Download presentation
Presentation is loading. Please wait.

1
Bone Disease in Renal Failure Dr Anne Kleinitz and Dr Cherelle Fitzclarence renalgp@kamsc.org.au

2
Overview Pathogenesis Normal Bone Remodeling Hyperparathyroidism Classifications of bone disease Diagnosis of bone disease Treatment of bone disease in CKD Case Studies

3
Pathogenesis Kidney failure disrupts systemic calcium and phosphate homeostasis and affects the bone, GIT and parathyroid glands. In kidney failure there is decreased renal excretion of phosphate and diminished production of calcitriol (1,25- dihydroxyvitamin D) –Calitriol increases serum calcium levels The increased phosphate and reduced calcium, feedback and lead to secondary hyperparathyroidism, metabolic bone disease, soft tissue calcifications and other metabolic abnormalities
 –Calitriol increases serum calcium levels The increased phosphate and reduced calcium, feedback and lead to secondary hyperparathyroidism, metabolic bone disease, soft tissue calcifications and other metabolic abnormalities.")
4
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH Calcitriol

5
Although bone disease and abnormal PTH are a major feature, CVD and excess calcification (extra-skeletal) are important causes of morbidity and mortality
 are important causes of morbidity and mortality")
6
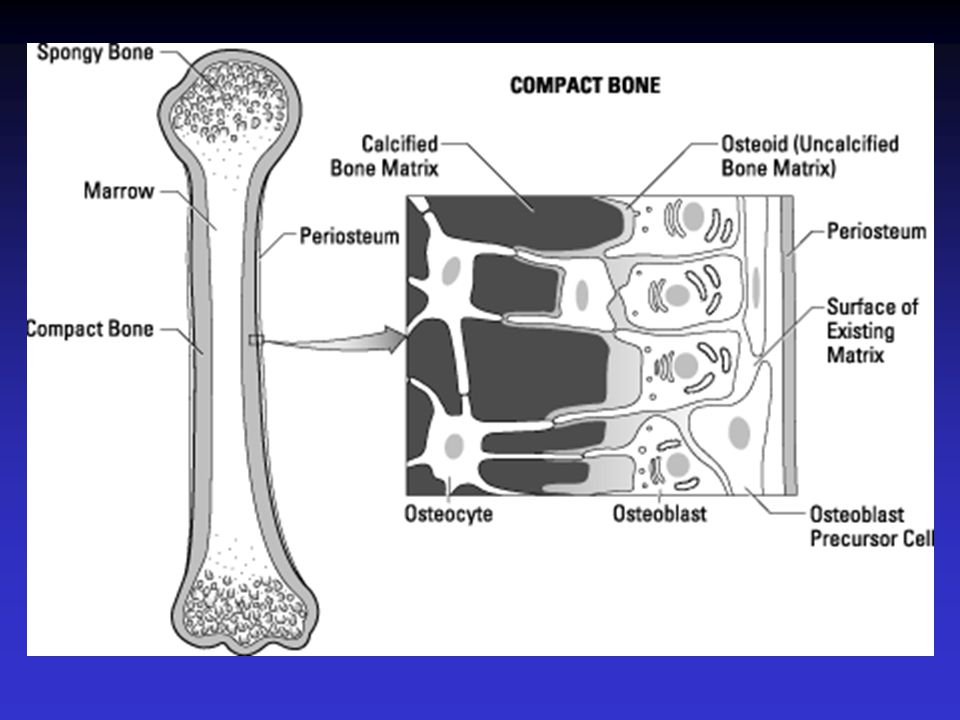
Pathogenesis Normal Bone Remodeling

7
Resorption osteoclasts Formation osteoblasts → matrix Mineralisation Quiescence Normal Bone Remodelling Cycle

8
Pathogenesis Normal Bone Remodeling Hyperparathyroidism

9
Increase PTH is hallmark of secondary hyperparathyroidism The major factors leading to it’s increase are; –Decreased production of Vit D3 (calcitriol) –Decreased serum calcium –Increased serum phosphorous
 –Decreased serum calcium –Increased serum phosphorous")
10
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH Calcitriol

11
4 or more small glands on the posterior surface of the thyroid gland. Can function without neural control so can transplant to another part of the body 2 types of cells –Chief cells – produce parathyroid hormone –Oxyntic cells – function unknown

12
Role of PTH Responsible for maintaining serum calcium in a narrow range (2.15-2.6) Does this by; 1. acting directly on the distal tubule of the kidney to increase calcium reabsorption –Increases calcitriol production (D3) –D3 increases GIT absorption of Ca and Phos and promotes osteoclast formation. 2. Acting on bone to increase calcium and phosphate efflux
 –D3 increases GIT absorption of Ca and Phos and promotes osteoclast formation. 2. Acting on bone to increase calcium and phosphate efflux.")
13
The net effect of PTH is to create positive calcium balance necessary to maintain homeostasis. To balance out the increased phos from skeletal effects, and GIT effects of calcitriol, PTH acts secondarily to increase renal phos excretion –By decreasing activity of sodium phosphate co- transporter in prox renal tubule.

