Download presentation
Presentation is loading. Please wait.

1
Lipoproteins Metabolism and Clinical Implications Jack Blazyk

3
Why do we need lipoproteins?

4
How do we store our energy reserves? Carbohydrates Lipids Proteins 85% 15% <1%

5
Lipids are not very soluble in water

7
R - C - O Ester

8
Phospholipids Phosphatidylcholine = Lecithin

9
Lipids in the Blood Fatty Acids Bound to albumin Cholesterol, Triglycerides and Phospholipids Transported by lipoproteins Cholesterol can be free or esterified Triglycerides must be degraded extracellularly to be absorbed by cells <5% ~50%~15-20%~30% ~⅔~⅓

10
Anatomy of a Lipoprotein Fig. 25-1

11
Fig. 18.14 Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier

12
Apolipoproteins (or Apoproteins) They are the unique structural determinants of lipoproteins They serve as enzyme cofactors They are ligands for binding to lipoprotein receptors
 They are the unique structural determinants of lipoproteins They serve as enzyme cofactors They are ligands for binding to lipoprotein receptors")
13
Table 25-1. Composition of the Lipoproteins in Plasma of Humans LipoproteinSourceApolipoproteins ChylomicronsIntestine[A-I, A-II, A-IV], 1 B-48, C-II, E Chylomicron remnantsChylomicronsB-48, E VLDLLiver (intestine)B-100, C-II, E IDLVLDLB-100, E LDLVLDLB-100 HDLLiver, intestine, VLDL, chylomicrons A-I, A-II, A-IV, C-II, D, 2 E HDL 1 HDL 2 HDL 3 Preβ-HDL 3 A-I Albumin / free fatty acids Adipose tissue Abbreviations: HDL, high-density lipoproteins; IDL, intermediate-density lipoproteins; LDL, low-density lipoproteins; VLDL, very low density lipoproteins. 1 Secreted with chylomicrons but transfers to HDL. 2 Associated with HDL 2 and HDL 3 subfractions. 3 Part of a minor fraction known as very high density lipoproteins (VHDL).
B-100, C-II, E IDLVLDLB-100, E LDLVLDLB-100 HDLLiver, intestine, VLDL, chylomicrons A-I, A-II, A-IV, C-II, D, 2 E HDL 1 HDL 2 HDL 3 Preβ-HDL 3 A-I Albumin / free fatty acids Adipose tissue Abbreviations: HDL, high-density lipoproteins; IDL, intermediate-density lipoproteins; LDL, low-density lipoproteins; VLDL, very low density lipoproteins. 1 Secreted with chylomicrons but transfers to HDL. 2 Associated with HDL 2 and HDL 3 subfractions. 3 Part of a minor fraction known as very high density lipoproteins (VHDL)..")
14
Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.19 Fig. 18.13

15
How are dietary fats transported?

16
Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.16

17
Triglyceride-Degrading Enzymes LPL (Lipoprotein Lipase) extracellular enzyme on the walls of blood capillaries, anchored to the endothelium TG is hydrolyzed to free fatty acids plus glycerol Some of the released FFA enters circulation (bound to albumin) but most is transported into nearby tissue - mainly adipose, heart, and muscle (80%), while about 20% is transported to the liver
 extracellular enzyme on the walls of blood capillaries, anchored to the endothelium TG is hydrolyzed to free fatty acids plus glycerol Some of the released FFA enters circulation (bound to albumin) but most is transported into nearby tissue - mainly adipose, heart, and muscle (80%), while about 20% is transported to the liver")
18
Fig. 25-3 Metabolic fate of chylomicrons. (A, apolipoprotein A; B-48, apolipoprotein B-48;, apolipoprotein C; E, apolipoprotein E; HDL, high-density lipoprotein; TG, triacylglycerol; C, cholesterol and cholesteryl ester; P, phospholipid; HL, hepatic lipase; LRP, LDL receptor-related protein.) Only the predominant lipids are shown.
 Only the predominant lipids are shown..")
19
Triglyceride-Degrading Enzymes HL (Hepatic Lipase) HL is bound to the sinusoidal surface of liver cells Hydrolyzes TG to free fatty acids plus glycerol (just like LPL) Specific for chylomicron remnants and HDL
 HL is bound to the sinusoidal surface of liver cells Hydrolyzes TG to free fatty acids plus glycerol (just like LPL) Specific for chylomicron remnants and HDL")
20
Why do liver cells make VLDL? How is cholesterol delivered to tissues?

