Download presentation
Presentation is loading. Please wait.

1
Potassium Dr Anjali Acharya Department of Medicine Division of Nephrology Jacobi Medical Center Albert Einstein College of Medicine

5
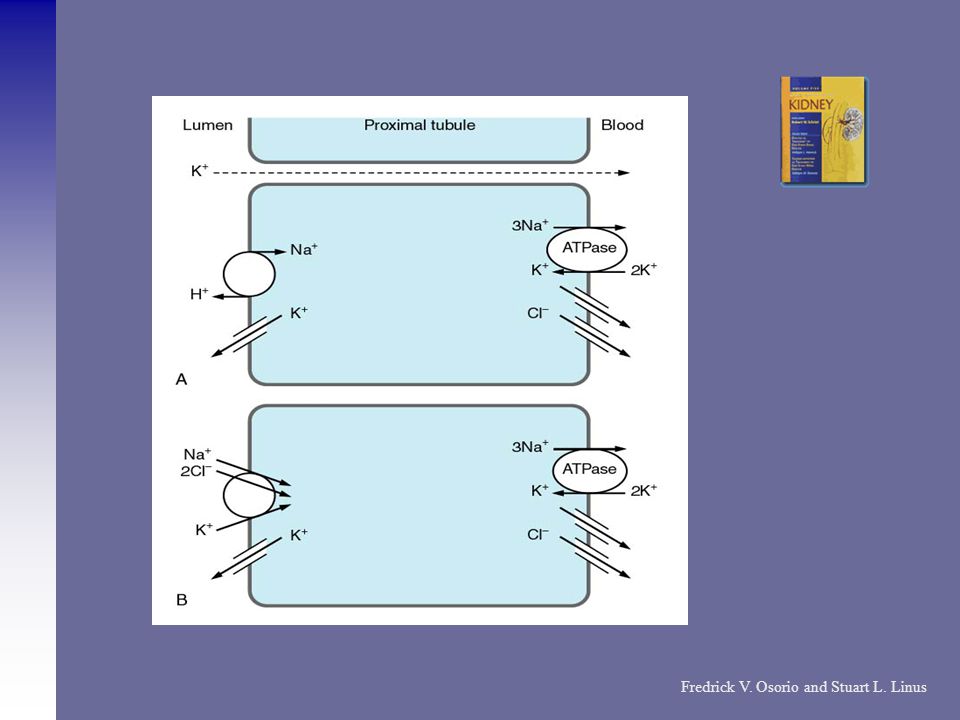
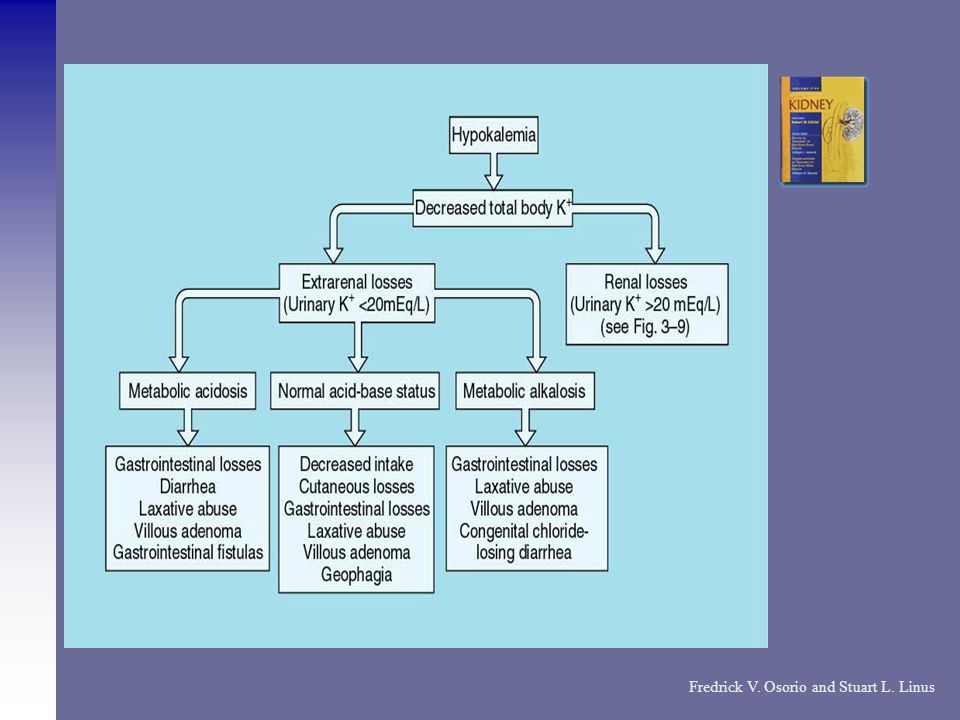
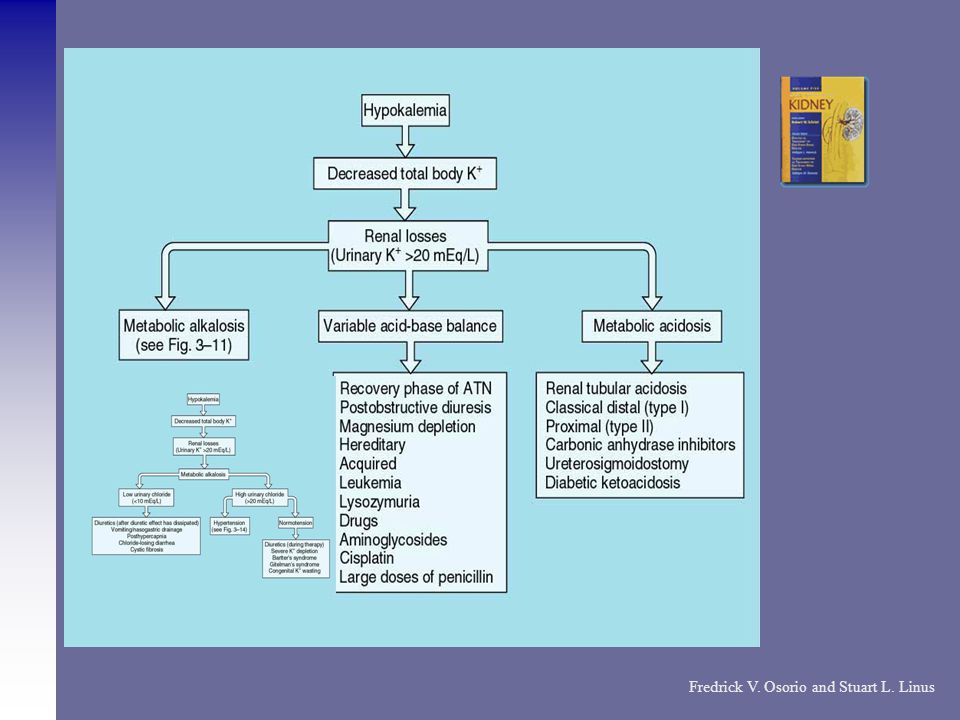
Fredrick V. Osorio and Stuart L. Linus

