Download presentation
Presentation is loading. Please wait.

1
Calcium metabolism: Physiology, biochemistry & pathology
PBL 5 Calcium metabolism: Physiology, biochemistry & pathology

2
Effects of hypocalcaemia Contraction
Biological role of Ca2+ protein stability second messenger synaptic transmission of nerve impulses blood clotting muscle contraction RDI: 20-25mmol ( mg) Effects of hypocalcaemia Contraction lethal tetany at [Ca2+ ] ≤ 4mg/100ml Reduction spontaneous nerve discharge tetanic muscle Effects of hypercalcaemia If normal extracellular fluid [Ca2+] increases up to 12 mg/100ml depressed neuronal activity constipation lack of appetite disseminated calcium phosphate precipitation at [Ca2+ ] ≥ 17mg/100ml
 Effects of hypocalcaemia. Contraction. lethal tetany at [Ca2+ ] ≤ 4mg/100ml Reduction. spontaneous nerve discharge. tetanic muscle. Effects of hypercalcaemia. If normal extracellular fluid [Ca2+] increases up to 12 mg/100ml. depressed neuronal activity. constipation. lack of appetite. disseminated calcium phosphate precipitation at [Ca2+ ] ≥ 17mg/100ml.")
3
Role of Ca2+ in cell regulation
Cytosolic Ca2+ concentration (0.1 – 0.01μmol/L) is kept much lower than extracellular levels (~1.3mmol/L) This is due to Ca2+ being continuously pumped from cytosol into intracellular Ca2+ stores such as the endoplasmic reticulum and sarcoplasmic reticulum, vesicles and mitochondria, or it is transported out of the cell Ca2+ is involved in: myocyte contraction exocytosis of neurotransmitters in presynaptic nerve endings endocrine and exocrine Hormone secretion excitation of sensory cells closure of gap junctions calmodulin can bind up to 4 Ca2+ ions when the [Ca2+]i rises. Ca2+-calmodulin complexes activate a number of different enzymes, including myosin light chain kinase (MLCK), which is involved in smooth muscle contraction
 is kept much lower than extracellular levels (~1.3mmol/L) This is due to Ca2+ being continuously pumped from cytosol into intracellular Ca2+ stores such as the endoplasmic reticulum and sarcoplasmic reticulum, vesicles and mitochondria, or it is transported out of the cell. Ca2+ is involved in: myocyte contraction. exocytosis of neurotransmitters. in presynaptic nerve endings. endocrine and exocrine. Hormone secretion. excitation of sensory cells. closure of gap junctions. calmodulin can bind up to 4 Ca2+ ions when the [Ca2+]i rises. Ca2+-calmodulin complexes activate a number of different enzymes, including myosin light chain kinase (MLCK), which is involved in smooth muscle contraction.")