21
Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.17

22
Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.20

23
ACAT Intracellular Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.21

24
How does HDL transport cholesterol from the periphery to the liver?

25
Lippincott’s Illustrated Reviews Biochemistry - 5 th Ed. - 2011 R. Harvey & D. Ferrier Fig. 18.23 ?

26
Fig. 18.18 Lecithin:cholesterol Acyltransferase (LCAT) Lecithin Lyso-lecithin LCAT In HDL Phosphatidylcholine (PC) Lyso-phosphatidylcholine (Lyso-PC) Fig. 18.21 Lippincott’s Illustrated Reviews - Biochemistry - 5 th Ed. - 2011 - R. Harvey & D. Ferrier
 Lecithin Lyso-lecithin LCAT In HDL Phosphatidylcholine (PC) Lyso-phosphatidylcholine (Lyso-PC) Fig Lippincott’s Illustrated Reviews - Biochemistry - 5 th Ed R. Harvey & D. Ferrier.")
27
LCAT (Lecithin:Cholesterol Acyltransferase) Formation of cholesterol esters in HDL ACAT (Acyl-CoA:Cholesterol Acyltransferase) Formation of cholesterol esters inside cells
 Formation of cholesterol esters in HDL ACAT (Acyl-CoA:Cholesterol Acyltransferase) Formation of cholesterol esters inside cells")
28
Fig. 18.29 Lippincott’s Illustrated Reviews - Biochemistry - 5 th Ed. - 2011 - R. Harvey & D. Ferrier

29
Clinical Implications of Lipoproteins

30
Data from Framingham Heart Study

31
Activation of LDL Receptors LDLLDL Cholesterol LDL Receptors Liver Slide Source: Lipids Online Slide Library www.lipidsonline.org

32
LDLLDL Cholesterol LDL Receptors Liver Slide Source: Lipids Online Slide Library www.lipidsonline.org Familial Hypercholesterolemia x

33
Pre-2013 Lipid Guidelines

34
What drug therapies are available to improve blood lipid profiles?

35
Statins Acetyl-CoA LDLLDL HMG-CoA Reductase Cholesterol LDL Receptors Statin Liver Slide Source: Lipids Online Slide Library www.lipidsonline.org

36
Statins Rosuvastatin (Crestor - AstraZeneca) Fluvastatin (Lescol - Novartis) Atorvastatin (Lipitor - Pfizer) Pravastatin (Pravachol - BMS) Simvastatin (Zocor- Merck) Lovastatin (Mevacor - Merck) Nov 2011 Dec 2012 2006 2001 2016
 Fluvastatin (Lescol - Novartis) Atorvastatin (Lipitor - Pfizer) Pravastatin (Pravachol - BMS) Simvastatin (Zocor- Merck) Lovastatin (Mevacor - Merck) Nov 2011 Dec")
37
Adapted from British Journal of Cardiology 2004;11(2) Christopher J. Packard “Evolution of the HMG CoA Reductase Inhibitors (Statins) in Cardiovascular Medicine”
 in Cardiovascular Medicine .")
38
producing more than one effect; especially : having multiple phenotypic expressions Wish List for the Ideal Statin

39
Pleiotropic Effects of Statins (Cholesterol-independent?) Improved endothelial function Enhanced plaque stability Decreased oxidative stress, inflammation, and thrombogenic response Beneficial effects on immune system, CNS, and bone Effects mediated by inhibition of isoprenoids (lipid attachments for intracellular signaling molecules like Rho, Ras, and Rac)??
 Improved endothelial function Enhanced plaque stability Decreased oxidative stress, inflammation, and thrombogenic response Beneficial effects on immune system, CNS, and bone Effects mediated by inhibition of isoprenoids (lipid attachments for intracellular signaling molecules like Rho, Ras, and Rac)")
40
What are Statin Side Effects? Muscle pain and damage (rhabdomyolysis) Liver damage Digestive problems Rash or flushing Increased blood sugar or type 2 diabetes Neurological side effects [Click for more detail]
 Liver damage Digestive problems Rash or flushing Increased blood sugar or type 2 diabetes Neurological side effects [Click for more detail].")
41
Adapted from British Journal of Cardiology 2004;11(2) Christopher J. Packard “Evolution of the HMG CoA Reductase Inhibitors (Statins) in Cardiovascular Medicine”
 in Cardiovascular Medicine .")
44
Pharmaceutical Intervention Beyond Statins?

