Download presentation
Presentation is loading. Please wait.

1
Case Presentations (Lower Gastrointestinal Bleeding) What Would You Do? What We Did!! Eric J. Dozois, MD Division of Colon and Rectal Surgery Mayo Clinic Rochester, Minnesota

2
Goals of the Presentation Interesting cases of LGIB Stimulate discussion - audience Review key points of topic

3
CASE # 1

4
Chief Complaint 67 year old male Called to the intensive care unit to see a patient with bright red blood per rectum

5
History of Present Illness POD # 2Aorto-bi-iliac graft aorto-renal artery graft for aortoiliac disease

6
History of Present Illness In ICU, stable for last 24 hrs HR 90, BP 115/80, Temp 37.5 BRBPR x 2, now watery diarrhea LLQ abdominal pain Hgb = 8, WBC 18, urine output 5cc/hr

7
Past Medical History Cecal angiodysplasia Sigmoid diverticular disease History of colon polyps – s/p polypectomy complicated by postpolypectomy bleed

8
Family History 2 brothers with colon cancer 1 sister with uterine cancer 1 sister with gastric cancer

9
Differential Diagnosis? Colon cancer C. difficile colitis Ischemic colitis Aorto-enteric fistula Colonic/Sb Angiodysplasia Gastric or duodenal ulcer

10
Work Up and Plan ? Resuscitated, transfused, Abx started Stool sent for C. diff colitis Flexible sigmoidoscopy

11
Plan Flex Sig15 – 60 cm loss of vascular pattern intense erythema, purple discoloration

12
Plan?

13
Hospital Course Fluids, optimized hemodynamics More BRBPR, watery diarrhea Worsening LLQ pain, confused HR 130, BP 90/60, T 38.9 Repeat Flex Sig : “ much worse than yesterday !”

14
Plan?

15
Operative Management Left colon/sigmoid, patchy necrosis – Left Hemicolectomy – End Colostomy – Hartmann Pouch How would you manage the rectal stump??

16
Postop Course Discharged from the hospital on POD 14 2 Months later… Emergency Fem – pop Graft thrombosis, emboli 1 Month later…In ER with BRBPR…..

17
Hospital Course On coumadin, INR = 3, Hgb = 7 Admitted to ICU, transfused Passes 400cc amount of bright red blood per RECTUM!

18
Differential Diagnosis? Dis-use Proctitis Ischemic rectal stump Aorto-rectal stump fistula

19
Work Up? Extended “Push” EGD: – Normal Flex sigmoidoscopy: – Fresh blood & clots – Proximal stump has 3 cm ulcer – ? dehiscence of stump

20
CT Angiogram

21
Angiogram

22
Treatment ? Observation….. 12 Hours later - Massive bleed!! – Blood from rectum… – Blood from Colostomy… – Blood per NGT… Now What?

23
Operative Findings 2 liters of blood in abdomen Dehiscence of proximal aortic anastomosis Fistula to 3 rd portion of duodenum Dehiscence of rectal stump Repair of graft and rectal stump

24
Aorto-Enteric Fistula Incidenceless than 1% 4 th portion of duodenum “Herald bleed” - late diagnosis

25
Aorto-Enteric Fistula Risk Factors: – Repair for ruptured aneurysm – Infection, thrombosis, hematoma – Infection, pseudo-aneurysm, fistula

28
Frequency of Signs and Symptoms in Patients with Aorto-Enteric Fistula Proportion Effected (%) GI bleeding (“herald”) 94 Hematemasis 78 Back or Abd pain 48 Melena 46 Shock 33 Pulsatile mass 17 Syncope 10
 GI bleeding ( herald ) 94 Hematemasis 78 Back or Abd pain 48 Melena 46 Shock 33 Pulsatile mass 17 Syncope 10")
29
Diagnostic Tools in Patients with Aorto- enteric Fistula Detection Rate (%) CT 61 Angiography 26 EGD 25 Technetium scan 14 Enteroclysis 13 Colonoscopy 10 Ultrasound 0 Barium enema 0
 CT 61 Angiography 26 EGD 25 Technetium scan 14 Enteroclysis 13 Colonoscopy 10 Ultrasound 0 Barium enema 0")
30
Prognosis - Aorto-Enteric Fistula Early Mortality21% Late Mortality24% 5-Year Survival61% Armstrong et al. J Vasc Surg 2005;42:660

31
Rifampin Graft, Omental Wrap

32
CASE # 2

33
Chief Complaint 9 year old male Bright red blood per rectum!

34
History of Present Illness 4 days of bright red blood per rectum, by day 5 stool was dark colored On first day of bleeding, 5 emesis Now – asymptomatic

35
Past Medical History Attention deficit disorder No bleeding risk factors Family History: – Brother had intussusception age 6mos – Mother has colon polyps age 42

