Download presentation
Presentation is loading. Please wait.

1
Biomedical waste Management
Collected by JHPatel

2
Unit3 : Biomedical waste Management : definition, health and Environment issues. Category of waste, segregation, collection , and transportation . Treatment systems.

3
Biomedical waste Management

4
Definitions Legal: "Bio-medical waste" means any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or in research activities pertaining thereto or in the production or testing of biologicals, and including categories mentioned in Schedule I;

5
Scientific definition
"Bio-medical waste" is the waste solids, liquids, sharps, and laboratory waste that are potentially infectious or dangerous and are considered biowaste. It is a waste from biological sources or is used in the diagnosis, prevention, or treatment of diseases. Common producers of biomedical waste include hospitals, health clinics, nursing homes, medical research laboratories, offices of physicians, dentists, and veterinarians, home health care, and funeral homes. BIOMEDICAL WASTE Any solid, fluid and liquid or liquid waste, including it’s container and any intermediate product, which is generated during the diagnosis, treatment or immunisation of human being or animals, in research pertaining thereto, or in the production or testing of biological and the animal waste from slaughter houses or any other similar establishment Similar spirit is there in Indian Legal definition

6
Why to manage BMW? The reasons are:
1. Injuries from sharps leading to infection to all categories of hospital personnel and waste handler. 2. nosocomial infections in patients from poor infection control practices and poor waste management. 3. Risk of infection outside hospital for waste handlers and scavengers and at time general public living in the vicinity of hospitals. 4. Risk associated with hazardous chemicals, drugs to persons handling wastes at all levels. 5. “Disposable” being repacked and sold by unscrupulous elements without even being washed. 6. Drugs which have been disposed of, being repacked and sold off to unsuspecting buyers. 7. Risk of air, water and soil pollution directly due to waste, or due to defective incineration emissions and ash.

7
2. Collection of bio-medical waste
APPROACH FOR biomedical WASTE MANAGEMENT 1. Segregation of waste Segregation is the essence of waste management and should be done at the source of generation of Bio-medical waste e.g. all patient care activity areas, diagnostic services areas, operation theaters, labour rooms, treatment rooms etc. The responsibility of segregation should be with the generator of biomedical waste i.e. doctors, nurses, technicians etc. (medical and paramedical personnel). 2. Collection of bio-medical waste Collection of bio-medical waste should be done as per Bio-medical waste (Management and Handling) Rules. At ordinary room temperature the collected waste should not be stored for more than 24 hours. 3. Transportation Within hospital, waste routes must be designated to avoid the passage of waste through patient care areas. Separate time should be earmarked for transportation of bio-medical waste to reduce chances of it’s mixing with general waste. Desiccated wheeled containers, trolleys or carts should be used to transport the waste/plastic bags to the site of storage/ treatment . 4. Treatment of hospital waste 4.1 General waste The 85% of the waste generated in the hospital belongs to this category. The, safe disposal of this waste is the responsibility of the local authority.
. 2. Collection of bio-medical waste. Collection of bio-medical waste should be done as per Bio-medical waste (Management and Handling) Rules. At ordinary room temperature the collected waste should not be stored for more than 24 hours. 3. Transportation. Within hospital, waste routes must be designated to avoid the passage of waste through patient care areas. Separate time should be earmarked for transportation of bio-medical waste to reduce chances of it’s mixing with general waste. Desiccated wheeled containers, trolleys or carts should be used to transport the waste/plastic bags to the site of storage/ treatment . 4. Treatment of hospital waste. 4.1 General waste. The 85% of the waste generated in the hospital belongs to this category. The, safe disposal of this waste is the responsibility of the local authority.")
8
5. Safety measures 6. Training
4.2 bio-medical waste: 15% of hospital waste 1. Deep burial 2. Autoclave and microwave treatment (Annexure II) 3. Shredding (Annexure II) 4. Secured landfill 5. Incineration (Annexure III) 5. Safety measures 5.1 All the generators of bio–medical waste should adopt universal precautions and appropriate safety measures while doing therapeutic and diagnostic activities and also while handling the bio-medical waste. 5.2 It should be ensured that: 1. Drivers, collectors and other handlers are aware of the nature and risk of the waste. 2. Written instructions, provided regarding the procedures to be adopted in the event of spillage/ accidents. 3. Protective gears provided and instructions regarding their use are given. 4. workers are protected by vaccination against tetanus and hepatitis B 6. Training 1. Each and every hospital must have well planned awareness and training programme for all category of personnel including administrators (medical, paramedical and administrative). 2. All the medical professionals must be made aware of Bio-medical Waste (Management and Handling) Rules 1998. 3. To institute awards for safe hospital waste management and universal precaution practices. 4. Training should be conducted to all categories of staff in appropriate language/medium and in an acceptable manner.
 3. Shredding (Annexure II) 4. Secured landfill. 5. Incineration (Annexure III) 5. Safety measures. 5.1 All the generators of bio–medical waste should adopt universal precautions and appropriate safety measures while doing therapeutic and diagnostic activities and also while handling the bio-medical waste. 5.2 It should be ensured that: 1. Drivers, collectors and other handlers are aware of the nature and risk of the waste. 2. Written instructions, provided regarding the procedures to be adopted in the event of spillage/ accidents. 3. Protective gears provided and instructions regarding their use are given. 4. workers are protected by vaccination against tetanus and hepatitis B. 6. Training. 1. Each and every hospital must have well planned awareness and training programme for all category of personnel including administrators (medical, paramedical and administrative). 2. All the medical professionals must be made aware of Bio-medical Waste (Management and Handling) Rules To institute awards for safe hospital waste management and universal precaution practices. 4. Training should be conducted to all categories of staff in appropriate language/medium and in an acceptable manner.")
9
History and introduction of BMW in India
The modern age, in the 21st century with increased use of disposable material and the presence of dreaded disease like Hepatitis – B and AIDS, it is utmost important to take care of the infected and hazardous waste to save the mankind from disasters. The Health care institution or hospitals which are responsible for care of morbid population are emitting voluminous quantity of rubbish, garbage and Bio Medical Waste matter each day from wards, operation theatre and outpatient areas. Proper management of hospital waste is essential to maintain hygiene, aesthetics, cleanliness and control of environmental pollution. The hospital waste like body parts, organs, tissues, blood and body fluids along with soiled linen, cotton, bandage and plaster casts from infected and contaminated areas are very essential to be properly collected, segregated, stored, transported, treated and disposed of in safe manner to prevent nosocomial or hospital acquired infection . Various communicable diseases, which spread through water, sweat, blood, body fluids and contaminated organs, are important to be prevented. The Bio Medical Waste scattered in and around the hospitals invites flies, insects, rodents, cats and dogs that are responsible for the spread of communication disease like plague and rabies. Rag pickers in the hospital, sorting out the garbage are at a risk of getting tetanus and HIV infections. The recycling of disposable syringes, needles, IV sets and other article like glass bottles without proper sterilization are responsible for Hepatitis, HIV, and other viral diseases. It becomes primary responsibility of Health administrators to manage hospital waste in most safe and eco-friendly manner.

10
1. Supreme Court judgment dated 1st March 1996 in connection with safe disposal of hospital waste ordered that (a) All hospitals with 50 beds and above should install either their own incinerator or an equally effective alternative method before 30th November 1996. (b) The incinerator or the alternative method should be installed with a necessary pollution control mechanism conforming to the standard laid down by Central Pollution Control Board (CPCB). (c) Hazardous medical waste should be segregated as source and disinfected before final disposal. 2. Ministry of Environment & Forest, Govt. of India issued a notification for Biomedical Waste(Management & Handling) Rules 1998 in exercise of powers conferred by Section 6, 8 & 25 of the Environment (Protection) Act, 1986 that was published in The Gazette of India Extraordinary, Part-II, Section 3-Sub-Section (ii) New Delhi, July 27,
 All hospitals with 50 beds and above should install either their own incinerator or an. equally effective alternative method before 30th November (b) The incinerator or the alternative method should be installed with a necessary pollution control mechanism conforming to the standard laid down by Central Pollution Control Board (CPCB). (c) Hazardous medical waste should be segregated as source and disinfected before final. disposal. 2. Ministry of Environment & Forest, Govt. of India issued a notification for Biomedical Waste(Management & Handling) Rules 1998 in exercise of powers conferred by Section 6, 8 & 25 of the Environment (Protection) Act, 1986 that was published in The Gazette of India Extraordinary, Part-II, Section 3-Sub-Section (ii) New Delhi, July 27,")
11
General Description and Quantity
Hospital waste refers to all waste generated, discarded and not intended for further use in the hospital. It is broadly categorized into the following categories: 1. General Waste 2. Pathological Waste 3. Infectious Waste 4. Sharps 5. Pharmaceutical Waste 6. Chemical Waste 7. Radioactive Waste AMOUNT AND COMPOSITION OF HOSPITAL WASTE GENERATED (a) Amount Country Quantity (kg/bed/day) U. K. 2.5 U.S.A. 4.5 France 2.5 Spain 3.0 India 1.5
 Amount. Country Quantity (kg/bed/day) U. K U.S.A France 2.5. Spain 3.0. India 1.5.")
12
(b) Hazardous/non-hazardous
a) Hazardous but non-infective 5% b) Hazardous and infective 10% Non-hazardous 85% (c) Composition By weight Plastic 14% Combustible Dry cellublostic solid 45% Wet cellublostic solid 18% Non-combustible 20%
 Hazardous but non-infective 5% b) Hazardous and infective 10% Non-hazardous 85% (c) Composition. By weight. Plastic 14% Combustible. Dry cellublostic solid 45% Wet cellublostic solid 18% Non-combustible 20%")
14
First notification of MINISTRY OF ENVIRONMENT & FORESTS
NOTIFICATION New Delhi, 20th July, 1998 S.O. 630 (E).-Whereas a notification in exercise of the powers conferred by Sections 6, 8 and 25 of the Environment (Protection) Act, 1986 (29 of 1986) was published in the Gazette vide S.O. 746 (E) dated 16 October, 1997 inviting objections from the public within 60 days from the date of the publication of the said notification on the Bio-Medical Waste (Management and Handling) Rules, 1998 and whereas all objections received were duly considered.. Now, therefore, in exercise of the powers conferred by section 6, 8 and 25 of the Environment (Protection) Act, 1986 the Central Government hereby notifies the rules for the management and handling of bio-medical waste.
.-Whereas a notification in exercise of the powers conferred by Sections 6, 8 and 25 of the Environment (Protection) Act, 1986 (29 of 1986) was published in the Gazette vide S.O. 746 (E) dated 16 October, 1997 inviting objections from the public within 60 days from the date of the publication of the said notification on the Bio-Medical Waste (Management and Handling) Rules, 1998 and whereas all objections received were duly considered.. Now, therefore, in exercise of the powers conferred by section 6, 8 and 25 of the Environment (Protection) Act, 1986 the Central Government hereby notifies the rules for the management and handling of bio-medical waste.")
15
centers/Establishments etc.
Hospitals/Nursing Homes/Maternity centre/Pathological laboratories/Health care centers/Establishments etc. 1. They shall refrain from throwing any bio-medical waste on the streets or open spaces, as well as into the municipal dustbins or the domestic waste collection sites. 2. They shall also refrain from throwing any ordinary solid waste on footpaths, streets or open spaces/nallas. 3. They shall keep colour-coded bins or bags as per the directions of the Govt. of India, Ministry of Environment dated 20th Bio-medical Waste (Management & Handling) Rules 1998, and follow the directions of CPCB & State PCBs from time to time for the storage of biomedical waste including amputated limbs, tissues, soiled bandages, used injections, syringes, etc.
 Rules 1998, and follow the directions of CPCB & State PCBs from time to time for the storage of biomedical waste including amputated limbs, tissues, soiled bandages, used injections, syringes, etc.")
16
Disposal of Bio-Medical Waste
All hospitals, nursing homes, pathology laboratories, health care establishments generating Biomedical waste should dispose of the Bio-medical waste strictly in terms of Bio-medical Waste (Management & Handling) Rules This responsibility is of the waste producer. They should organize themselves and give a contract to a private operator to collect their waste and dispose of at a central facility. All the towns may direct the medical institutions to organize themselves expeditiously and facilitate the creation of waste treatment and disposal facility through a private operator to ensure scientific disposal of waste.
 Rules This responsibility is of the waste producer. They should organize themselves and give a contract to a private operator to collect their waste and dispose of at a central facility. All the towns may direct the medical institutions to organize themselves expeditiously and. facilitate the creation of waste treatment and disposal facility through a private operator to ensure scientific disposal of waste.")
17
Biomedical Waste All syringes, medication vials, alcohol swabs and cotton ball that have come in contact with this medication or with blood or body fluids cannot be disposed of in your regular garbage or dumpster but must be placed in the Sharps Container for disposal as biomedical waste.It is suggested to use color coded bins for disposing Septic waste and food waste in a hospital or Clinics