45
Vytorin Ezetimibe - Zetia (Schering-Plough) Simvastatin - Zocor (Merck) FDA approved Zetia in 2002 FDA approved Vytorin in 2004 Zocor patent expired in 2006
 Simvastatin - Zocor (Merck) FDA approved Zetia in 2002 FDA approved Vytorin in 2004 Zocor patent expired in 2006")
47
ENHANCE Trial Aftermath April 2006 - ENHANCE trial completed March 2008 - ENHANCE results released November 2009 - Merck acquires Schering-Plough February 2013 - Merck pays $688M settlemen t

49
Resurrection of Vytorin?

51
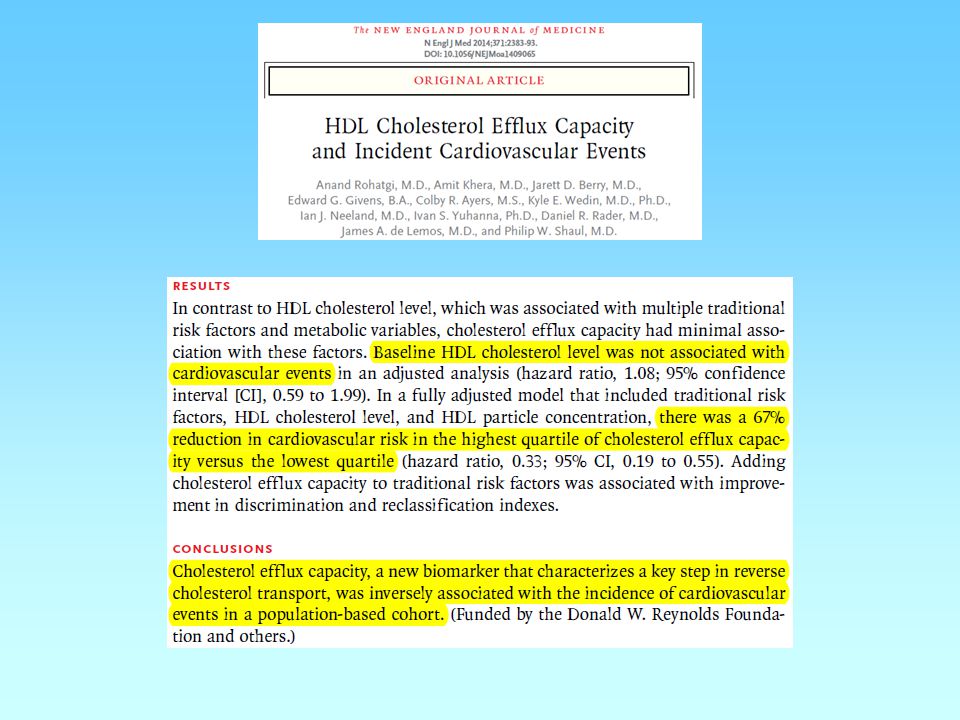
Correlation vs. Causation Does lower LDL-cholesterol always result in improved cardiac health? Primary vs. Secondary Endpoints