4
Calcium storage in the body
In Blood: Normally found in concentrations of approximately 2.4 mmol/dL Ca2+ is normally found in concentrations of 1.2mmol/L 40% is combined with plasma proteins (won’t diffuse through capillary membrane) 10% is combined with other plasma and interstitial substances (will diffuse through capillary membrane) 50% is in ionised form (will diffuse through capillary membrane) In Bone: Exists in crystalline salts Mostly of hydroxyapatite (Ca10(PO4)6(OH)2) Relative ratio of calcium to phosphorous varies according to nutritional status Normal extracellular fluid concentrations of calcium and phosphorous are greatly in excess of that required to cause precipitation of hydroxyapatite This is inhibited by various inhibitors throughout the body Precipitation of calcium salts occurs along the collagen fibres of bone due to neutralisation of the inhibitors (possibly due to secretion of pyrophosphate by the osteoblasts) Rapidly mobilizable calcium is found in the form of CaHPO4 and other amorphous calcium salts
 10% is combined with other plasma and interstitial substances (will diffuse through capillary membrane) 50% is in ionised form (will diffuse through capillary membrane) In Bone: Exists in crystalline salts. Mostly of hydroxyapatite (Ca10(PO4)6(OH)2) Relative ratio of calcium to phosphorous varies according to nutritional status. Normal extracellular fluid concentrations of calcium and phosphorous are greatly in excess of that required to cause precipitation of hydroxyapatite. This is inhibited by various inhibitors throughout the body. Precipitation of calcium salts occurs along the collagen fibres of bone due to neutralisation of the inhibitors (possibly due to secretion of pyrophosphate by the osteoblasts) Rapidly mobilizable calcium is found in the form of CaHPO4 and other amorphous calcium salts.")
5
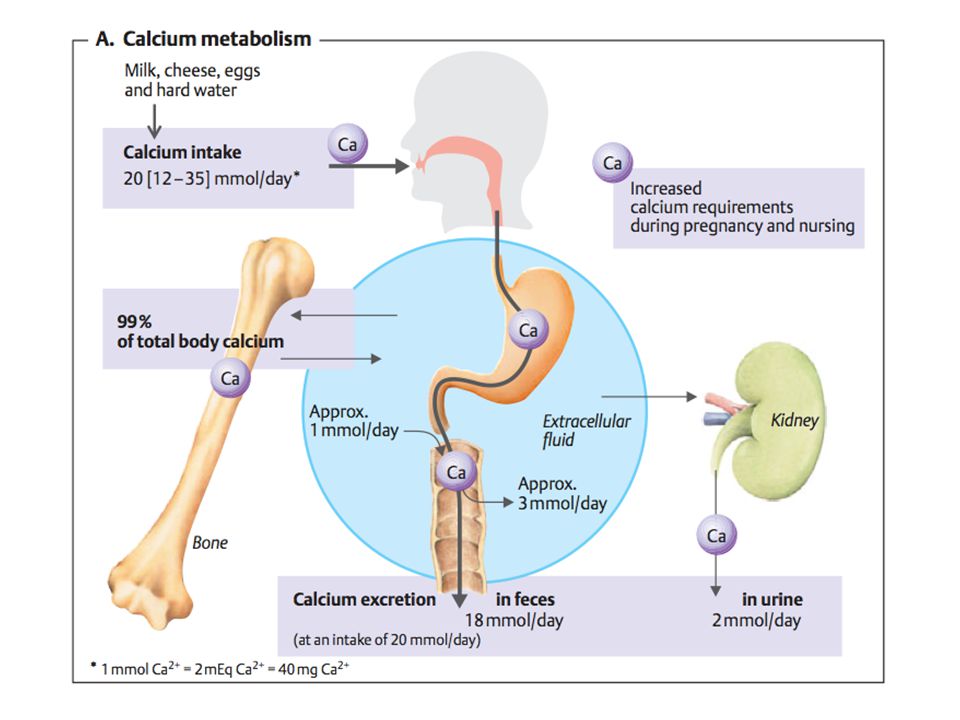
Excretion In Faeces: In Kidneys:
9/10 of daily intake of Ca2+ is excreted in the faeces In Kidneys: 90% of Ca2+ in glomerular filtrate is reabsorbed in the proximal tubules, the loops of Henle and the early distal tubules Selective reabsorption occurs in the late distal tubules and early collecting ducts If Ca2+ concentration in blood is low then almost all can be reabsorbed