19
COLOUR CODING AND TYPE OF CONTAINER FOR DISPOSAL OF BIO-MEDICAL WASTES
Colour Conding Type of Container -I Waste Category Treatment options as per Schedule I Yellow Plastic bag Cat. 1, Cat. 2, and Cat. 3, Cat. 6. Incineration/deep burial Red Disinfected container/plastic bag Cat. 3, Cat. 6, Cat.7. Autoclaving/Microwaving/ Chemical Treatment Blue/White translucent Plastic bag/puncture proof Cat. 4, Cat. 7. Container Chemical Treatment and destruction/shredding Black Plastic bag Cat. 5 and Cat. 9 and Cat. 10. (solid) Disposal in secured landfill
 Disposal in secured landfill.")
20
Bio-medical waste bag ready for incineration

22
Bio medical waste symbol to
be tagged in hospitals and clinics at disposal locations for safety.

23
S.O. 630 (E).-Whereas a notification in exercise of the powers conferred by Sections 6, 8 and 25 of the Environment (Protection) Act, 1986 (29 of 1986) was published in the Gazette vide S.O. 746 (E) dated 16 October, 1997 inviting objections from the public within 60 days from the date of the publication of the said notification on the Bio-Medical Waste (Management and Handling) Rules, 1998 and whereas all objections received were duly considered.. Now, therefore, in exercise of the powers conferred by section 6, 8 and 25 of the Environment (Protection) Act, 1986 the Central Government hereby notifies the rules for the management and handling of bio-medical waste. Amended 2003 and draft proposal for 2012
 Act, 1986 the Central Government hereby notifies the rules for the management and handling of bio-medical waste. Amended 2003 and draft proposal for")
24
1. SHORT TITLE AND COMMENCEMENT:
(1) These rules may be called the Bio-Medical Waste (Management and Handling) Rules, 1998. (2) They shall come into force on the date of their publication in the official Gazette. APPLICATION: These rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form.
 These rules may be called the Bio-Medical Waste (Management and Handling) Rules, (2) They shall come into force on the date of their publication in the official Gazette. APPLICATION: These rules apply to all persons who generate, collect, receive, store, transport, treat, dispose, or handle bio medical waste in any form.")
25
3. DEFINITIONS: In these rules unless the context otherwise requires
(1) "Act" means the Environment (Protection) Act, 1986 (29 of 1986); (2) "Animal House" means a place where animals are reared/kept for experiments or testing purposes; (3) "Authorisation" means permission granted by the prescribed authority for the generation, collection, reception, storage, transportation, treatment, disposal and/or any other form of handling of bio-medical waste in accordance with these rules and any guidelines issued by the Central Government. (4) "Authorised person" means an occupier or operator authorised by the prescribed authority to generate, collect, receive, store, transport, treat, dispose and/or handle bio-medical waste in accordance with these rules and any guidelines issued by the Central Government;
 Act means the Environment (Protection) Act, 1986 (29 of 1986); (2) Animal House means a place where animals are reared/kept for experiments or testing purposes; (3) Authorisation means permission granted by the prescribed authority for the generation, collection, reception, storage, transportation, treatment, disposal and/or any other form of handling of bio-medical waste in accordance with these rules and any guidelines issued by the Central Government. (4) Authorised person means an occupier or operator authorised by the prescribed authority to generate, collect, receive, store, transport, treat, dispose and/or handle bio-medical waste in accordance with these rules and any guidelines issued by the Central Government;")
26
(10) "Schedule" means schedule appended to these rules;
(5) "Bio-medical waste" means any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or in research activities pertaining thereto or in the production or testing of biologicals, and including categories mentioned in Schedule I; (6) "Biologicals" means any preparation made from organisms or micro-organisms or product of metabolism and biochemical reactions intended for use in the diagnosis, immunisation or the treatment of human beings or animals or in research activities pertaining thereto; (7) "Bio-medical waste treatment facility" means any facility wherein treatment. disposal of bio-medical waste or processes incidental to such treatment or disposal is carried out; (8) "Occupier" in relation to any institution generating bio-medical waste, which includes a hospital, nursing home, clinic dispensary, veterinary institution, animal house, pathological laboratory, blood bank by whatever name called, means a person who has control over that institution and/or its premises; (9) "Operator of a bio-medical waste facility" means a person who owns or controls or operates a facility for the collection, reception, storage, transport, treatment, disposal or any other form of handling of bio-medical waste; (10) "Schedule" means schedule appended to these rules;
 Bio-medical waste means any waste, which is generated during the diagnosis, treatment or immunisation of human beings or animals or in research activities pertaining thereto or in the production or testing of biologicals, and including categories mentioned in Schedule I; (6) Biologicals means any preparation made from organisms or micro-organisms or product of metabolism and biochemical reactions intended for use in the diagnosis, immunisation or the treatment of human beings or animals or in research activities pertaining thereto; (7) Bio-medical waste treatment facility means any facility wherein treatment. disposal of bio-medical waste or processes incidental to such treatment or disposal is carried out; (8) Occupier in relation to any institution generating bio-medical waste, which includes a hospital, nursing home, clinic dispensary, veterinary institution, animal house, pathological laboratory, blood bank by whatever name called, means a person who has control over that institution and/or its premises; (9) Operator of a bio-medical waste facility means a person who owns or controls or operates a facility for the collection, reception, storage, transport, treatment, disposal or any other form of handling of bio-medical waste; (10) Schedule means schedule appended to these rules;")
27
4. DUTY OF OCCUPIER: It shall be the duty of every occupier of an institution generating bio-medical waste which includes a hospital, nursing home, clinic, dispensary, veterinary institution, animal house, pathological laboratory, blood bank by whatever name called to take all steps to ensure that such waste is handled without any adverse effect to human health and the environment. 5. TREATMENT AND DISPOSAL (1) Bio-medical waste shall be treated and disposed of in accordance with Schedule I, and in compliance with the standards prescribed in Schedule V. (2) Every occupier, where required, shall set up in accordance with the time-schedule in Schedule VI, requisite bio-medical waste treatment facilities like incinerator, autoclave, microwave system for the treatment of waste, or, ensure requisite treatment of waste at a common waste treatment facility or any other waste treatment facility.
 Bio-medical waste shall be treated and disposed of in accordance with Schedule I, and in compliance with the standards prescribed in Schedule V. (2) Every occupier, where required, shall set up in accordance with the time-schedule in Schedule VI, requisite bio-medical waste treatment facilities like incinerator, autoclave, microwave system for the treatment of waste, or, ensure requisite treatment of waste at a common waste treatment facility or any other waste treatment facility.")
28
6. SEGREGATION, PACKAGING, TRANSPORTATION AND STORAGE
(1) Bio-medical waste shall not be mixed with other wastes. (2) Bio-medical waste shall be segregated into containers/bags at the point of generation in accordance with Schedule II prior to its storage, transportation, treatment and disposal. The containers shall be labeled according to Schedule III. (3) If a container is transported from the premises where bio-medical waste is generated to any waste treatment facility outside the premises, the container shall, apart from the label prescribed in Schedule III, also carry information prescribed in Schedule IV. (4) Notwithstanding anything contained in the Motor Vehicles Act, 1988, or rules thereunder, untreated biomedical waste shall be transported only in such vehicle as may be authorised for the purpose by the competent authority as specified by the government. (5) No untreated bio-medical waste shall be kept stored beyond a period of 48 hours Provided that if for any reason it becomes necessary to store the waste beyond such period, the authorised person must take permission of the prescribed authority and take measures to ensure that the waste does not adversely affect human health and the environment
 Bio-medical waste shall not be mixed with other wastes. (2) Bio-medical waste shall be segregated into containers/bags at the point of generation in accordance with Schedule II prior to its storage, transportation, treatment and disposal. The containers shall be labeled according to Schedule III. (3) If a container is transported from the premises where bio-medical waste is generated to any waste treatment facility outside the premises, the container shall, apart from the label prescribed in Schedule III, also carry information prescribed in Schedule IV. (4) Notwithstanding anything contained in the Motor Vehicles Act, 1988, or rules thereunder, untreated biomedical waste shall be transported only in such vehicle as may be authorised for the purpose by the competent authority as specified by the government. (5) No untreated bio-medical waste shall be kept stored beyond a period of 48 hours. Provided that if for any reason it becomes necessary to store the waste beyond such period, the authorised person must take permission of the prescribed authority and take measures to ensure that the waste does not adversely affect human health and the environment.")
29
7. PRESCRIBED AUTHORITY (1) The Government of every State and Union Territory shall establish a prescribed authority with such members as may be specified for granting authorisation and implementing these rules. If the prescribed authority comprises of more than one member, a chairperson for the authority shall be designated. (2) The prescribed authority for the State or Union Territory shall be appointed within one month of the coming into force of these rules. (3) The prescribed authority shall function under the supervision and control of the respective Government of the State or Union Territory. (4) The prescribed authority shall on receipt of Form 1 make such enquiry as it deems fit and if it is satisfied that the applicant possesses the necessary capacity to handle bio-medical waste in accordance with these rules, grant or renew an authorisation as the case may be. (5) An authorisation shall be granted for a period of three years, including an initial trial period of one year from the date of issue. Thereafter, an application shall be made by the occupier/operator for renewal. All such subsequent authorisation shall be for a period of three years. A provisional authorisation will be granted for the trial period, to enable the occupier/operator to demonstrate the capacity of the facility.
 The Government of every State and Union Territory shall establish a prescribed authority with such members as may be specified for granting authorisation and implementing these rules. If the prescribed authority comprises of more than one member, a chairperson for the authority shall be designated. (2) The prescribed authority for the State or Union Territory shall be appointed within one month of the coming into force of these rules. (3) The prescribed authority shall function under the supervision and control of the respective Government of the State or Union Territory. (4) The prescribed authority shall on receipt of Form 1 make such enquiry as it deems fit and if it is satisfied that the applicant possesses the necessary capacity to handle bio-medical waste in accordance with these rules, grant or renew an authorisation as the case may be. (5) An authorisation shall be granted for a period of three years, including an initial trial period of one year from the date of issue. Thereafter, an application shall be made by the occupier/operator for renewal. All such subsequent authorisation shall be for a period of three years. A provisional authorisation will be granted for the trial period, to enable the occupier/operator to demonstrate the capacity of the facility.")
30
6) The prescribed authority may after giving reasonable opportunity of being heard to the applicant and for reasons thereof to be recorded in writing, refuse to grant or renew authorisation. (7) Every application for authorisation shall be disposed of by the prescribed authority within ninety days from the date of receipt of the application. (8) The prescribed authority may cancel or suspend an authorisation, if for reasons, to be recorded in writing, the occupier/operator has failed to comply with any provision of the Act or these rules : Provided that no authorisation shall be cancelled or suspended without giving a reasonable opportunity to the occupier/operator of being heard.
 Every application for authorisation shall be disposed of by the prescribed authority within ninety days from the date of receipt of the application. (8) The prescribed authority may cancel or suspend an authorisation, if for reasons, to be recorded in writing, the occupier/operator has failed to comply with any provision of the Act or these rules : Provided that no authorisation shall be cancelled or suspended without giving a reasonable opportunity to the occupier/operator of being heard.")
31
8. AUTHORISATION (1) Every occupier of an institution generating, collecting, receiving, storing, transporting, treating, disposing and/or handling bio-medical waste in any other manner, except such occupier of clinics, dispensaries, pathological laboratories, blood banks providing treatment/service to less than 1000 (one thousand) patients per month, shall make an application in Form 1 to the prescribed authority for grant of authorisation. (2) Every operator of a bio-medical waste facility shall make an application in Form 1 to the prescribed authority for grant of authorisation. (3) Every application in Form 1 for grant of authorisation shall be accompanied by a fee as may be prescribed by the Government of the State or Union Territory.
 Every occupier of an institution generating, collecting, receiving, storing, transporting, treating, disposing and/or handling bio-medical waste in any other manner, except such occupier of clinics, dispensaries, pathological laboratories, blood banks providing treatment/service to less than 1000 (one thousand) patients per month, shall make an application in Form 1 to the prescribed authority for grant of authorisation. (2) Every operator of a bio-medical waste facility shall make an application in Form 1 to the prescribed authority for grant of authorisation. (3) Every application in Form 1 for grant of authorisation shall be accompanied by a fee as may be prescribed by the Government of the State or Union Territory.")
32
9. ADVISORY COMMITTEE The Government of every State/Union Territory shall constitute an advisory committee. The committee will include experts in the field of medical and health, animal husbandry and veterinary sciences, environmental management, municipal administration, and any other related department or organisation including non-governmental organisations. The State Pollution Control Board/Pollution Control Committee shall be represented. As and when required, the committee shall advise the Government of the State/Union Territory and the prescribed authority about matters related to the implementation of these rules. 10. ANNUAL REPORT Every occupier/operator shall submit an annual report to the prescribed authority in Form 11 by 31 January every year, to include information about the categories and quantities of bio-medical wastes handled during the preceding year. The prescribed authority shall send this information in a compiled form to the Central Pollution Control Board by 31 March every year.