52
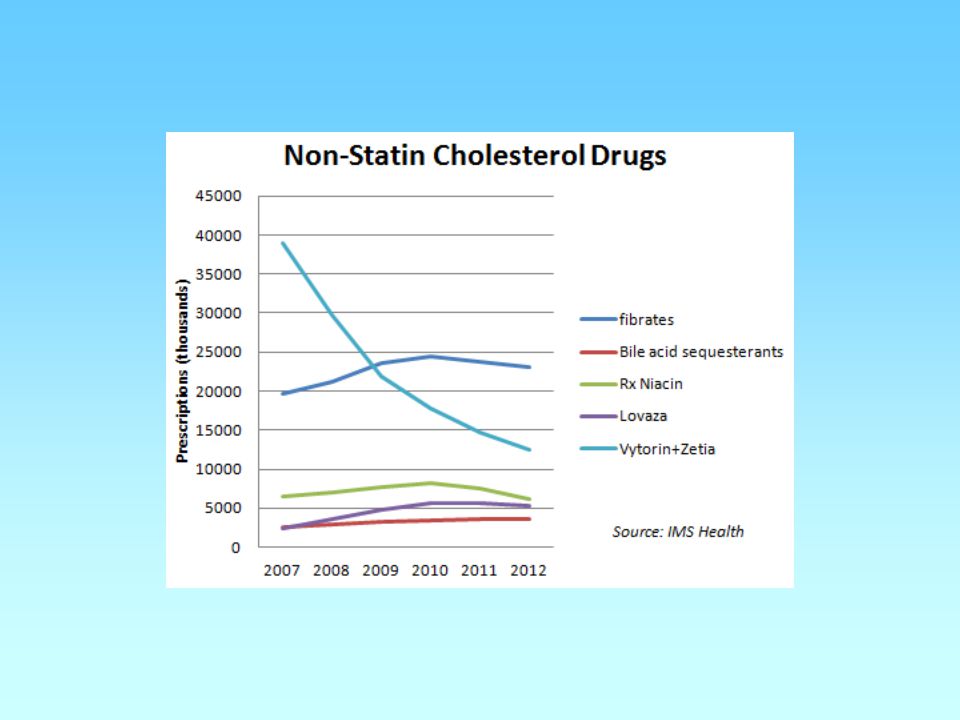
Other drugs to improve lipid profile and CV health?

53
Data from Framingham Heart Study

54
LCAT CE to VLDL TG to HDL

55
(Niaspan ®)
")
56
LCAT CE to VLDL TG to HDL

57
CETP Inhibitors torcetrapib (Pfizer) dalcetrapib (Roche) anacetrapib (Merck) evacetrapib (Lilly) ? ?

61
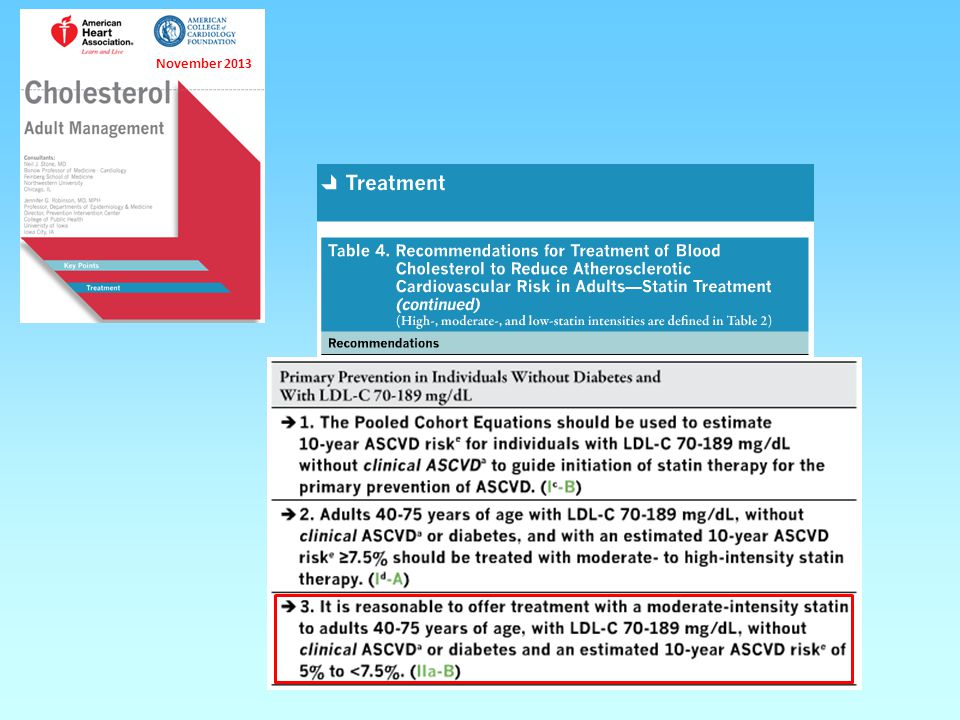
New 2013 AHA/ACC Guidelines Statins for the Masses? Obesity should be managed and treated like a disease More Americans could benefit from statins Cholesterol-lowering statin drugs could be prescribed to an estimated 33 million Americans without cardiovascular disease who have a 7.5 percent or higher risk for a heart attack or stroke within the next 10 years. This is a dramatic change from the 2002 federal cholesterol guideline, which recommended that people should only take a statin if their 10-year risk level exceeded 20 percent. The old guideline only considered a person’s risk for heart disease, leaving out the risk for stroke.