6
Control of circulating calcium
Calcium levels are under tight control by parathyroid hormone (PTH) and the vitamin D axis. Sources for circulating calcium are: Absorption of dietary calcium by GIT Reduction of calcium excretion by the kidneys Release of stored calcium from bones
 and the vitamin D axis. Sources for circulating calcium are: Absorption of dietary calcium by GIT. Reduction of calcium excretion by the kidneys. Release of stored calcium from bones.")
7
Regulation of plasma levels
The calcium sensing receptor (CaSR) is expressed in: parathyroid, thyroid, kidney, gastrointestinal tract, brain Regulation of calcium is primarily done by parathyroid hormone (PTH) Production of parathyroid hormone is inhibited by high Ca2+ levels Effects of PTH: Reabsorption of Ca2+ in kidney (at distal tubules) The action of 1-hydroxylase (which converts Vitamin D to 1,25-Dihydroxycholecalciferol) Resorption of bone number of Ca2+ channels in osteoblasts Activity of osteoclasts Phosphate secretion Thus preventing phosphate and calcium from recrystallising bone By actions of 1,25-Dihydroxycholecalciferol Plasma Ca2+ inhibits the conversion of 25-Hydroxycholecalciferol to 1,25-Dihydroxycholecalciferol Lack of 1,25-Dihydroxycholecalciferol absorption of Ca2+ from bones Lack of 1,25-Dihydoxycholecalciferol absorption of Ca2+ from renal tubules By effects of Calcitonin Production of calcitonin is stimulated by high Ca2+ levels Reabsorption of calcium in the kidneys Resorption of bone High Ca2+ levels are sensed by membrane receptors IP3 released intracellularly triggers an increase in the [Ca2+]i of parafollicular C cells of the thyroid gland. This induces the exocytosis of calcitonin,
 is expressed in: parathyroid, thyroid, kidney, gastrointestinal tract, brain. Regulation of calcium is primarily done by parathyroid hormone (PTH) Production of parathyroid hormone is inhibited by high Ca2+ levels. Effects of PTH: Reabsorption of Ca2+ in kidney (at distal tubules) The action of 1-hydroxylase (which converts Vitamin D to 1,25-Dihydroxycholecalciferol) Resorption of bone. number of Ca2+ channels in osteoblasts. Activity of osteoclasts. Phosphate secretion. Thus preventing phosphate and calcium from recrystallising bone. By actions of 1,25-Dihydroxycholecalciferol. Plasma Ca2+ inhibits the conversion of 25-Hydroxycholecalciferol to 1,25-Dihydroxycholecalciferol. Lack of 1,25-Dihydroxycholecalciferol absorption of Ca2+ from bones. Lack of 1,25-Dihydoxycholecalciferol absorption of Ca2+ from renal tubules. By effects of Calcitonin. Production of calcitonin is stimulated by high Ca2+ levels. Reabsorption of calcium in the kidneys. Resorption of bone. High Ca2+ levels are sensed by membrane receptors IP3 released intracellularly triggers an increase in the [Ca2+]i of parafollicular C cells of the thyroid gland. This induces the exocytosis of calcitonin,")
11
Disturbances in Calcium homeostasis
Causes of hypercalcaemia Causes of hypocalcaemia >90% of cases