33
11. MAINTENANCE OF RECORDS
(1) Every authorised person shall maintain records related to the generation, collect ' ion, reception, storage, transporation, treatment, disposal and/or any form of handling of bio-medical waste in accordance with these rules and any guidelines issued. (2) All records shall be subject to inspection and verification by the prescribed authority at any time. 12. ACCIDENT REPORTING When any accident occurs at any institution or facility or any other site where bio-medical waste is handled or during transportation of such waste, the authorised person shall report the accident in Form Ill to the prescribed authority forthwith.
 Every authorised person shall maintain records related to the generation, collect ion, reception, storage, transporation, treatment, disposal and/or any form of handling of bio-medical waste in accordance with these rules and any guidelines issued. (2) All records shall be subject to inspection and verification by the prescribed authority at any time. 12. ACCIDENT REPORTING. When any accident occurs at any institution or facility or any other site where bio-medical waste is handled or during transportation of such waste, the authorised person shall report the accident in Form Ill to the prescribed authority forthwith.")
34
13. APPEAL Any person aggrieved by an order made by the prescribed authority under these rules may, within thirty days from the date on which the order is communicated to him, prefer an appeal to such authority as the Government of State/Union Territory may think fit to constitute : Provided that the authority may entertain the appeal after the expiry of the said period of thirty days if it is satisfied that the appellant was prevented by sufficient cause from filing the appeal in time.

35
SCHEDULE I (See Rule 5) CATEGORIES OF BIO-MEDICAL WASTE
 CATEGORIES OF BIO-MEDICAL WASTE")
36
The Hindu newspaper COIMBATORE, October 22, 2012 Bid to dump biomedical waste: Corpn. issues notice to hospital

39
BIOMEDICAL WASTE CATEGORIES
CAT1 HUMAN ANATOMICAL CAT2 ANIMAL CAT3 MICROBIOLOGY &BIOTECHNOLOGY CAT4 WASTE SHARPS CAT5 CYTOTOXICDRUGS & DISCARDED MEDICINES CAT6 SOILDWASTE CAT7 SOLID WASTE CAT8 LIQUID WASTE CAT9 INCINERATIONASH CAT10 CHEMICAL

40
COLOUR CODING AND TYPE OF CONTAINER FOR DISPOSAL OF BIO-MEDICAL WASTES
SCHEDULE II COLOUR CODING AND TYPE OF CONTAINER FOR DISPOSAL OF BIO-MEDICAL WASTES Colour Conding Type of Container -I Waste Category Treatment options as per Schedule I Yellow Plastic bag Cat. 1, Cat. 2, and Cat. 3, Cat. 6. Incineration/deep burial Red Disinfected container/plastic bag Cat. 3, Cat. 6, Cat.7. Autoclaving/Microwaving/ Chemical Treatment Blue/White translucent Plastic bag/puncture proof Cat. 4, Cat. 7. Container Chemical Treatment and destruction/shredding Black Plastic bag Cat. 5 and Cat. 9 and Cat. 10. (solid) Disposal in secured landfill Yellow
 Disposal in secured landfill. Yellow.")
44
BIOMEDICAL WASTES REGULATIONS
WASTE CAT 1,2,3 & 6 - YELLOW - PLASTIC BAGS INCINERATION & BURIEL WASTE CAT 3,6 & 7 - RED-DISINFEC CONT & PLASTIC BAGS - CHEMICAL DIS. AUTOCL, MICRO. CAT4 & 7 - BLUE /WHITE/TRANS-PLASTIC BAGS- - - CHEMCIAL ,SHREDDING, AUTOCL, MICRO, CAT5,9 &10 - BLACK-PLASTIC BAG - SECURED LANDFILL Lead Containers: These containers are used for collecting radioactive wastes This waste is to be disposed as per the guidelines provided by Bhabha Atomic Research Centre (BARC), Mumbai. Radioactive wastes, especially cobalt needles used for brachy treatment must be returned to BARC. Cytotoxic waste can be stored in sturdy cardboard boxes and later can be incinerated.
, Mumbai. Radioactive wastes, especially cobalt needles used for brachy treatment must be returned to BARC. Cytotoxic waste can be stored in sturdy cardboard boxes and later can be incinerated.")
46
LABEL FOR BIO-MEDICAL WASTE CONTAINERS/BAGS
SCHEDULE III LABEL FOR BIO-MEDICAL WASTE CONTAINERS/BAGS

48
OPTIMIZATION OF BIO-MEDICAL WASTE MANAGEMENT
Large health care units to have a treatment disposal facility of their own Large units with spare capacity in their to be shared with smaller units Treatment facilities to accept waste form small waste generators . Common Treatment Disposal Facilities under PPP. Local medical association to assist in cooperative ventures. State Govts. & municipal bodies to join hands Sites allotted for common incineration facilities Treated bio-medical wastes to be picked up by municipal bodies.

50
NEWER APPROACHES FOR BMW MANAGEMENT
Effective collection system to be put in place within and outside health care units Ensure proper segregation and packaging Pollution prevention thru EST Waste reduction Use of safe substitutes for hazardous subs in use

51
NEWER TECHNOLOGIES NEWER TECHNOLOGIES TO BE ADOPTED FOR BMW
NON INCINERATION TECHNOLOGY [AUTOCLAVING & HYDROCLAVING & MICROWAVING] USE OF REUSABLES WHERE POSSIBLE INSTEAD OF DISPOSABLES SAFE SUBSTITUTES FOR MERCURY MODERNIZATION OF THE OPERATING PLANTS

53
Waste minimization: Waste minimization is an important first step in managing wastes safely, responsibly and in a cost effective manner. This management step makes use of reducing, reusing and recycling principles. There are many possible routes to minimize the amount of both general waste and biomedical wastes within the health care or related facility. Alternative technologies for biomedical waste minimization (e.g., microwave treatment; hammer mill) have been investigated and are not considered to be practical. Some of the principles of waste minimization are listed below and will be developed further in the long-term strategy.

54
The training for handling of hospital waste is generally restricted within the waste handlers (Sweeper) this is the main obstruction to established a good INTEGRATED HOSPITAL WASTE MANAGEMENT PLAN. Biomedical waste generated by Doctors and paramedical staffs and segregation of waste at site of generation is the key factor to reduce the quantity of infected waste. If the infected waste is mixed with non-infected waste the quantity of infected waste becomes huge, unmanageable and almost impossible to dispose effectively. So Paramedical staff must be trained by the knowledgeable person so that they can handle the infected waste in efficient manner. Due training should be given with refresher course in certain intervals. Color coated bins and bin liners should be placed at the points of generation. For better understanding of segregation. Matter should be placed in such a manner that the staffs should feel that following the system will give them a better life to live with their families. The necessary equipments should be given to them. If the segregation system is up to the mark than this has been observed that 85 to 90% of the total waste becomes non infected only 10 to 15% are infected waste which need special disposal system. Incineration/Deep burial. Per day in-house patient generate 1.5Kg of waste only 10 to 15% of which is infected waste. Radiology department generate radioactive waste. Handling of radioactive waste requires special attention and skill.

55
Training to word boys:-
They respond well when it connected to their day to day problem. The best idea is to listen to their problem sympathetically then they will be more open to the session. Written words are best abandoned with this group. Best way to create interest is audio/visual method. This group can come out with valuable suggestions if proper attention is given to them. Training to the Doctors:- Without having national and international research report in hand /audiovisual format it will create very very less effect to them. They require more academic approach with working example to other institution. Often this has been observed that doctors feel s that this type of season is imposition to them. Their time should be respected. Training to the paramedical:-They are the backbone of the waste management system of the hospital. To train them is a critical subject. Nurses are interested, active but due to duty schedule they are in hurry. Time should be chosen when they are free and a smart and good commutating skilled trainer should be placed to this group with audiovisual system to demonstrate the good practices effectively. Language sometime become problem. Trainer should know the local languages or he/she can take help.

56
SCHEDULE IV (see Rule 6) LABEL FOR TRANSPORT OF BIO-MEDICAL WASTE CONTAINERS/BAGS Day Month Year Date of generation

59
SCHEDULE V (see Rule 5 and Schedule 1) STANDARDS FOR TREATMENT AND DISPOSAL OF BIO-MEDICAL WASTES STANDARDS FOR INCINERATORS: All incinerators shall meet the following operating and emission standards A. Operating Standards

67
SCHEDULE VI SCHEDULE FOR WASTE TREATMENT FACILITIES LIKE INCINERATOR/ AUTOCLAVE/ MICROWAVE SYSTEM A Hospitals and nursing homes in towns with population of 30 lakhs by 31st December, 1999 or earlier and above B. Hospitals and nursing homes in towns with population of below 30 lakhs, (a) with 500 beds and above by 31st December, 1999 or earlier (b) with 200 beds and above but less than 500 beds by 31st December, 2000 or earlier (c) with 50 beds and above but less than 200 beds by 31st December, 2001 or earlier (d) with less than 50 beds by 31st December, 2002 or earlier C. All other institutions generating bio-medical waste not included by 31st December, 2002 or earlier in A and B above
 with 500 beds and above by 31st December, 1999 or earlier (b) with 200 beds and above but less than 500 beds by 31st December, 2000 or earlier. (c) with 50 beds and above but less than 200 beds by 31st December, 2001 or earlier. (d) with less than 50 beds by 31st December, 2002 or earlier C. All other institutions generating bio-medical waste not included by 31st December, 2002 or earlier in A and B above")
74
Section 8 permits the education of individuals dealing with hazardous wastes regarding various safety measures. Section 10 bestows authority to enter the premises and inspect. Section 15 allows the government to take punitive steps against defaulters. This involves imprisonment up to five years or penalty of upto rupees one lakh or both. In case the default continues, it would then attract a penalty of rupees five thousand per day up to one year and thereafter imprisonment up to seven years. Section 17 provides for punishment in case of violations by government departments.

75
FORM I (see rule 8) APPLICATION FOR AUTHORISATION (To be submitted in duplicate.) To The Prescribed Authority (Name of the State Govt/UT Administration) Address. 1. Particulars of Applicant
 Address. 1. Particulars of Applicant.")
80
FORM II (see rule 10) ANNUALREPORT (To be submitted to the prescribed authority by 31 January every year). 1 . Particulars of the applicant:

86
FORM III (see Rule 12) ACCIDENT REPORTING 1. Date and time of accident: 2. Sequence of events leading to accident 3. The waste involved in accident : 4. Assessment of the effects of the accidents on human health and the environment,.

87
One of the features of the new rules is that now every occupier
. BMW Rules 2011 vs. 1998 One of the features of the new rules is that now every occupier 2011 1998 Every occupier generating BMW, irrespective of the quantum of wastes comes under the BMW Rules and requires to obtain authorisation Occupiers with more than 1000 beds required to obtain authorisation Duties of the operator listed Operator duties absent Categories of Biomedical Waste reduced to Eight Biomedical waste divided in ten categories Treatment and disposal of BMW made mandatory for all the HCEs Rules restricted to HCEs with more than 1000 beds A format for annual report appended with the Rules No format for Annual Report Form VI i.e. the report of the operator on HCEs not handing over the BMW added to the Rules Form VI absent

88
“Such a change has been proposed because earlier hospitals did not give a clear picture of the number of patients being served and thus evaded authorization and were exempted from treating their wastes. It was also difficult to ascertain the number of patients being treated in any hospital” The new Rules have incorporated State Ministry of Health for grant of license to Health Care Establishments (HCEs) HCEs after they get authorization from the SPCBs. The new Rules have bridged the gap since earlier the HCEs only required to obtain license from State Ministry of Health and carried out their functions but now they have to obtain prior authorization before commencing their activities. SPCBs would make sure that the HCEs have the necessary capacity and adequate equipments and then grant them the authorization or renew their authorization.
 HCEs after they get authorization from the SPCBs. The new Rules have bridged the gap since earlier the HCEs only required to obtain license from State Ministry of Health and carried out their functions but now they have to obtain prior authorization before commencing their activities. SPCBs would make sure that the HCEs have the necessary capacity and adequate equipments and then grant them the authorization or renew their authorization.")
89
Occupier and Operators duties flagged Duties of the occupier have been elaborated in the present Rules. Proper training has to be imparted by the occupier to the health care workers engaged in handling BMW. The training for staff involved in the hospital waste management involves a number of parameters. The Rules merely mention proper training but there are no details as such on what kind of training should be imparted to the health care workers. A set of guidelines or regulations needs to be drafted by the HCEs in consultation with health and safety experts as a part of training module Apart from the duties of the occupier the present rules have also listed duties for the operators of common BMW treatment facility. The operators now have to ensure that the BMW is collected from all the HCEs and is transported, handled, stored, treated and disposed in an environmentally sound manner. The operators also have to inform the prescribed authority if any HCEs are not handing the segregated BMW as per the guidelines prescribed in the rules. Accident reporting a must Accidents that take place during the management of wastes have been defined in the new Rules. Accidents like injuries from sharps, mercury spills and fire hazards now have to be reported in Form III along with the remedial action taken. The Rules have also made mandatory for all the HCEs with 30 or more beds to set up a cell or unit to deal with the BMW management. The cell has to meet every six months and minutes of the meeting have to be submitted along with the Annual Report to the prescribed authority. “The move to set up a cell for BMW handling and making them meet every six months and reporting was initiated since most of the hospitals in various states did not had a separate unit to deal with such wastes”

