) PTH – CKD 3 (3.85 – 7.7 pmol/l) CKD 4 (7.7 – 12.1 pmol/l) CKD 5 (16.5 – 33 pmol/l) Ensure calcium-phosphate product does not exceed 4.44 mmol 2 /l 2")
93
Achievement of Treatment Goals 26% PTH 44% PO4- 43% Ca2+ 61% Ca2+/PO4- product DOPPS II Study (Am J Kidney Dis 2004; 44: 34)
")
94
Monitoring of Ca2+/PO4-/PTH CKD StagePTHCa2+/PO4- 312 months 43 months 5 1 month

95
Post-transplant monitoring Bone densitometry: Baseline, 1 and 2 years post-transplant Calcium, Phosphate, Bicarbonate: Fortnightly for 3 months, then monthly during first year PTH: Monthly during first 3 months, then 3- monthly during first year. Thereafter according to CKD guidelines

96
UK RCGP Guidelines Stage 3 CKD – check PTH If PTH raised, check Vitamin D level If Vitamin D level low, give non-active Vitamin D + calcium supplement Repeat PTH at 3 months – if still high - refer






































 1,25(OH) 2 D 3 calcitriol Synthesis of active vitamin D 10%, 90%, Bile Salts Tightly regulated 25-hydroxylase.>")



 Vitamin D 2 : Ergosterol (pro D 2 ) Ergocalciferol (D 2 ) added to milk and dairy. (Human) Vitamin D 3 : Pro (7-dehydrocholesterol)>")