32
Calcium Metabolism

33
Passive and paracellular Ca2 transport takes place across tight junctions and is driven by the electrochemical gradient for Ca2 (blue arrow). Active and transcellular Ca2 transport is a three-step process. Ca2 enters through (hetero)tetrameric epithelial Ca2 channels, TRPV5 andTRPV6, Ca2 bound to calbindin diffuses to the basolateral membrane. At the basolateral membrane, Ca2 is extruded via an ATP-dependent Ca2-ATPase (PMCA1b) and a Na/Ca2 exchanger (NCX1). The active form of vitaminD stimulates the individual steps of transcellular Ca2 transport by increasing the expression of the luminal Ca2 channels, calbindins, and the extrusion systems.
tetrameric epithelial Ca2 channels, TRPV5 andTRPV6, Ca2 bound to calbindin diffuses to the basolateral membrane. At the basolateral membrane, Ca2 is extruded via an ATP-dependent Ca2-ATPase (PMCA1b) and a Na/Ca2 exchanger (NCX1). The active form of vitaminD stimulates the individual steps of transcellular Ca2 transport by increasing the expression of the luminal Ca2 channels, calbindins, and the extrusion systems..")
34
Ion transport in loop of Henle

35
TRPV5 knockout mice display profound renal Ca2 wasting because of impaired active reabsorption in DCT of the distal nephron TRPV5 expression in the kidney is mainly regulated by both PTH and 1,25(OH)2D. Parathyroidectomy in rats is accompanied by diminished TRPV5, calbindin- D28K, and Na/Ca2 exchanger protein abundance. Nijmegen group clearly established the channel TRPV5 as the rate-limiting step in active Ca2 reabsorption They elucidated several interesting extracellular factors that may regulate the crucial TRPV5 channel and play a role in clinical disorders of calcium excretion

36
The anti-aging hormone Klotho regulates and stimulates TRPV5 activity and calcium transport via a novel mechanism By modifying its glycosylation status? Also, the extracellular pH seems to act as a dynamic switch controlling cell surface expression of TRPV5.