90
Mandatory treatment and disposal The new Rules have made the treatment and disposal of Bio Medical wastes mandatory for all the institutions generating them. The Rules clearly mention that every occupier should set up adequate treatment facilities like autoclave/microwave/incinerator/hydroclave, shredder prior to commencement of its operation or ensure that the wastes are treated at a common bio medical waste treatment facility or an authorized waste treatment facility. Another conspicuous feature of the rule is the clause on promotion of new technologies. the new Rules have omitted incinerator as one of the pre requisites for on-site treatment of BMW. The omission is owing to the various environmental impacts of incineration. The new Rules say that the occupier having 500 or more beds may install incinerator subject to compliance of all the guidelines. Incinerators can be allowed for a cluster of hospitals or positioned in major part of cities so that HCEs can transport their waste to them instead of having one. Deep burial for disposal of BMW has also been removed from the Rules. The Rules says it can be an option only in rural areas with no access to CTF with prior approval from the prescribed authority. However it is not mentioned in the rules as to what kind of wastes can be deep buried. New rules have included a clause saying that the occupier or operators now have to monitor the stack emissions from incinerator quarterly as per the norms specified and the results have to be recorded and submitted to the prescribed authority. Reporting the results of emissions would help operators and occupiers to achieve compliance and strive for further improvement in the operation of incinerator.

91
Ambiguities cleared The Bio Medical Waste (Management and Handling) Rules 1998 contained ten categories of wastes which have been reduced in the present rules to eight. The 2011 Rules have discarded Category No. 8 (containing liquid waste generated from laboratory, cleaning, washing and disinfection activities) and Category No. 9 (containing incineration ash). However, laboratory wastes listed in Category 8 has been included in the present Category 3. The current rules have also cleared the confusion over the colour coding of the containers used for disposal of BMW. The Schedule II of the 1998 Rules creates a confusion regarding the disposal of Category 3 and Category 6 wastes which could either be disposed in yellow or red coloured bags. Similarly, Category 7 wastes could also be disposed in red or blue bags. The present Rules have thus clarified the ambiguity and allotted one colour code to each category of waste.
 and Category No. 9 (containing incineration ash). However, laboratory wastes listed in Category 8 has been included in the present Category 3. The current rules have also cleared the confusion over the colour coding of the containers used for disposal of BMW. The Schedule II of the 1998 Rules creates a confusion regarding the disposal of Category 3 and Category 6 wastes which could either be disposed in yellow or red coloured bags. Similarly, Category 7 wastes could also be disposed in red or blue bags. The present Rules have thus clarified the ambiguity and allotted one colour code to each category of waste..")
92
Colour Coding and Type of Container for Disposal of BMW
Type of container to be used Waste Category Number Yellow Non Chlorinated plastic bags Category 1,2,5,6 Red Non Chlorinated plastic bags/puncture proof container for sharps Category 3,4,7 Blue Non Chlorinated plastic bags container Category 8 Black Municipal Apart from the various categories of wastes, Schedule II of the Rules has also incorporated the storage and disposal of municipal solid waste (MSW) generated from the hospitals. The Rules expounds that the MSW such as paper waste, food waste and other non infectious wastes generated from the hospitals should be stored in black coloured bags/containers and disposed as per the Municipal Solid Waste (Management and Handling) Rules 2000.
 generated from the hospitals. The Rules expounds that the MSW such as paper waste, food waste and other non infectious wastes generated from the hospitals should be stored in black coloured bags/containers and disposed as per the Municipal Solid Waste (Management and Handling) Rules")
93
Loose protocol for cytotoxic drugs it has been lax in drafting a proper protocol for cytotoxic drugs. Discarded medicines and cytotoxic drugs comprise Category no. 5 in the Schedule 1 of the Rules and are described as wastes consisting of outdated, contaminated and discarded medicines. Cytotoxic drugs are drugs that are used in the treatment of cancer and are used in the chemotherapy. It is termed so because it is toxic to the cells and inhibits the growth of cancer cells. The present Rules have neglected the severity of exposure to cytotoxic drugs and the perils of unsafe disposal of such drugs. It is highly toxic and extreme care is required in the handling of such drugs for treatment and disposal. The occupier should provide a thorough training and information explaining in detail the hazards of cytotoxic drugs to the people handling such wastes in their facilities. Hospitals should devise safest and best available system for the management of such toxic waste. a separate protocol for collection, packaging, storage, treatment and disposal of cytotoxic drugs.

94
Rules also fails to give proper guidelines on the disposal of bed linens and mattresses which are discarded after certain period of use. According to the rules the linens and mattresses comes under Category no. 6 and incineration is suggested for treatment and disposal. “Soiled linen and mattresses may contain pathogenic microorganisms from one diseased person which can easily be transferred to the other patients using it. However owing to its bulkiness it is difficult to dispose it off” Incineration for such wastes is not a feasible option, a separate mechanism to dispose linens and mattresses should be devised and incorporated in the rules.

95
One of the directives in the rules talks about setting up of ‘District Level Monitoring Committees’ in the districts to scrutinize the compliance to the new Rules in the hospitals and other agencies generating BMW and facilities engaged in treatment and disposal of BMW. As per the rules, the District Level Monitoring Committee would be headed by District Medical Officer or his nominee. The Committee is also entrusted with the task to prepare and submit a half yearly report on the status of health care facilities lying in its jurisdiction to the State Level Advisory Committee. A copy of the report should also be sent to Central Pollution Control Board or Ministry of Environment and Forests and State Pollution Control Board/Pollution Control Committee as the case may be for necessary action.

96
The Rules have also considered the Government hospitals and their lack of capacity and resources. These hospitals generally charge pittance and serve a large proportion of populace. Managing the BMW wastes in these hospitals would require adequate infrastructure, manpower and expertise which they lack. The Rules have instructed the State Government or Union Territory to allocate separate funds to all such health care facilities for appropriate management of their BMW. The State Government is also instructed to procure and allocate treatment equipments for government HCEs.

97
Technology options for ‘treatment’
There are mainly five technology options available for the treatment of Bio-Medical Waste or still under research can be grouped as 1. Chemical processes 2. Thermal processes 3. Mechanical processes 4. Irradiation processes 5. Biological processes 1. Chemical processes These processes use chemical that act as disinfectants. Sodium hypochlorit, dissolved chlorine dioxide, peracetic acid, hydrogen peroxide, dry inorganic chemical and ozone are examples of such chemical. Most chemical processes are water-intensive and require neutralising agents. 2. Thermal processes These processes utilise heat to disinfect. Depending on the temperature they operate it is been grouped into two categories, which are Low-heat systems and High-heat systems Low-heat systems (operates between °C) use steam, hot water, or electromagnetic radiation to heat and decontaminate the waste. Autoclave & Microwave are low heat systems. Autoclaving is a low heat thermal process and it uses steam for disinfection of waste. Autoclaves are of two types depending on the method they use for removal of air pockets are gravity flow autoclave and vacuum autoclave. Microwaving is a process which disinfect the waste by moist heat and steam generated by microwave energy
 use steam, hot water, or electromagnetic radiation to heat and decontaminate the waste. Autoclave & Microwave are low heat systems. Autoclaving is a low heat thermal process and it uses steam for disinfection of waste. Autoclaves are of two types depending on the method they use for removal of air pockets are gravity flow autoclave and vacuum autoclave. Microwaving is a process which disinfect the waste by moist heat and steam generated by microwave energy.")
102
High-heat systems (operates between 540-8,300°C) employ combustion and high temperature plasma to decontaminate and destroy the waste. Incinerator & Hydroclaving are high heat systems. Hydroclaving - is steam treatment with fragmentation and drying of waste

103
INCINERATION Waste collected in yellow containers is incinerated. Waste categorized as Human Anatomical Waste and Animal Waste is incinerated. Human Anatomical Waste includes human tissues, organs, and body parts. Animal waste includes animal tissues, organs, body parts, carcasses, bleeding parts, experimental animals used in research, and waste generated by veterinary hospitals and colleges, and animal houses.

107
Primary Chamber is designed to burn the waste at 800 Deg C.
Secondary Chamber is designed to burn the waste at 1050 Deg C. The incinerator has oil fired burners. The incinerator is designed for operation under excess air conditions. Combustion under excess air conditions ensures complete destruction of dioxins and furans and produces smokeless flue gases.

115
3. Mechanical processes These processes are used to change the physical form or characteristics of the waste either to facilitate waste handling or to process the waste in conjunction with other treatment steps. The two primary mechanical processes are Compaction - used to reduce the volume of the waste Shredding - used to destroy plastic and paper waste to prevent their reuse. Only the disinfected waste can be used in a shredder.

117
4. Irradiation processes
exposes wastes to ultraviolet or ionizing radiation in an enclosed chamber. These systems require post shredding to render the waste unrecognizable. 5. Biological processes - using biological enzymes for treating medical waste. It is claimed that biological reactions will not only decontaminate the waste but also cause the destruction of all the organic constituents so that only plastics, glass, and other inert will remain in the residues.

118
Types of Composting can be considered for BMW
Vermicomposting Enhanced Microbial Composting Windrows Composting In- vessel Composting Bin Composting Rotating Drum Composting Transportable Composting Aerobic Composting Anaerobic Composting

119
VERMICOMPOSTING Using of earth worms for composting organic residue. The excreta (castings) of the worms are rich in nitrate, available forms of P, K, Ca and Mg. The passage of soil through earthworms promotes the growth of bacteria and actinomycetes. Actinomycetes thrive in the presence of worms and their content in worm casts is more than six times that in the original soil.
 of the worms are rich in nitrate, available forms of P, K, Ca and Mg. The passage of soil through earthworms promotes the growth of bacteria and actinomycetes. Actinomycetes thrive in the presence of worms and their content in worm casts is more than six times that in the original soil.")
120
ENHANCED MICROBIAL COMPOSTING
INOCULATION Inoculum organisms utilized for composting are mainly fungi such as Trichoderma sp. and Pleurotus sp. The microbial inoculant contains microbial consortia (group) with different microorganism targeting different substrate. The promising (useful) microbes are Pleurotus, Trichoderma, Bacillus, Pseudomonas and Streptomyces.
 with different microorganism targeting different substrate. The promising (useful) microbes are Pleurotus, Trichoderma, Bacillus, Pseudomonas and Streptomyces.")
121
Bio- compost process In the bio-compost process, temperature is raised upto 700C in the initial days to kill all the pathogenic organism and weed (wide) seed. Moisture is maintained 60 % and particle size is reduced upto 2 cm are the important process in biocomposting. Turning the compost material once in 10 days will enhance the composting process. All biodegradable waste will be put into biocompost process to get good organic manure.
 seed. Moisture is maintained 60 % and particle size is reduced upto 2 cm are the important process in biocomposting. Turning the compost material once in 10 days will enhance the composting process. All biodegradable waste will be put into biocompost process to get good organic manure.")
122
ENHANCED MICROBIAL COMPOSTING
Types of Pleurotus species Pleurotus ostreatoroseus Pleurotus ostreatus Pleurotus citrinopileatus Pleurotus cornucopiae Pleurotus flabellatus Pleurotus sajor-caju Pleurotus pulmonarius

123
Wind-rows Composting Wind-row composting consists of placing the mixture of raw materials in long narrow piles called wind-rows that are agitated or turned on a regular basis. Wind-rows aerate primarily by natural or passive air movement (convection and gaseous diffusion). For small- to moderate-scale operations, turning can be accomplished with a front-end loader or a bucket loader on a tractor.
. For small- to moderate-scale operations, turning can be accomplished with a front-end loader or a bucket loader on a tractor.")
124
Passively Aerated Wind-rows
In this method, air is supplied to the composting materials through perforated pipes for turning. Air flows into the pipes and through the wind-row. Because of the chimney effect created hot gases rise upward out of the wind-row. The wind-rows are generally formed by the procedures described for the aerated static pile method. It is important to avoid compaction of materials while constructing the wind-row. Aeration pipes are placed on top of the peat/compost base. When the composting period is completed, the pipes are removed.