14
Uraemic Secondary Hyperparathyroidism Cause PO 4 retention Low 1,25 Vit D synthesis Effects Proximal weakness, Bone pain (late) ↑ Alk Phos, bone erosions Rx Diet, PO 4 binders Calcitriol, PTHx (usually for 3 o )
 ↑ Alk Phos, bone erosions Rx Diet, PO 4 binders Calcitriol, PTHx (usually for 3 o )")
15
Secondary hyperparathyroidism In renal failure driven by –Hypocalcaemia –Decreased vitamin D –hyperphosphataemia

16
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH Calcitriol

18
hyperPTH in CKD In CKD is a progressive disorder. Involves both increased secretion PTH & hyperplasia Can occur once eGFR < 60 PTH levels increase progressively as renal function declines and by CKD stage 5(<15) most pt’s expected to have this. Usually the 1 st sign and occurs before lab tests pick up phosphatemia, ↓ Vit D3 and ↓ calcium –Presumably as PTH is maintaining homeostasis. Unless treated, progresses and frequency of parathyroidectomy proportional to yrs on dialysis
 most pt’s expected to have this. Usually the 1 st sign and occurs before lab tests pick up phosphatemia, ↓ Vit D3 and ↓ calcium –Presumably as PTH is maintaining homeostasis. Unless treated, progresses and frequency of parathyroidectomy proportional to yrs on dialysis.")
19
Overview Pathogenesis Normal Bone Remodeling Hyperparathyroidism Classifications of bone disease in CKD

20
Classification of Bone Disease in CKD The circulating level of PTH is primary determinant of bone turnover in CKD Type of bone disease depends upon –Age of pt –Duration of kidney failure –Severity of hyperPTH –Type of dialysis PTH & Vit D receptors, as well as calcium sensors are present on osteoblasts

22
Types of Renal Bone Disease Traditionally classified according to degree of abnormal bone turnover High Turnover (osteitis fibrosa) –Hyperparathyroidism Low turnover –Adynamic- Osteomalacia Beta 2 MG amyloidosis Osteoporosis –Post-menopausal- Post-transplant
 –Hyperparathyroidism Low turnover –Adynamic- Osteomalacia Beta 2 MG amyloidosis Osteoporosis –Post-menopausal- Post-transplant")
23
Resorption osteoclasts Formation osteoblasts → matrix Accelerates: High PO 4 or Low Ca 2+, Vit D3, Retards: Vit D3, Age, Diabetes, Al 3+, PTHx Mineralisation Quiescence Uraemic Bone RemodellingCycle

24
Resorption osteoclasts Formation osteoblasts → matrix Accelerates: High PO 4 or Low Ca 2+, calcitriol, HCO 3, oestrogen Retards: Calcitriol*, Age, Diabetes, Al 3+, PTHx Mineralisation *Acts via osteoblasts Quiescence Uraemic Bone RemodellingCycle Via PTH*, IL-1,6 & TNF

25
High turn over bone disease Due to excess PTH Increased bone turnover activity (greater number of osteoclasts and osteoblasts) and defective mineralization. Associated with bone pain and increased risk of fractures. Severe symptomatic disease is currently uncommon with modern therapy.

26
Mixed uraemic bone disease Mixture of high turn over bone disease and osteomalacia

27
Osteomalacia Formally linked to aluminium toxicity –From aluminium based phosphate binders –From contamination of water in diasylate solutions

28
Adynamic bone disease Characterized by low osteoblastic activity and bone formation rates Seen in up to 40% HD and 50% PD May be due to excess suppression of the parathyroid gland with therapies, particularly calcium-containing phosphate binders and vitamin D analogues.vitamin D Typically maintain a low serum intact PTH concentration, which is frequently accompanied by an elevated serum calcium level. Felt to represent a state of relative hypoparathyroidism

29
Clinical manifestations of bone disease Most with CKD and mildly elevated PTH are asymptomatic When present classified as either 1. Musculoskeletal 2. Extra-skeletal