36
Hospital Course Seen in ER – stable, Hg 7 HR 130, BP 80/60 Abd/rectal exam negative Overnight stable, Hgb = 6

37
Differential Diagnosis? Intestinal duplication Juvenile polyp FAP Meckel’s diverticulum IBD

38
Work Up? EGDNegative ColonoscopyNegative Other Tests?

39
Meckel’s Scan Negative

40
Tagged RBC Scan Negative What Now??

41
Second Meckel’s Scan Positive!

42
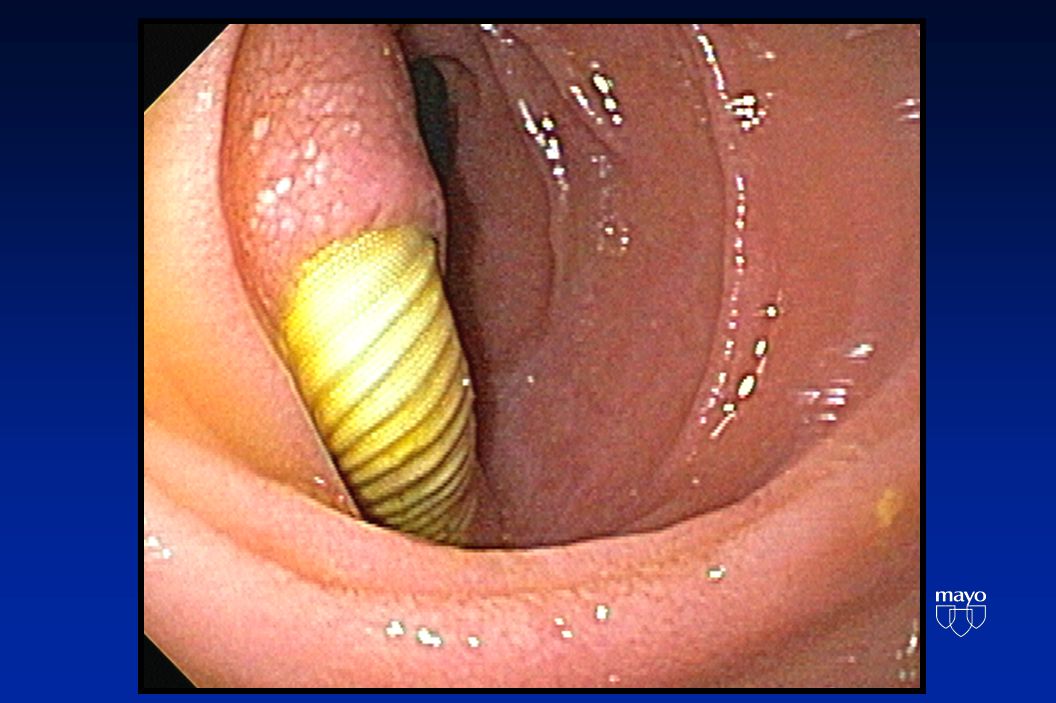
Treatment ? OperationLaparoscopic assisted Meckel’s diverticulectomy, appendectomy Pathology Meckel’s diverticulum with focal heterotopic gastric mucosa

45
Meckel’s Diverticulum (MD) Incidence of MD in general population is 1% Bleeding MD is the most common cause of acute lower GI bleeding in pediatric patients The most common presentation in a child is obstruction, and it is adults bleeding *Park et al. Ann Surg 2005;241:529

46
Meckel’s Diverticulum 16% - are symptomatic Presentation varies – perforation, obstruction, bleeding 29% - ectopic or abnormal tissue Park et al. Ann Surg 2005;241:529

47
Histologic Findings in 180 Pts* Findings Patients No.% Ectopic tissue Gastric 5933 Pancreatic 9 5 Carcinoid 4 2 Duodenal 3 2 Lipoma 2 1 Leiomyosarcoma 10.6 Diverticulitis 4525 Enterolith 11 6 No Abnormality 4625 *Park et al. Ann Surg 2005;241:529

48
Meckel’s Scan In children, sensitivity 85%, specificity 95% In adults, sensitivity 65%, specificity 9%. Sensitivity decreases during acute bleeding Intestinal duplication & nodular lymphoid hyperplasia can give false-positives

49
CASE # 3

50
Chief Complaint 88 yr old male Asked to see in the medical ICU for lower gi bleeding

51
History of Present Illness Outside hospital, passed 800cc blood Hgb 8.0 Colonoscopy - clots & diverticula Transfused 4 units, Hgb remained 8.2 Transferred to Mayo, given 2 units Stable in intensive care unit

52
Past Medical History 10 episodes of LGIB in 20 years, ….4 in last 6 months 1990 - Gastric ulcer Coronary Artery Disease – MI x 2