125
Passively Aerated Wind-rows

126
A DISSERTATION PRESENTATION ON BIO-MEDICAL WASTE MANAGEMENT USING VERMI-COMPOSTING TECHNIQUE AT SHREE KRISHNA HOSPITAL. Work completed In 2005 August

127
GRAPHIC DISPLAY OF BIO-MEDICAL WASTE
TOTAL HOSPITAL WASTE % NON HAZARDOUS WASTE % INFECTIOUS WASTE % NON INFECTIOUS WASTE (BUT HAZARDOUS) 5%
 5%")
128
Average Composition of Hospital waste in India
Sr.No. Material % ( Wet wt.tons) 1 Paper 15 2 Plastic 10 3 Rags 4 Metals( shraps etc.) 5 Infectious waste 1.5 6 Glass 7 General waste 53.5
 1. Paper Plastic Rags. 4. Metals( shraps etc.) 5. Infectious waste Glass. 7. General waste")
129
Vermicomposting : Concept to Commissioning
The term vermicomposting means the use of earthworms for composting organic residues. Red worms : “Red wigglers, red hybrid, tiger worm, garlic worm, brandling worm, or manure worms.” The Latin name for these worms is Eisenia foetida

130
Why Vermicomposting Experimental Set-up : Ecofriendly, Economical
Reusable. Experimental Set-up : Containers Bedding Water Red worms Non fatty kitchen scraps, blood soaked cottons and sanitary napkins

131
Sample 1 : 30% Kitchen waste + 70% Cow dung
TEST RESULTS : Sample 1 : 30% Kitchen waste + 70% Cow dung Sample N P K M.C. O.C. pH % Before degradation 0.568 0.412 0.347 82.0 13.92 6.82 24.5 After 15days 0.616 0.435 0.349 66.2 13.22 7.03 21.46 After 30days 0.784 0.477 0.18 41.2 12.52 6.81 15.96 C/N

133
Sample 2 : 10% Kitchen waste +Blood soaked cotton,
sanitary napkins + 90% Cow dung Sample No. 2 N P K M.C. O.C. pH C/N % Before degradation 0.981 0.396 0.15 44.8 49.15 6.75 50.46 After 15days 0.863 0.408 0.151 50.2 31.86 6.88 36.92 After 30days 0.652 0.39 0.143 30.4 27.84 8.13 42.69

135
Sample 3 : 10% Kitchen waste + 90% Cow dung
Sample No.3 N P K M.C. O.C. pH C/N % Before degradation 0.504 0.486 0.301 77.2 24.15 7.05 47.91 After 15days 0.536 0.501 0.314 65.4 22.04 7.46 41.11 After 30days 1.092 0.516 0.319 45.4 19.02 6.86 17.41

137
Sample 4 : 100% Cow dung Sample No.4 N P K M.C. O.C. pH C/N %
% Before degradation 0.700 0.666 0.18 37.3 23.73 7.57 33.85 After 15days 0.812 0.781 0.322 39.4 19.72 8.02 24.28 After 30days 1.578 1.197 0.643 50.3 16.298 6.72 10.37

139
technique fairly and satisfactorily in all the bioreactor except the
General bio-medical waste was treated by vermicomposting technique fairly and satisfactorily in all the bioreactor except the bioreactor 2,which contained blood soaked cotton, sanitary napkins with kitchen waste. The degradation in bioreactor 2 could not be completed, as the red worms died after 12 days and the waste became anaerobic. Probable reasons for this can be, there might be an infectious agent present in the waste, also owing to blood soaked cotton and sanitary napkins, Oxygen demand was increased. In accordance with the demand of oxygen v/s. supply of oxygen was not balanced. As aerobic organism requires oxygen proportionately higher than the polluting load. Imbalance factor occurred there. Owing to insufficient supply of oxygen, the aerobic organism turned to anerobic condition. There was a reduction in C/N ratio within 15days in bio-reactor 2 and then after, increment in C/N ratio indicates that mixture was little bit degraded. It indicates that lack of aeration was the cause of this damage

141
Preliminary studies were carried out from vermicomposting beds, each measuring3.5ft.x3.5ft x1ft., lined by a single layer of earthen tiles made on a cemented floor in a few rooms having asbestos sheets ceiling. Twelve such beds were used for studies. These beds were charged with infected biodegradable waste comprising of cotton/gauze pieces soiled with blood, pus and body fluids etc. In many cases it would have been admixed with antiseptics/antibiotics used for dressing of wounds etc. It was covered with dry leaves after watering and admixing with an adequate number of earthworms (Eisenia fetida and Eudrilus eugeniae). They were left undisturbed for vermicomposting and compost thus formed later was subjected to aerobic microbiological cultures at periodic intervals till full composting took place
. They were left undisturbed for vermicomposting and compost thus formed later was subjected to aerobic microbiological cultures at periodic intervals till full composting took place.")
144
Journal Article ECOFRIENDLY TREATMENT OF BIOMEDICAL WASTES USING EPIGEIC EARTHWORMS M.S. Dinesh, Geetha K.S, Vaishnavi V, Radha D. Kale, V. Krishna Murthy Journal of Indian Society of Hospital Waste Management 09/2010; 9(1):5-20. Biomedical waste (BMW) treatment by incineration and disposal of the resultant ash in landfills is the most widely used process. There is growing interest to adopt alternative technologies. The present study was carried out to evolve an environmental friendly method to treat biodegradable part of biomedical waste collected from local hospital using vermicomposting. Biomedical waste was collected after onsite treatment with 5%NaOCl as a safety measure. It was subjected to initial decomposition process by mixing with cow dung slurry in the culture tubs maintained in the vermiculture unit of the laboratory. Initially decomposed BMW was fed to epigeic earthworms in monoculture and polyculture practices to screen suitable vermicomposting method. Natural composting was considered as control. Two cycles of vermicomposting was done using fresh BMW each time. Nutrient levels and storage studies of vermicompost and natural compost were also carried out. Statistical analysis was worked out to find out the most suitable treatment method. Results revealed that the vermicomposting of BMW was comparatively more efficient than natural composting. The performance efficiencies of earthworms in different treatments were as follows: Eisenia fetida > Mixed culture> Eudrilus eugeniae > Perionyx excavatus. It was also found that repeating the same set of earthworms for successive cycle showed improved rate of vermicomposting. Since the complexity and toxicity levels of BMW produced at different hospitals vary, it is recommended to treat BMW by vermicomposting using a mixed culture of all three epigeic earthworms. It is also essential to gradually expose them to the waste to make them adapt to this toxic material. Vermicomposting with proper handling of BMW can be an energy efficient ecofriendly approach for reducing and recycling of this hazardous waste. Bioresource Technology. 2003; 88(3): K a v i r a j a n d S h a r m a S . M u n i c i p a l s o l i d w a s t e m a n a g e m e n t t h r o u g h v e r m i c o m p o s t i n g e m p l o y i n g e x o t i c a n d l o c a l s p e c i e s o f e a r t h w o r m s . Bioresource Technology. 2003; 90(2): Journal of ISHWM Vol. 9 Issue 1 September Full-text sources View Available from Vaishnavi Venugopalan 2 Jul 2012 ISHWM-Vol 9 Issue 1 Apr 2010.pdf Available from Vaishnavi Venugopalan · 2 Jul 2012 Jobs See more Senior Medical / Pharmaceutical Sales Rep Position: Sales Professional Employer: Quintiles NASA Postdoctoral Fellowships Position: PostDoc Position Employer: NASA / ORAU Keywords biodegradable part biomedical waste culture tubs decomposed BMW different treatments Eisenia fetida fresh BMW hazardous waste initial decomposition process local hospital mixed culture Nutrient levels polyculture practices screen suitable vermicomposting method storage studies successive cycle suitable treatment method three epigeic earthworms toxic material toxicity levels Vaishnavi Venugopalan Jacobs University © 2013 researchgate.net. All rights reserved. About us · Contact us · News · Privacy · Terms Already a member? Log in Log in Password Forgot password? Keep me logged in No Yes Are you a researcher? Best matches for biomedical waste vermicomposting Two cycles of vermicomposting was done using fresh BMW each time. Jump to text » More matches » « Fewer matches
:5-20. Biomedical waste (BMW) treatment by incineration and disposal of the resultant ash in landfills is the most widely used process. There is growing interest to adopt alternative technologies. The present study was carried out to evolve an environmental friendly method to treat biodegradable part of biomedical waste collected from local hospital using vermicomposting. Biomedical waste was collected after onsite treatment with 5%NaOCl as a safety measure. It was subjected to initial decomposition process by mixing with cow dung slurry in the culture tubs maintained in the vermiculture unit of the laboratory. Initially decomposed BMW was fed to epigeic earthworms in monoculture and polyculture practices to screen suitable vermicomposting method. Natural composting was considered as control. Two cycles of vermicomposting was done using fresh BMW each time. Nutrient levels and storage studies of vermicompost and natural compost were also carried out. Statistical analysis was worked out to find out the most suitable treatment method. Results revealed that the vermicomposting of BMW was comparatively more efficient than natural composting. The performance efficiencies of earthworms in different treatments were as follows: Eisenia fetida > Mixed culture> Eudrilus eugeniae > Perionyx excavatus. It was also found that repeating the same set of earthworms for successive cycle showed improved rate of vermicomposting. Since the complexity and toxicity levels of BMW produced at different hospitals vary, it is recommended to treat BMW by vermicomposting using a mixed culture of all three epigeic earthworms. It is also essential to gradually expose them to the waste to make them adapt to this toxic material. Vermicomposting with proper handling of BMW can be an energy efficient ecofriendly approach for reducing and recycling of this hazardous waste. Bioresource Technology. 2003; 88(3): K a v i r a j a n d S h a r m a S . M u n i c i p a l s o l i d w a s t e m a n a g e m e n t t h r o u g h v e r m i c o m p o s t i n g e m p l o y i n g e x o t i c a n d l o c a l s p e c i e s o f e a r t h w o r m s . Bioresource Technology. 2003; 90(2): Journal of ISHWM Vol. 9 Issue 1 September Full-text sources. View Available from Vaishnavi Venugopalan. 2 Jul ISHWM-Vol 9 Issue 1 Apr 2010.pdf. Available from Vaishnavi Venugopalan · 2 Jul Jobs See more. Senior Medical / Pharmaceutical Sales Rep. Position: Sales Professional. Employer: Quintiles. NASA Postdoctoral Fellowships. Position: PostDoc Position. Employer: NASA / ORAU. Keywords. biodegradable part. biomedical waste. culture tubs. decomposed BMW. different treatments. Eisenia fetida. fresh BMW. hazardous waste. initial decomposition process. local hospital. mixed culture. Nutrient levels. polyculture practices. screen suitable vermicomposting method. storage studies. successive cycle. suitable treatment method. three epigeic earthworms. toxic material. toxicity levels. Vaishnavi Venugopalan. Jacobs University. © 2013 researchgate.net. All rights reserved. About us · Contact us · News · Privacy · Terms. Already a member Log in Log in. . Password Forgot password Keep me logged in. No Yes Are you a researcher Best matches for biomedical waste vermicomposting. Two cycles of vermicomposting was done using fresh BMW each time. Jump to text » More matches » « Fewer matches.")
145
Sampling . Collection of bio-medical wastes:
Bio-medical waste (45kg) was collected from K.S. Hospital, BSK 3rd Stage, Bangalore, India and was used as and when required for the experimentation. For each of the cycle of vermicomposting, 20 kg of BMW was utilized and 5 kg of BMW was used as control (natural composting). Only the biodegradable matter of the infected BMW was considered for the experiment.. This included blood stained cotton pieces, pus and body fluids, antiseptics/antibiotics used for dressing of wounds, spilled liquid and tissues collected from operation tables. They were subjected to the preliminary treatment onsite to reduce the probable hazardous effect. Similar procedures were followed in previous literature [14]. 2. Preliminary on-site treatment of BMW: The BMW used for the experiment was chemically sterilized on-site using 5% of 1N NaOCl as suggested in previous works [15]. This was done to disinfect the BMW before subjecting it to vermicomposting and natural composting. 3. Primary decomposition of disinfected BMW: Following the chemical treatment, the disinfected BMW was made palatable or more suitable for the earthworm species to feed [16]. Primary decomposition of BMW was carried out in laboratory for a period of 15 days as follows: 3.1 Preparation of cow dung slurry: A homogenous mixture of cow dung slurry was prepared at 1:4 (w/v) ratios by mixing 250 g of cow dung with 1 L of distilled water. Five liters of the slurry was prepared and maintained in five separate containers containing 1L slurry in each forf further use.
 was collected from K.S. Hospital, BSK 3rd Stage, Bangalore, India and was used as and when required for the experimentation. For each of the cycle of vermicomposting, 20 kg of BMW was utilized and 5 kg of BMW was used as control (natural composting). Only the biodegradable matter of the infected BMW was considered for the experiment.. This included blood stained cotton pieces, pus and body fluids, antiseptics/antibiotics used for dressing of wounds, spilled liquid and tissues collected from operation tables. They were subjected to the preliminary treatment onsite to reduce the probable hazardous effect. Similar procedures were followed in previous literature [14]. 2. Preliminary on-site treatment of BMW: The BMW used for the experiment was chemically sterilized on-site using 5% of 1N NaOCl as suggested in previous works [15]. This was done to disinfect the BMW before subjecting it to vermicomposting and natural composting. 3. Primary decomposition of disinfected BMW: Following the chemical treatment, the disinfected BMW was made palatable or more suitable for the earthworm species to feed [16]. Primary decomposition of BMW was carried out in laboratory for a period of 15 days as follows: 3.1 Preparation of cow dung slurry: A homogenous mixture of cow dung slurry was prepared at 1:4 (w/v) ratios by mixing 250 g of cow dung with 1 L of distilled water. Five liters of the slurry was prepared and maintained in five separate containers containing 1L slurry in each forf further use.")
146
3.2 Mixing of BMW with cow dung slurry: To each of the five containers with 1L cow dung slurry, 5 kg of BMW was added and mixed (at 5:1, BMW : Cow dung slurry ratio w/v). The mixture was allowed to undergo primary decomposition for a period of 15 days in the laboratory. The same procedure was carried out to prepare the control tank. It was also done to facilitate the consumption of BMW by epigeic earthworms during the process of vermicomposting. The process of preliminarily on-site treatment and primary decomposition was carried out for every fresh batch of BMW used for vermicomposting. 4. Tank preparation: 4.1 Preparation of tanks for vermicomposting and natural composting Four plastic tanks were maintained to carry out the process of vermicomposting. Each tank used for the experiment measured 1M long, 0.5M broad and 0.5m deep. A tank containing only 5kg primary decomposed BMW but without introduction of any earthworm species was maintained as control and allowed to undergo natural composting for a period of 45 days. The mix used for the study to begin with was measured for pH, moisture content and temperature. The initial measured pH was 6.3, temperature 250 C and 60% moisture Collection of suitable epigeic earthworms: The epigeic earthworm species namely Eisenia fetida, Eudrilus eugeniae and Perionyx excavatus were used for the study. These species were collected from the Department of Agricultural Microbiology, University of Agriculture, GKVK,Bangalore Release of earthworms into tanks: To each of the four tanks maintained for vermicomposting, 5kg of primarily decomposed BMW (previously prepared and maintained in laboratory) was added. Three tanks were used as monoculture tanks (single species per tank) while one was used as a polyculture tank (all three species in tank). Hundred adult earthworms each of Eisenia fetida, Eudrilus eugeniae and Perionyx excavatus were released into the monoculture tanks respectively. The polyculture tank had 33 adults of each of E. fetida, E. eugeniae and P.excavatus. After the first cycle of vermicomposting, the recovered/survived earthworms (both adult and juveniles) from the respective tanks were used for another cycle of vermicomposting (45 days) using fresh primarily decomposed BMW
 was added. Three tanks were used as monoculture tanks (single species per tank) while one was used as a polyculture tank (all three species in tank). Hundred adult earthworms each of Eisenia fetida, Eudrilus eugeniae and Perionyx excavatus were released into the monoculture tanks respectively. The polyculture tank had 33 adults of each of E. fetida, E. eugeniae and P.excavatus. After the first cycle of vermicomposting, the recovered/survived earthworms (both adult and juveniles) from the respective tanks were used for another cycle of vermicomposting (45 days) using fresh primarily decomposed BMW.")
147
CONCLUSION The present study reveals that vermicomposting is a efficient and ecofriendly technique for management of biomedical wastes, in comparison to normal composting. A study carried out using different species of earthworms independently and as mixed culture for vermicomposting of BMW showed that E. fetida is more efficient than the other two epigeic earthworm species E. eugeniae and P. excavatus. A mixed culture of all the three species was as efficient as that of E. fetida. It is advisable to maintain a polyculture of earthworms to treat BMW since all three species work in unison to decompose the waste and even if one of the species fails to survive in the toxic and complex BMW environment, the surviving species would be able to carry out the process efficiently.