12
Manifestations of hypercalcaemia
Patients with mild hypercalcemia (calcium <12 mg/dl [3 mmol/L]) may be asymptomatic, or they may report nonspecific symptoms, such as constipation fatigue depression. A serum calcium of 12 to 14 mg/dL (3 to 3.5 mmol/L) may be well-tolerated chronically, while an acute rise to these concentrations may cause marked symptoms, including polyuria polydipsia dehydration anorexia nausea muscle weakness changes in sensorium. In patients with severe hypercalcemia (calcium >14 mg/dL [3.5 mmol/L]), there is often progression of these symptoms
 may be asymptomatic, or they may report nonspecific symptoms, such as. constipation. fatigue. depression. A serum calcium of 12 to 14 mg/dL (3 to 3.5 mmol/L) may be well-tolerated chronically, while an acute rise to these concentrations may cause marked symptoms, including. polyuria. polydipsia. dehydration. anorexia. nausea. muscle weakness. changes in sensorium. In patients with severe hypercalcemia (calcium >14 mg/dL [3.5 mmol/L]), there is often progression of these symptoms.")
13
More manifestations of hypercalcaemia
Neuropsychiatric disturbances A number of mild neuropsychiatric disturbances have been associated with hypercalcemia, mostly in patients with primary hyperparathyroidism. The most common symptoms are anxiety depression cognitive dysfunction More severe symptoms may occur in patients with severe hypercalcemia (calcium >14 mg/dL [3.5 mmol/L]) from any cause. These symptoms are more likely to occur in the elderly and in those with rapidly rising calcium concentrations. lethargy confusion stupor coma GIT abnormalities Gastrointestinal symptoms, such as constipation (may be related to decreased smooth muscle tone and/or abnormal autonomic function) anorexia nausea pancreatitis and peptic ulcer disease occur less frequently (Proposed mechanisms for the development of pancreatitis include deposition of calcium in the pancreatic duct and calcium activation of trypsinogen within the pancreatic parenchyma) peptic ulcer disease (has been described in patients with hypercalcemia due to primary hyperparathyroidism and may be caused by calcium-induced increases in gastrin secretion)
 from any cause. These symptoms are more likely to occur in the elderly and in those with rapidly rising calcium concentrations. lethargy. confusion. stupor. coma. GIT abnormalities Gastrointestinal symptoms, such as. constipation (may be related to decreased smooth muscle tone and/or abnormal autonomic function) anorexia. nausea. pancreatitis and peptic ulcer disease occur less frequently (Proposed mechanisms for the development of pancreatitis include deposition of calcium in the pancreatic duct and calcium activation of trypsinogen within the pancreatic parenchyma) peptic ulcer disease (has been described in patients with hypercalcemia due to primary hyperparathyroidism and may be caused by calcium-induced increases in gastrin secretion)")
14
More manifestations of hypercalcaemia
Renal dysfunction The most important renal manifestations are polyuria, resulting from decreased concentrating ability in the distal tubule, nephrolithiasis, and acute and chronic renal insufficiency. Nephrolithiasis When hypercalcemia is due to primary hyperparathyroidism or sarcoidosis, it is often longstanding, and the resulting chronic hypercalciuria may cause nephrolithiasis Renal insufficiency The development of renal insufficiency in individuals with hypercalcemia is related to the degree and duration of hypercalcemia. The combination of polyuria and diminished fluid intake secondary to gastrointestinal symptoms (nausea) can lead to dehydration, which exacerbates hypercalcemia and related symptoms. Cardiovascular disease Although uncommon, severe hypercalcemia can be associated with cardiac arrhythmia. Acute hypercalcemia directly shortens the myocardial action potential, which is reflected in a shortened QT interval. In addition, ST-segment elevation mimicking myocardial infarction has been reported in such patients. Chronic hypercalcemia may lead to deposition of calcium in heart valves, coronary arteries, and myocardial fibers; hypertension; and cardiomyopathy
 can lead to dehydration, which exacerbates hypercalcemia and related symptoms. Cardiovascular disease. Although uncommon, severe hypercalcemia can be associated with cardiac arrhythmia. Acute hypercalcemia directly shortens the myocardial action potential, which is reflected in a shortened QT interval. In addition, ST-segment elevation mimicking myocardial infarction has been reported in such patients. Chronic hypercalcemia may lead to deposition of calcium in heart valves, coronary arteries, and myocardial fibers; hypertension; and cardiomyopathy.")
15
Serum changes in bone disorders

Similar presentations





 builds up the internal frame.>")
 –Free calcium is 1.2 mM.>")

![Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.](/12/3581741/big_thumb.jpg "Ca ++ and P i Homeostasis. Ca ++ in the plasma [Ca ++ ] in plasma: 2.5 mM, of which about ½ is bound and thus physiologically inactive. Ratio of free/bound.>")











 Vitamin D 2 : Ergosterol (pro D 2 ) Ergocalciferol (D 2 ) added to milk and dairy. (Human) Vitamin D 3 : Pro (7-dehydrocholesterol)>")