63
November 2013

67
Click here

72
Case Vignette Stephen, a 52-year-old white jogger with a BMI of 25, wants you to assess his cardiovascular risks. He had scheduled his visit after taking his father to another physician to discuss his father’s blindness, which is related to type 2 diabetes. Both his parents have hypertension that is controlled with medication; neither smokes. Stephen is here to discuss the results of blood tests that had been performed before the day of the visit.

73
Case Vignette “I’m an accountant, Doc, and I live by the numbers. I don’t want to be my father in 20 years,” he says. He tells you that he has recently increased his running regimen to 3 miles a day and that he smokes a half-pack a day during tax season, when he is under stress. “So what do the numbers say, and what’s this calculator thing?” he asks. His total cholesterol level is 180 mg/dL, HDL-cholesterol level is 35 mg/dL, triglyceride level is 150 mg/dL, and LDL-cholesterol level is 115 mg/dL. His BP is 130/85 mm Hg.

74
Case Vignette You think this is a great opportunity for shared decision making and explain that although his LDL-cholesterol level is not high, he has three risk factors for heart disease and stroke (he has a low HDL-cholesterol level, smokes, and is a man). You explain that the new AHA/ACC risk calculator estimates his 10-year risk of an event such as a heart attack or stroke at 10.9%, thereby requiring statin therapy. The new guidelines assess the risks of death from atherosclerotic heart disease, nonfatal heart attack, and stroke and do not call for laboratory testing of LDL- cholesterol once treatment with a statin is started.

75
Case Vignette You also explain that the new guidelines have shifted the approach to using statins and that they have generated controversy. You tell him that, in fact, statin treatment would not be recommended under the old guidelines, which assess the risk of coronary heart disease, even though the predicted risk would be higher. You have been using the Adult Treatment Panel (ATP) III calculator in your practice, and Stephen’s 10-year calculated risk according to that guideline is 13%. At that level of risk, with an LDL cholesterol level below 130 mg/dL, statin therapy would not be advised.
 III calculator in your practice, and Stephen’s 10-year calculated risk according to that guideline is 13%. At that level of risk, with an LDL cholesterol level below 130 mg/dL, statin therapy would not be advised..")
76
Case Vignette You tell him that you want more time to consider the new guidelines, and the two of you agree to meet again in 2 weeks. Stephen, with his hand on the doorknob, says, “Doc, I really want to know what you would do.” After he leaves, your nurse tells you that your practice has 500 patients who may need similar reassessments if you decide to use the new calculator. Which one of the following three approaches would you recommend for Stephen?