30
Musculoskeletal Fractures, tendon rupture and bone pain from metabolic bone disease, muscular pain and weakness. Most clinically significant is hip fracture, seen in CKD 5 (and is associated with increase risk of death) –NB. In dialysis pts there is already a 4.4 x increase risk of hip fracture.
 –NB. In dialysis pts there is already a 4.4 x increase risk of hip fracture..")
31
Extra-skeletal Important to recognise disordered bone and mineral metabolism is a systemic disorder affecting soft tissues, particularly vessels, heart valves and skin. CVD accounts for around half of all deaths of dialysis patients. Coronary artery and vascular calcifications occur frequently in CKD 5 (and increase each year on dialysis)
.")
32
Types of calcification 1. Focal calcification associated with lipid laden atherosclerotic plaques Increases fragility and risk of plaque rupture 2. Diffuse calcification not in atherosclerotic plaques and occurs in media of vessels Called “Monckeberg’s sclerosis” Increases blood vessel stiffness and reduces vascular compliance Results in widened pulse pressure Increased afterload LVH Contributing to CVD morbidity

34
As per Cherelle “If we X-Ray most of our patients, they’ve got “tram tracks” – we hardly need an angiogram!”

35
Types of calcification Calciphylaxis or calcemic uremic arteriopathy –Seen primarily in CKD 5 –Occurs in 1-4% of dialysis patients –Presents with extensive calcification of the skin, muscles and SC tissues. Extensive medial calcification of small arteries, arterioles, capillaries and venules. Clinically they may have skin nodules, skin firmness, eschars, livedo reticularis and painful hyperaesthesia of the skin. May lead to non healing ulcers and gangrene

36
calciphylaxis A, Confluent calf plaques (borders shown with arrows). Parts of the skin are erythematous, which is easily confused with simple cellulitis. B, Gross ulceration in the same patient 3 months later. The black eschar has been surgically débrided. C, Calciphylactic plaques, a few of which are beginning to ulcerate. (Photographs courtesy of Dr. Adrian Fine. Up To Date)
.")
37
Angulated black eschar with surrounding livedo. Note the bullous change at the inferior edge of the eschar. (courtesy Up To Date)
.")
38
Amyloidosis Pts on dialysis for 7- 10 years can develop osteoarticular amyloid deposits. May present with carpel tunnel syndrome and arthritis

39
Overview Pathogenesis Normal Bone Remodeling Hyperparathyroidism Classifications of bone disease Diagnosis of bone disease

40
Diagnosis of CKD bone disease Blood –PTH Random circulating PTH (1/2 life 2-4 mins) Excreted renally so present for longer in RF –Calcium –Phosphate Bone biopsy –no longer frequently performed Imaging –In general not indicated
 Excreted renally so present for longer in RF –Calcium –Phosphate Bone biopsy –no longer frequently performed Imaging –In general not indicated")
41
PTH levels Normal ( Pathwest ) 0.7 – 7.0 pmol/L In CKD there is end-organ resistance Hence, recommended levels are 2 – 3 x normal.
 0.7 – 7.0 pmol/L In CKD there is end-organ resistance Hence, recommended levels are 2 – 3 x normal.")
42
Overview Pathogenesis Normal Bone Remodeling Hyperparathyroidism Classifications of bone disease Diagnosis of bone disease Treatment of bone disease in CKD

43
Treatment of CKD bone disease Directed towards normalising serum calcium, phosphate and PTH, while minimizing the risks associated with Rx

44
Treatment of CKD bone disease Various Rx for secondary hyperPTH and hyperphosphataemia include; 1. Dietary phosphorous restriction 2. Calcium and non-Ca phosphate binders 3. Calcitriol or other Vit D analogues 4. Calcimimetics 5. Parathyroidectomy

45
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH ↓Coke & dairy food CaCO3 with meals Calcitriol

46
Phosphorus (oxidized form is phosphate) 80% in the bone Food products include; nuts, beer, chocolate, coca-cola Normal level 0.8 – 1.5mmol/L ( Pathwest ) Passes into glomerular filtrate and 90% reabsorbed Reabsorption decreased by PTH and by calcitonin and increased if PTH is absent Low levels if hyperparathyroidism with excessive losses in urine High levels in hypoparathyroidism or renal failure
 80% in the bone Food products include; nuts, beer, chocolate, coca-cola Normal level 0.8 – 1.5mmol/L ( Pathwest ) Passes into glomerular filtrate and 90% reabsorbed Reabsorption decreased by PTH and by calcitonin and increased if PTH is absent Low levels if hyperparathyroidism with excessive losses in urine High levels in hypoparathyroidism or renal failure")
47
Phosphate binders Calcium-based phosphate binders –Calcium carbonate (Cal-Sup/Caltrate) –Only Cal-Sup i PBS/S100 –Varies, eg. 1 BD, 1-4 TDS –Must be chewed with food to maximize binding of ingested phosphorous.