149
Health hazardous of Biomedical wastes

150
Health hazards According to the WHO, the global life expectancy is increasing year after year. However, deaths due to infectious disease are also increasing. A study conducted by the WHO reveals that more than 50,000 people die everyday from infectious diseases. One of the causes for the increase in infectious diseases is improper waste management. Blood, body fluids and body secretions which are constituents of bio-medical waste harbour most of the viruses, bacteria and parasites that cause infection. This passes via a number of human contacts, all of whom are potential ‘recipients’ of the infection. Human Immunodeficiency Virus (HIV) and hepatitis viruses spearhead an extensive list of infections and diseases documented to have spread through bio-medical waste. Tuberculosis, pneumonia, diarrhea diseases, tetanus, whooping cough etc., are other common diseases spread due to improper waste management. Occupational health hazards The health hazards due to improper waste management can affect The occupants in institutions and spread in the vicinity of the institutions People happened to be in contact with the institution like laundry workers, nurses, emergency medical personnel, and refuse workers. Risks of infections outside hospital for waste handlers, scavengers and (eventually) the general public Risks associated with hazardous chemicals, drugs, being handled by persons handling wastes at all levels Injuries from sharps and exposure to harmful chemical waste and radioactive waste also cause health hazards to employees.
 and hepatitis viruses spearhead an extensive list of infections and diseases documented to have spread through bio-medical waste. Tuberculosis, pneumonia, diarrhea diseases, tetanus, whooping cough etc., are other common diseases spread due to improper waste management. Occupational health hazards. The health hazards due to improper waste management can affect. The occupants in institutions and spread in the vicinity of the institutions. People happened to be in contact with the institution like laundry workers, nurses, emergency medical personnel, and refuse workers. Risks of infections outside hospital for waste handlers, scavengers and (eventually) the general public. Risks associated with hazardous chemicals, drugs, being handled by persons handling wastes at all levels Injuries from sharps and exposure to harmful chemical waste and radioactive waste also cause health hazards to employees.")
151
Hazards to the general public
The general public’s health can also be adversely affected by bio-medical waste. Improper practices such as dumping of bio-medical waste in municipal dustbins, open spaces, water bodies etc., leads to the spread of diseases. Emissions from incinerators and open burning also lead to exposure to harmful gases which can cause cancer and respiratory diseases. Exposure to radioactive waste in the waste stream can also cause serious health hazards. An often-ignored area is the increase of in-home healthcare activities. An increase in the number of diabetics who inject themselves with insulin, home nurses taking care of terminally ill patients etc., all generate bio-medical waste, which can cause health hazards.

153
Bio-medical waste & health hazards to animals and birds
Plastic waste can choke animals, which scavenge on open dumps. Injuries from sharps are common feature affecting animals. Harmful chemicals such as dioxins and furans can cause serious health hazards to animals and birds. Heavy metals can even affect the reproductive health of the animals Change in microbial ecology, spread of antibiotic resistance

155
Personnel safety devices
The use of protective gears should be made mandatory for all the personnel handling waste. Gloves: Heavy-duty rubber gloves should be used for waste handling by the waste retrievers. This should be bright yellow in colour. After handling the waste, the gloves should be washed twice. The gloves should be washed after every use with carbolic soap and a disinfectant. The size should fit the operator. Aprons, gowns, suits or other apparels: Apparel is worn to prevent contamination of clothing and protect skin. It could be made of cloth or impermeable material such as plastic. People working in incinerator chambers should have gowns or suits made of non-inflammable material. Masks: Various types of masks, goggles, and face shields are worn alone or in combination, to provide a protective barrier. It is mandatory for personnel working in the incinerator chamber to wear a mask covering both nose and mouth, preferably a gas mask with filters. Boots: Leg coverings, boots or shoe-covers provide greater protection to the skin when splashes or large quantities of infected waste have to be handled. The boots should be rubber-soled and anti-skid type. They should cover the leg up to the ankle.

157
Cleaning devices Brooms: The broom shall be a minimum of 1.2 m long, such that the worker need not stoop to sweep. The diameter of the broom should be convenient to handle. The brush of the broom shall be soft or hard depending on the type of flooring. Dustpans: The dustpans should be used to collect the dust from the sweeping operations. They may be either of plastic or enamelled metal. They should be free of ribs and should have smooth contours, to prevent dust from sticking to the surface. They should be washed with disinfectants and dried before every use. Mops: Mops with long handles must be used for swabbing the floor. They shall be of either the cloth or the rubber variety. The mop has to be replaced depending on the wear and tear. The mechanical-screw type of mop is convenient for squeezing out the water. Vacuum cleaners: Domestic vacuum cleaners or industrial vacuum cleaners can be used depending on the size of the rooms. Storage devices Dustbins: It is very important to assess the quantity of waste generated at each point. Dustbins should be of such capacity that they do not overflow between each cycle of waste collection. Dustbins should be cleaned after every cycle of clearance of waste with disinfectants. Dustbins can be lined with plastic bags, which are chlorine-free, and colour coded as per the law.

158
Handling devices Trolleys The use of trolleys will facilitate the removal of infectious waste at the source itself, instead of adding a new category of waste. Wheelbarrows: Wheelbarrows are used to transfer the waste from the point source to the collection centres. There are two types of wheelbarrow – covered and open. Wheelbarrows are made of steel and provided with two wheels and a handle. Care should be taken not to directly dump waste into it. Only packed waste (in plastic bags) should be carried. Care should also be taken not to allow liquid waste from spilling into the wheelbarrow, as it will corrode. These are ideal for transferring debris within the institution. Wheelbarrows also come in various sizes depending on the utility.
 should be carried. Care should also be taken not to allow liquid waste from spilling into the wheelbarrow, as it will corrode. These are ideal for transferring debris within the institution. Wheelbarrows also come in various sizes depending on the utility.")
159
Chutes: Chutes are vertical conduits provided for easy transportation of refuse vertically in case of institutions with more than two floors. Chutes should be fabricated from stainless steel. It should have a self-closing lid. These chutes should be fumigated everyday with formaldehyde vapours. The contaminated linen (contaminated with blood and or other body fluids) from each floor should be bundled in soiled linen or in plastic bags before ejecting into the chute. Alternately, elevators with mechanical winches or electrical winches can be provided to bring down waste containers from each floor. Chutes are necessary to avoid horizontal transport of waste thereby minimizing the routing of the waste within the premises and hence reducing the risk of secondary contamination.
 from each floor should be bundled in soiled linen or in plastic bags before ejecting into the chute. Alternately, elevators with mechanical winches or electrical winches can be provided to bring down waste containers from each floor. Chutes are necessary to avoid horizontal transport of waste thereby minimizing the routing of the waste within the premises and hence reducing the risk of secondary contamination.")
160
Use protective gear when handling waste Avoid needle stick injuries
Use protective gear when handling waste Avoid needle stick injuries Collect waste when the bin is 3/4 th full Avoid using common lift to move waste Avoid spillage Clean spills with disinfectant Use trolleys & do not drag waste bags