77
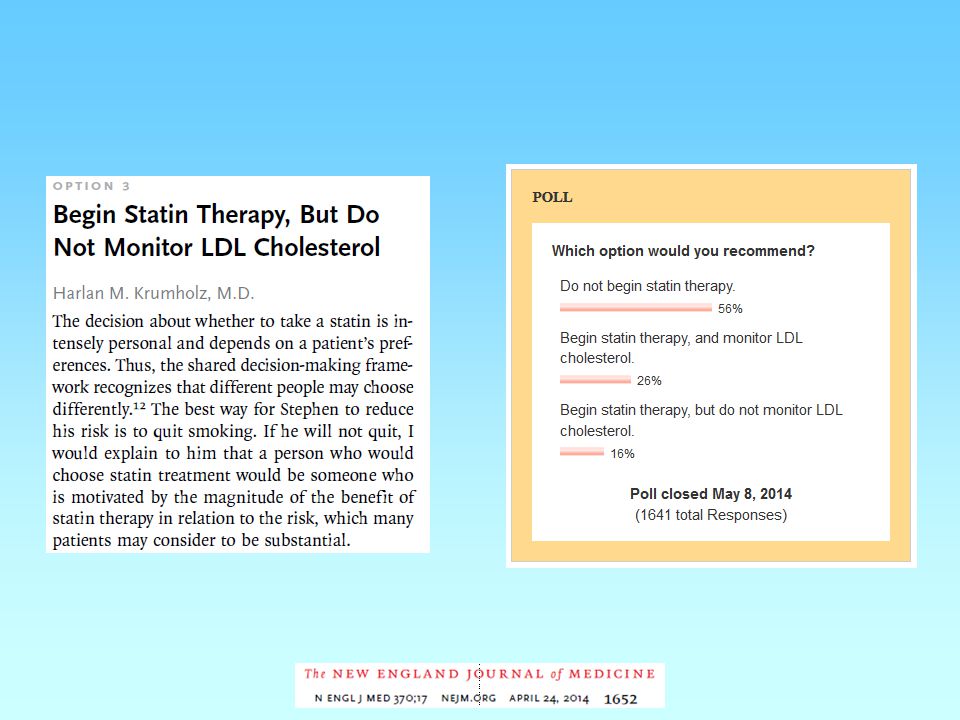
TREATMENT OPTIONS 1.Do not begin statin therapy. 2.Begin statin therapy, and monitor LDL-cholesterol. 3.Begin statin therapy, but do not monitor LDL-cholesterol.

82
It was supposed to be a moment of triumph. An august committee had for the first time relied only on the most rigorous scientific evidence to formulate guidelines to prevent heart attacks and strokes, which kill one out of every three Americans. The group had worked for five years, unpaid, to develop them. Then, at the annual meeting of the American Heart Association, it all went horribly awry. Many leading cardiologists now say the credibility of the guidelines, released Nov. 14, is shattered. And the troubled effort to devise them has raised broader questions about what kind of evidence should be used to direct medical practice, how changes should be introduced and even which guidelines to believe. “This was a catastrophic misunderstanding of how you go about this sort of huge change in public policy,” said Dr. Steven Nissen, a Cleveland Clinic cardiologist who is a past president of the American College of Cardiology. “There will be a large backlash.” [click here for full story]

83
http://www.cholesterolneversleeps.com/pcsk9 On the Horizon PCSK9 [Proprotein convertase subtilisin/kexin type 9] PCSK9 is involved in regulation of LDL-receptor recycling in hepatocytes Monoclonal antibodies to PCSK9 inhibit its activity and promote more LDL-receptor recycling, resulting in greater LDL uptake by liver cells and lower LDL-cholesterol in the blood For a short (4-min) video demonstrating the mechanism, click the link below:
![On the Horizon PCSK9 [Proprotein convertase subtilisin/kexin type 9] PCSK9 is involved in regulation of LDL-receptor recycling in hepatocytes Monoclonal antibodies to PCSK9 inhibit its activity and promote more LDL-receptor recycling, resulting in greater LDL uptake by liver cells and lower LDL-cholesterol in the blood For a short (4-min) video demonstrating the mechanism, click the link below:](http://images.slideplayer.com/12/3474411/slides/slide_83.jpg "On the Horizon PCSK9 [Proprotein convertase subtilisin/kexin type 9] PCSK9 is involved in regulation of LDL-receptor recycling in hepatocytes Monoclonal antibodies to PCSK9 inhibit its activity and promote more LDL-receptor recycling, resulting in greater LDL uptake by liver cells and lower LDL-cholesterol in the blood For a short (4-min) video demonstrating the mechanism, click the link below:")
84
PCSK9 [Proprotein convertase subtilisin/kexin type 9]
![PCSK9 [Proprotein convertase subtilisin/kexin type 9]](http://images.slideplayer.com/12/3474411/slides/slide_84.jpg "PCSK9 [Proprotein convertase subtilisin/kexin type 9]")
Similar presentations


















 E: Which monomer are enzymes made from? D: What is activation energy? C: Describe the effect of enzymes.>")


