48
Phosphate binders Non-calcium phos binder Sevelamer (available for 12 months) –Often used in conjunction with Cal-sup –Used when phos still high despite max Cal-Sup (2 TDS) –More costly
 –Often used in conjunction with Cal-sup –Used when phos still high despite max Cal-Sup (2 TDS) –More costly")
49
Phosphate binders Aluminium-containing phos binders –Alu-tabs/aluminium hydroxide –Most effective, but ceaesd use around 12 months ago when sevelamer and cinacalcet available. –Systemic absorption with subsequent neurological, haematological and bone toxicity.

50
Calcitriol 1,25-(OH)2 Vitamin D3 or other analogues bind to receptor on PT tissue and suppress PTH production
2 Vitamin D3 or other analogues bind to receptor on PT tissue and suppress PTH production")
51
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH Calcitriol

52
Calcitonin Produced by parafollicular or C cells of the thyroid gland Secreted when plasma calcium level rises Main action is the lowering of plasma calcium by limiting bone resorption and it increases phosphate excretion in the urine

53
Calcimimetics Calcium receptor-sensing agonists Act on PT gland and increase sensitivity of receptor to calcium Cinacalcet (Sensipar) –Significant decrease PTH, w/o Ca or phos –Avoids calcification
 –Significant decrease PTH, w/o Ca or phos –Avoids calcification")
54
↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH Calcitriol

55
Parathyroidectomy Last option Considered when other methods fail to ↓ PTH Either total or sub-total –Used to re-implant in forearm.

56
Summary of Rx Dietary phosphate restriction Phosphate binders Calcitriol or other Vit D analogues Calcium supplementation/calcimimetics Parathyroidectomy

57
Prevention of osteodystrophy ↓GFR ↑PO4 ↓1,25 DHCC ↓Ca ↑PTH ↓Coke & dairy food CaCO3 with meals Calcitriol

58
Transplant Bony changes improve post Tx, but if severe increased PTH, levels can persist for up top 10 years. Although Tx corrects many conditions leading to disordered mineral metabolism, Steroids may lead to bone fragility, osteoporosis and increased fractures.

59
Case Studies

60
Case 1 MC Diabetic nephropathy – Haemodialysis Hypothyroidism Pancreatic pseudocyst Epilepsy Anaemia Hypertension

61
Case 1 Currently PTH 104 Ca corrected 2.04 Po4 1.77 Medications –Calcium carbonate 2 three times with meals –Calcitriol 1mic 3 times a week

62
Case 1 What do we do? Thoughts?

63
Case 1 This lady is non compliant! No point changing her regime if she is not taking what you have written up Encourage compliance Explain the essential nature of compliance with this therapy

64
Case 2 RJ Diabetes Anaemia Dementia Alcoholism End stage kidney disease – CAPD IHD/cardiomyopathy – recent massive AMI Syphilis

65
Case 2 PO4 3.77 Ca 1.82 Product 6.86 PTH 166 Thoughts?

66
Case 2 Again non compliance Recent finding of around 20 webster packs in his room

67
Case 3 DB Diabetes End stage kidney disease – HD Hypothyroidism Hypertension Anaemia Recurrent laryngeal palsy IHD Constipation Depression Cerebrovasvcular disease

68
Case 3 Ca 2.72 PO4 1.39 PTH 20.1 Product 3.7 Thoughts?

69
Case 3 Has had parathyroidectomy (hence the recurrent laryngeal palsy) and parameters are exactly where we want them Meds –Calsup 2 tds with food –Calcitriol 6 (1.5mics) twice a week at dialysis
 and parameters are exactly where we want them Meds –Calsup 2 tds with food –Calcitriol 6 (1.5mics) twice a week at dialysis")
70
Case 4 ID Usual litany of problems HD Po4 1.0 Ca 2.6 PTH 3.1 Thoughts?

71
Case 4 Oversuppressed Need the PTH to be 2-3 times normal or patient will likely get adynamic bone disease Back off Vit D and Calcium In this case pt was on Calsup 2 tds and Calcitriol 6 (1.5mics) twice a week. Decrease Calcitriol eg 1.5mics once a week and decrease Calsup to 1 tds Monitor

72
Thank you! renalgp@kamsc.org.au

73
Calcium and Phosphorus Homeostasis

74
References Dr Mark Thomas, Nephrologist, Royal Perth Hospital Primer on Kidney Diseases, 5 th Edition. Greenberg, National Kidney Foundation. 2009

Similar presentations




 –Free calcium is 1.2 mM.>")
