Similar presentations









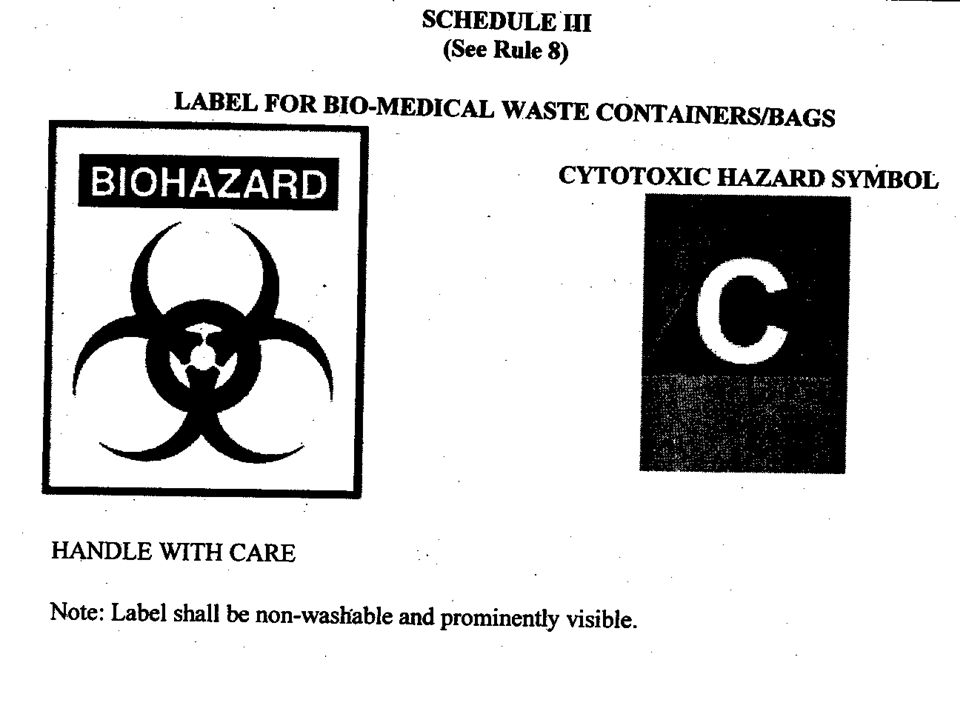
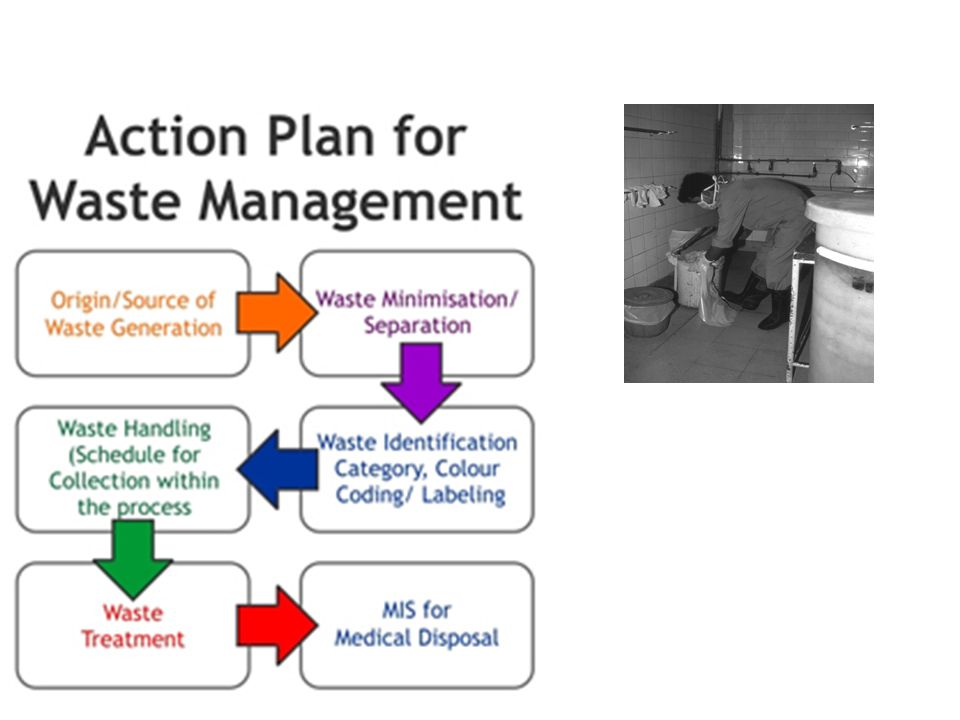

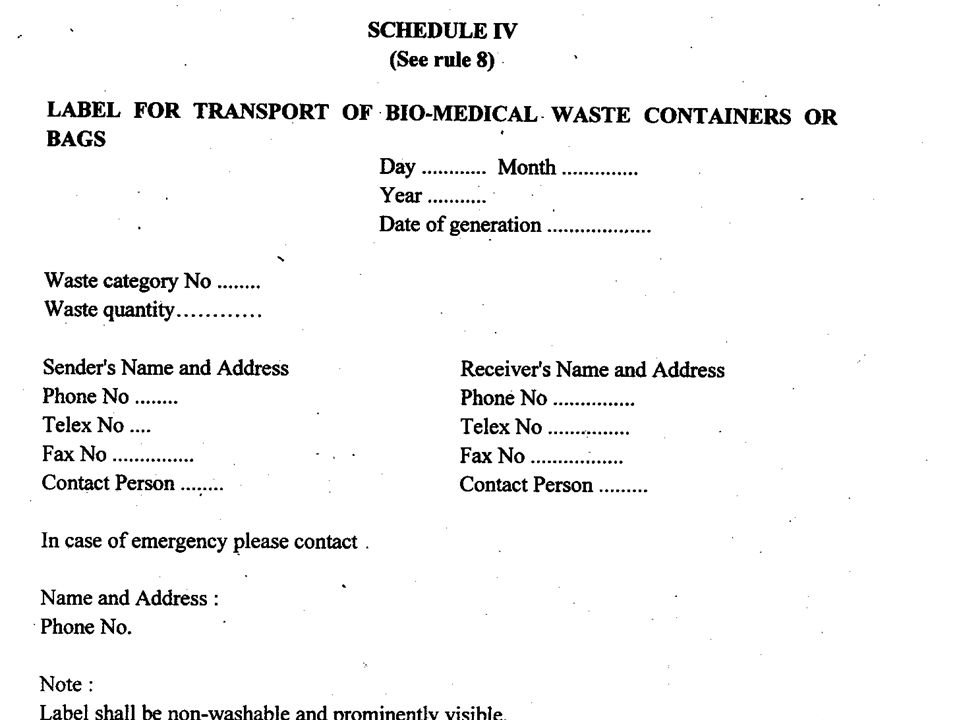

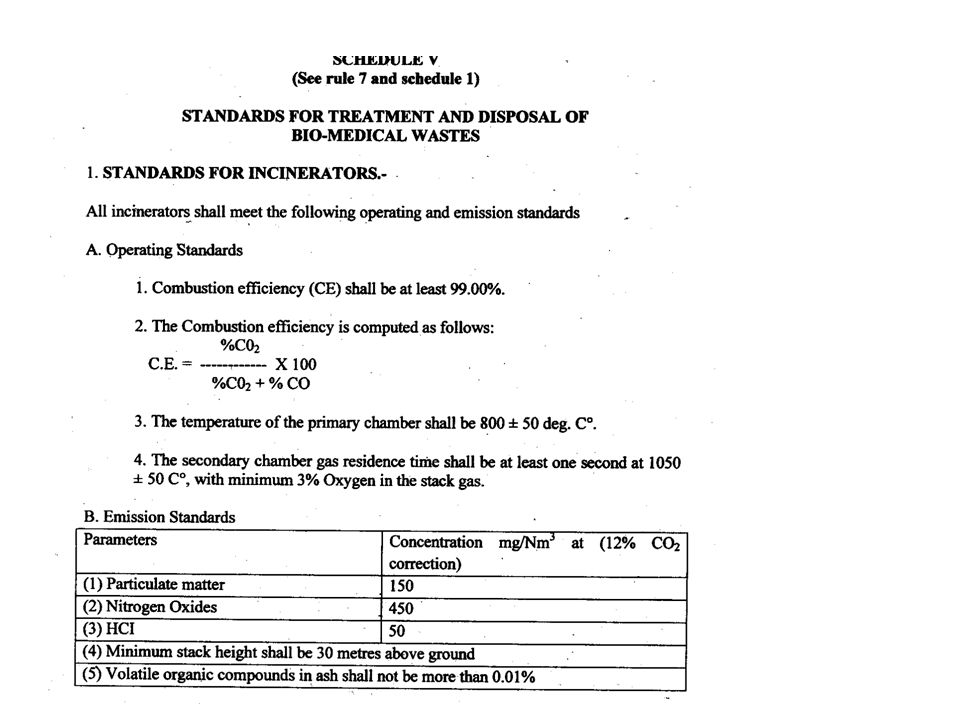
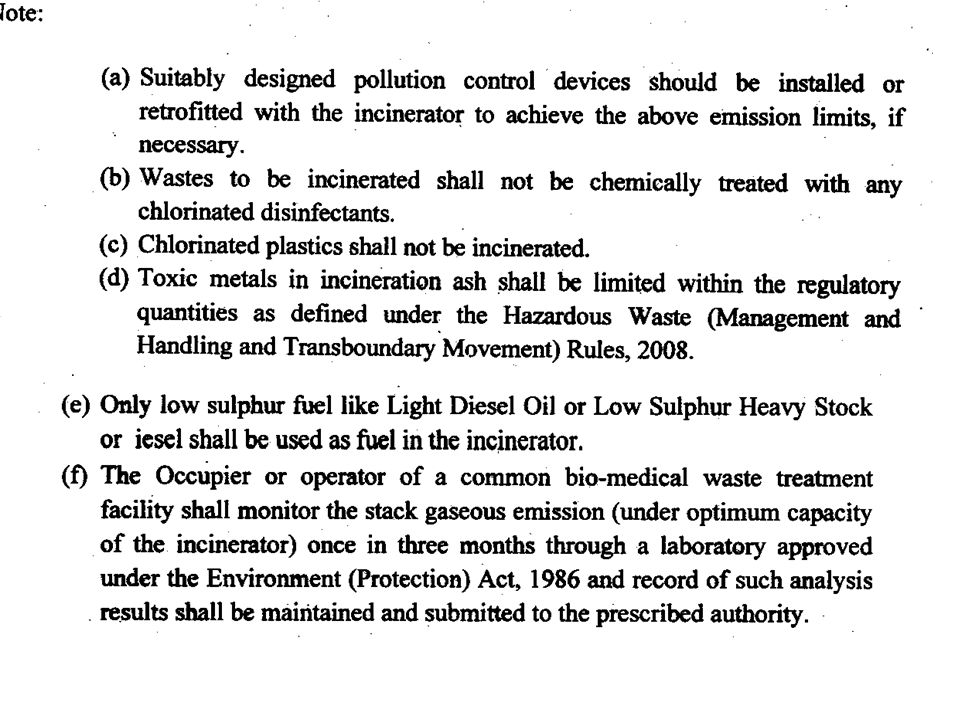


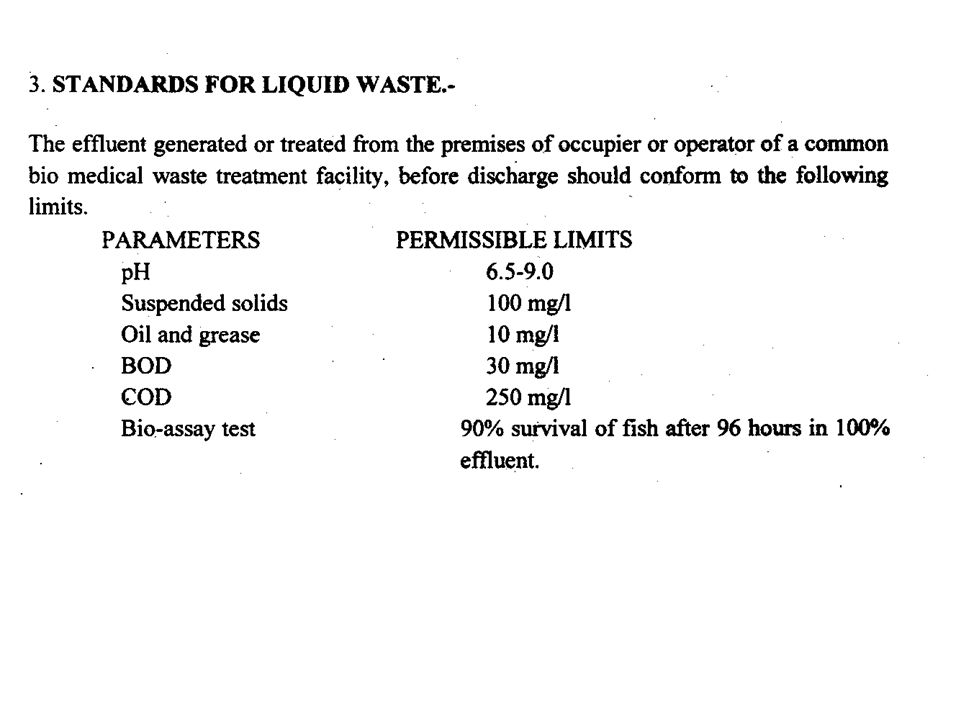
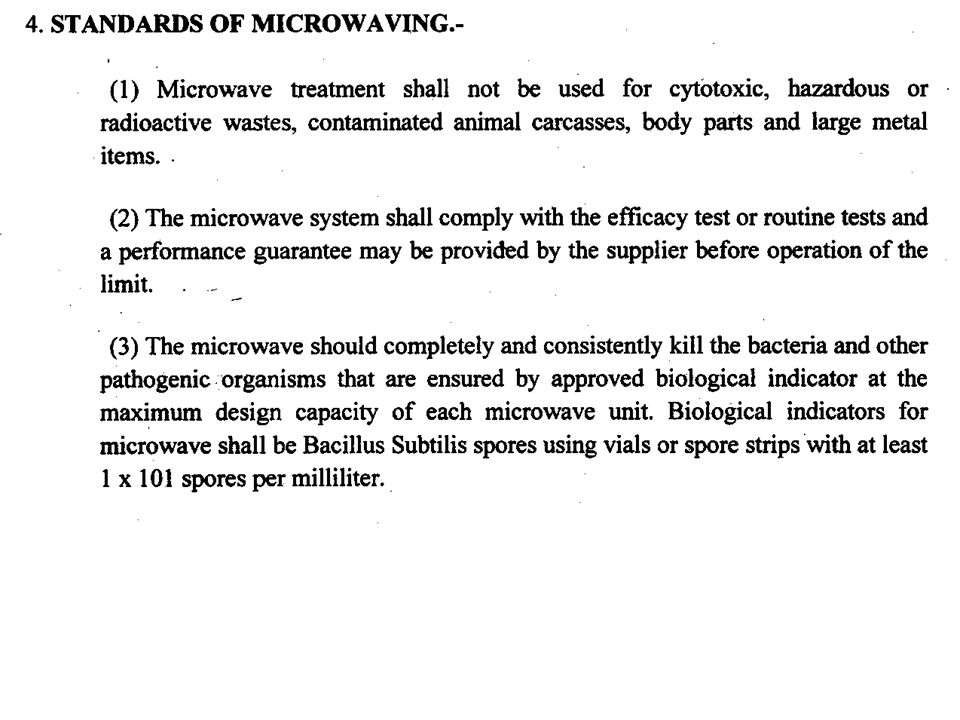