37
The extracellular calcium-sensing receptor (CaSR)-a member of the G protein-coupled receptor Regulates the secretion of parathyroid hormone (PTH) and the reabsorption of tubular fluid calcium. Activation of the CaR by increased extracellular Ca2+ inhibits parathyroid hormone (PTH) secretion, stimulates calcitonin secretion, and promotes urinary Ca2+ excretion Structural abnormalities of CaSR are responsible for different hypo- or hypercalcemic disorders: Inactivating mutations cause: familial hypocalciuric hypercalcaemia (FHH) and neonatal severe primary hyperparathyroidism (NSPHT), and Activating mutations cause autosomal dominant hypocalcaemia (ADH)
 secretion, stimulates calcitonin secretion, and promotes urinary Ca2+ excretion Structural abnormalities of CaSR are responsible for different hypo- or hypercalcemic disorders: Inactivating mutations cause: familial hypocalciuric hypercalcaemia (FHH) and neonatal severe primary hyperparathyroidism (NSPHT), and Activating mutations cause autosomal dominant hypocalcaemia (ADH).")
38
Calcium-Sensing Receptor The human CaSR gene is located on chromosome 3q13.3–21 The amino acid sequence of the hCaR A 1078 amino-acid polypeptide Activates multiple G proteins including Gq/11 and Gi, and thereby activates different signal transduction pathways, depending on the cell type Activation of the CaR by increased extracellular Ca2+ leads to inhibition of PTH secretion All GPCRs share the signature seven transmembrane-spanning (7TM) domain Agonist-induced GPCR activation presumably involves conformational changes of the membrane-spanning helices, altering the disposition of intracellular loops and Cterminus,and thereby promoting activation of G proteins.
 domain Agonist-induced GPCR activation presumably involves conformational changes of the membrane-spanning helices, altering the disposition of intracellular loops and Cterminus,and thereby promoting activation of G proteins.")
39
Etiology Of Hypocalcemia Hyperphosphatemia Intravascular binding Intravascular binding Hypercalciuria Decreased PTH secretion Hypovitaminosis D -poor intake or malabsorption, decreased 25- hydroxylation of vitamin D to form calcidiol in the liver, increased metabolism to inactive metabolites, decreased 1-hydroxylation of calcidiol to calcitriol in the kidney, and decreased calcitriol action. calcitriol Magnesium depletion – Mech-PTH resistance, decreased PTH secretion Causes-Malabsorption, chronic alcoholism, cisplatin, parenteral fluid administration, diuretic therapy, aminoglycosides cisplatin Sepsis or severe illness Sepsis or severe illness Chemotherapy Fluoride poisoning Bisphosphonates PSEUDOHYPOCALCEMIA

40
Treatment of Hypocalcemia Symptomatic or may be asymptomatic Symptomatic or may be asymptomatic Severity and the underlying cause The symptoms: paresthesias, tetany, hypotension, seizures, and they may have Chvostek's or Trousseau's signs, bradycardia, impaired cardiac contractility, and prolongation of the QT interval.

41
Treatment of Hypocalcemia Intravenous calcium, (1 to 2 grams of calcium gluconate) in 10 to 20 minutes The calcium should not be given more rapidly, because of the risk of serious cardiac dysfunction, including systolic arrest calcium gluconate calcium gluconate followed by a slow infusion of calcium Hypomagnesemia
 in 10 to 20 minutes The calcium should not be given more rapidly, because of the risk of serious cardiac dysfunction, including systolic arrest calcium gluconate calcium gluconate followed by a slow infusion of calcium Hypomagnesemia")
42
Hypercalcemia Etiology Hyperparathyroidism: Primary, Sec and tertiary Malignancy Malignancy Thyrotoxicosis Thyrotoxicosis Immobilization Hypervitaminosis A Increased calcium intake Increased calcium intake Chronic kidney disease Chronic kidney disease Milk alkali syndrome - hypercalcemia, metabolic alkalosis, and renal insufficiency Hypervitaminosis D - by increasing calcium absorption and bone resorption – exogenous or increased endogenous production of 1,25D Thiazide diuretics Thiazide diuretics Rhabdomyolysis and acute renal failure Rhabdomyolysis and acute renal failure Familial hypocalciuric hypercalcemia -loss of fn mutations in CaSR

43
Clinical manifestations of hypercalcemia NEUROPSYCHIATRIC DISTURBANCES - anxiety, depression, and cognitive dysfunction, lethargy, confusion, stupor, and coma GASTROINTESTINAL ABNORMALITIES - constipation, anorexia, and nausea, pancreatitis and peptic ulcer disease RENAL DYSFUNCTION- polyuria, nephrolithiasis, and acute and chronic renal insufficiency CARDIOVASCULAR DISEASE - shortens the myocardial action potential, can cause supraventricular or ventricular arrhythmias MUSCULOSKELETAL SYMPTOMS MUSCULOSKELETAL SYMPTOMS

44
Treatment of hypercalcemia Acute or chronic Severity- serum calcium concentration >14 mg/dL Isotonic saline-initial rate of 200 to 300 mL/h that is then adjusted to maintain the urine output at 100 to 150 mL/h. Loop diuretic BISPHOSPHONATES- analogs of inorganic pyrophosphate- inhibit calcium release by interfering with osteoclast-mediated bone resorption CALCITONIN GLUCOCORTICOIDS GLUCOCORTICOIDS Calcimimetics Dialysis Dialysis

45
Phosphate Metabolism

46
Electrogenic NaPi-IIa couples 3 Na+ ions to uphill movement of one divalent Pi per transport cycle. One net charge is translocated.

47
Phosphate The serum phosphate concentration is primarily a function of the rate of renal phosphate reabsorption Molecular components of renal phosphate reabsorption The Na/Pi co-transporter family mainly consists of three different types, but only two are expressed in the kidney: Type IIa (Na/Pi-2a) and type IIc (Na/Pi-2c), which are almost exclusively present in the brush border membrane of the renal proximal tubular epithelial cells Type III Na/Pi transporters are found in the basolateral membrane of the renal tubules, where they are thought to serve a function of regulating intracellular phosphate levels Factors affect phosphate transport by influencing the Na/Pi co-transporter system; (PTH) inhibits the Na/Pi co-transporter system-by endocytic retrieval of Na/Pi-2a and Na/Pi-2c proteins Fibroblast growth factor 23 (FGF-23): “phosphatonin”-stimulating urinary phosphate excretion by inhibiting the Na/Pi co-transporter system Dietary phosphate KLOTHO-(named for the Greek Fate purported to spin the thread of life),- Klotho is essential for endogenous FGF-23 Function. Klotho seems to act by converting a protein precursor of the receptor for FGF-23 into the functional receptor.

48
HEREDITARY HYPOPHOSPHATEMIC RICKETS WITH HYPERCALCIURIA (HHRH) HHRH is a primary disorder of renal Pi reabsorption Renal type IIa Na/Pi cotransporter (Npt2) is an important determinant of Pi homeostasis Growth retardation, bone deformities, renal Pi wasting, hypophosphatemia, increased serum levels of 1,25(OH)2D and associated hypercalciuria
 HHRH is a primary disorder of renal Pi reabsorption Renal type IIa Na/Pi cotransporter (Npt2) is an important determinant of Pi homeostasis Growth retardation, bone deformities, renal Pi wasting, hypophosphatemia, increased serum levels of 1,25(OH)2D and associated hypercalciuria")
49
Electrogenic NaPi-IIa couples 3 Na+ ions to uphill movement of one divalent Pi per transport cycle. One net charge is translocated. Electroneutral NaPi-IIc couples 2 Na+ ions to the uphill transport of one divalent Pi. No net charge transfer occurs Driven by ATP hydrolysis, the NaKATPase maintains intracellular electronegativity by removing accumulated Na+ ions in exchange for K+ ions. Basolateral exit of Pi is via an unknown pathway. Pi then diffuses into blood. Blood Na+Pi − HPO4 2 HPO4 +

Similar presentations






























![Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.](/12/3581741/big_thumb.jpg "Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.>")

 and, >")

![Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.](/15/4762424/big_thumb.jpg "Clinical aspects of common mineral disorders. hypocalcemia Normal [Ca2+] total = 8.5-10.5 mg/dl (2.12-2.62 mmol/L) Normal [Ca2+] ion = 4.65-5.25 mg/dL.>")