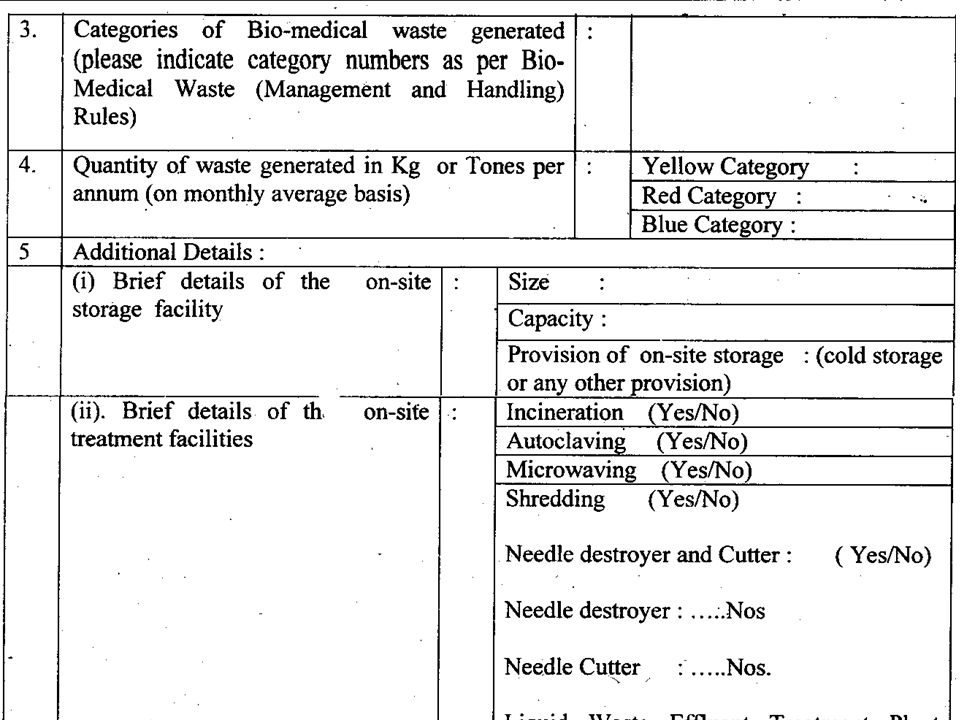

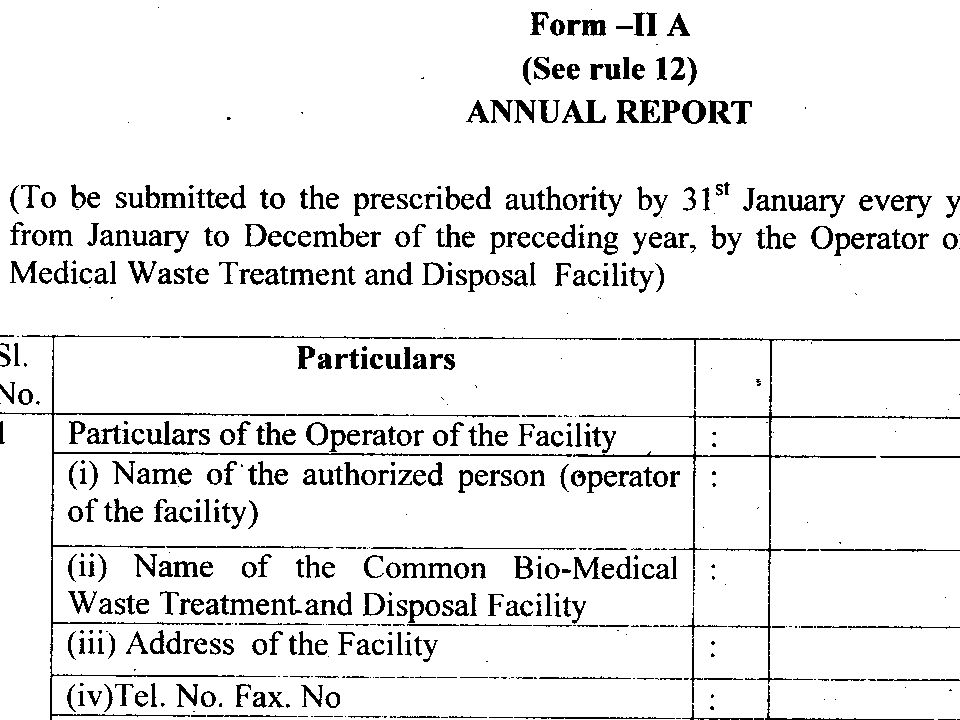












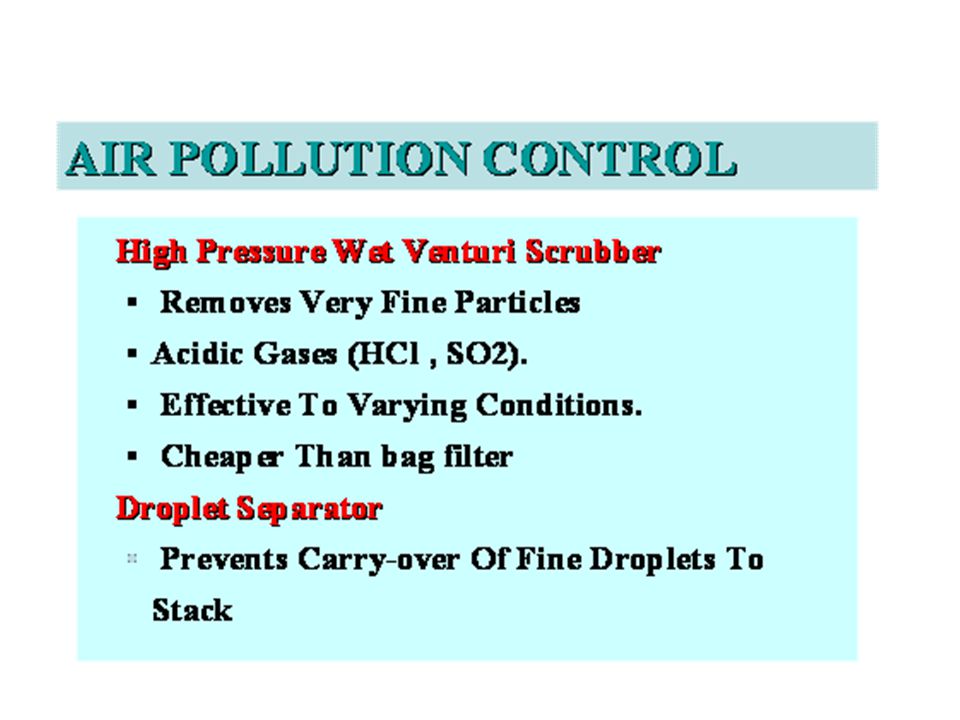




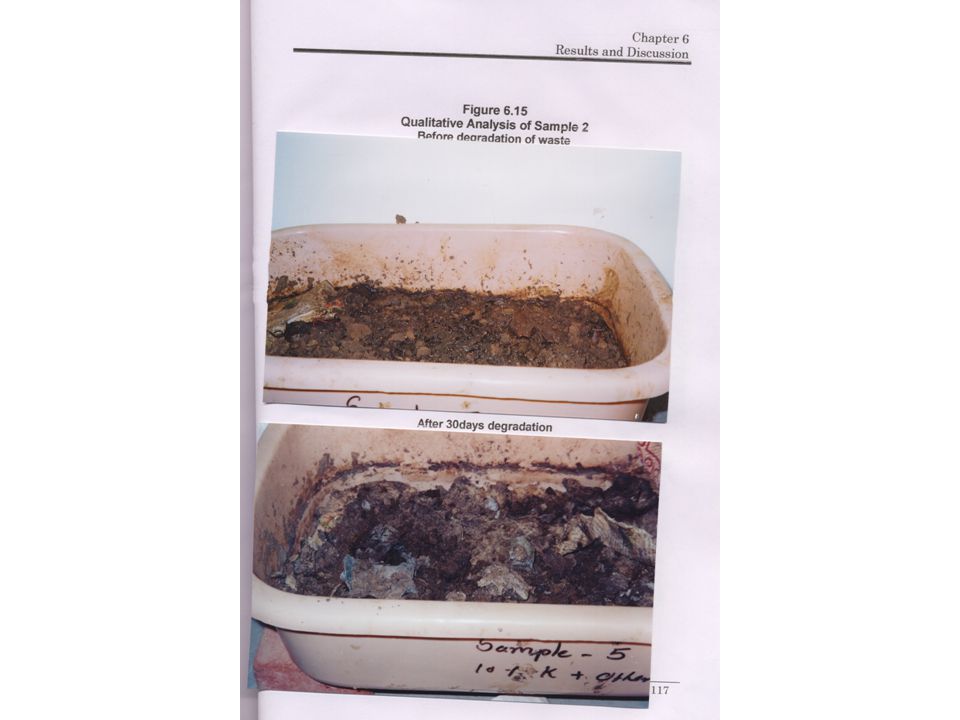

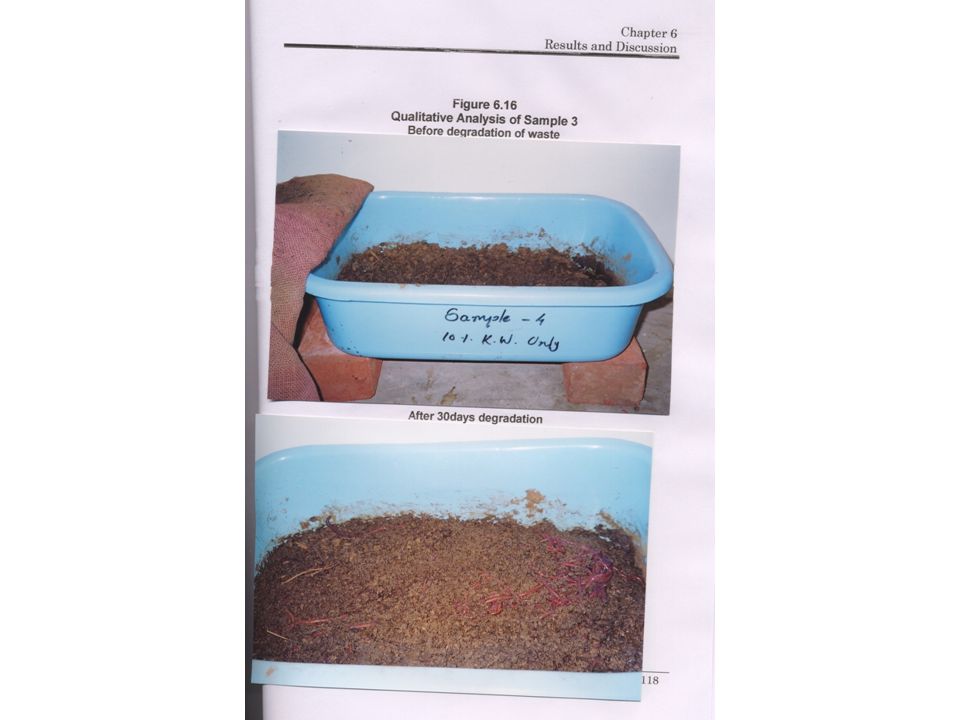








 Act, 1986 for the occupier of Health Care Facilities By Miss. Charu Gupta MSc. Environment.>")

 Alternative Disposal Methods Ohrid, Ana Petrovska.>")











>")
 OF 1970 George Mason University College of Nursing and Health Science Regulatory Requirements.>")