53
Differential Diagnosis Diverticular bleed Angiodysplasia Carcinoma UGI Source – recurrence of gastric ulcer?

54
Work Up? EGDNGT related erosions only ColonoscopyBlood throughout colon TI intubated – dark blood No active bleeding site Scattered diverticula throughout colon, dense in sigmoid

55
Work Up? Enteroclysis – jejunal & ileal diverticula Tagged RBC scan - Negative Provocative Angiogram : – Access through common femoral artery – IMA, the SMA – Heparin - 5000U – tPA - 10 to 50mg in 5mg increments Now What? Negative

56
Hospital Course Stabilized in ICU, observed Transferred to floor, resumed diet Ready for discharge on HD 7

57
Hospital Course Hypotensive Tachycardic Massive LGIB…. Plan?

58
Surgical Management Abdominal exploration Intraoperative small bowel enteroscopy Total abdominal colectomy, ileostomy

59
GI Bleed of Unknown Source In 95% of cases LGI bleeding can be diagnosed by a combination of endoscopy, scintigraphy, and barium studies (enteroclysis, barium enema) 1 Blind surgical resection is associated with significant re-bleed rates & high mortality 2 1 Welch et al. Adv Surg 1973;7:95 2 Hoedema et al. Dis Colon Rectum 2005;48:2010

60
Mesenteric Angiography *Vernava et al. Dis Colon Rectum 1997;40:846-858.

61
Selective Mesenteric Angiogram Therapeutic Intervention Vasopressin – 90% success, re-bleeding up to 50% – Arrhythmia, pulmonary edema, MI Super Selective Embolization – 100% success, re-bleed 7% – 40% (expertise) – Bowel infarct rare Methylene blue or India ink - localize
 – Bowel infarct rare Methylene blue or India ink - localize")
62
Provocative Angiography* Indicated when all other studies fail Uses anticoagulant (heparin), vasodilator (tolazoline), & thrombolytic agent (tPA) Major side effects are possible Success in small series = 20% - 65% *Ryan et al. J Vasc Interv Radiol 2001;12:1273

63
Surgical Options Directed segmental colectomy Blind segmental colectomy Blind subtotal colectomy

64
Directed Segmental Colectomy Author N Re-bleed Mortality Rate (%) (%) Write 20 00 Browder 17 00 Nath 16 00 Welch 42 102 Boley 27 154 *Vernava et al. Dis Colon Rectum 1997;40:846-858.

65
Blind Segmental Colectomy Author N Re-bleed Mortality Rate (%) (%) McGuire 5 40 20 Casarella 4 50 50 Eaton 24 75 50 Drapanas 23 35 30 *Vernava et al. Dis Colon Rectum 1997;40:846-858.

66
Subtotal Colectomy Author N Re-bleed Mortality Rate (%) (%) Eaton 4 0 0 Drapanas 35 0 11 Welch 10 0 10 Britt 10 0 20 Abcarian 10 60 40 Vernava et al. Dis Colon Rectum 1997;40:846-858

67
Pitfalls of Blind Subtotal Colectomy* ProcedureRe-bleed Final Diagnosis TAC, IRA Yes Bleeding Hemorrhoids TAC, IRA Yes Solitary Rectal Ulcer TAC, IRA Yes LB & SB Ectasias TAC, IRAYes (died) Osler-Weber-Rendu TAC, IRA(2) Yes (both died) Unknown *Abcarian et al. Dis Colon Rectum 1982;25:441-445

68
Pitfalls of Blind Subtotal Colectomy Proximal Disease: – Small bowel Source - tumors, angiodysplasia Distal Disease: – Anorectal source - SRUS, hemorrhoids, fissures, IBD Systemic Disease: – Leukemia, hemophilia, vasculitis, sarcoid

69
Lower GI Bleed Diagnostic Hints SymptomsPossible Diagnosis Abd. pain & bleedingIschemic bowel IBD Ruptured AAA Painless bleeding Diverticular, angiodysplasia, Benign/malignant neoplasm Proctitis

70
Lower GI Bleed Diagnostic Hints Symptoms Possible Diagnosis Bloody diarrhea Infectious colitis, IBD Ischemic bowel Rectal pain & bleeding Fissures Constipation & bleeding Malignancy Diverticular

71
Lower GI Bleed Common Etiologies Adolescence and Children: – Meckel’s diverticulum – Polyps – IBD Adults to age 60: – Neoplasm – IBD – Diverticula

72
Lower GI Bleed Common Causes Age > 60 yrs: – Angiodysplasia – Diverticula – Neoplasm

73
Lower GI Bleed Uncommon Etiologies Ischemic, Infectious (CMV) colitis Ischemic enteritis Postpolypectomy hemorrhage (0.2% - 3%) Anorectal disease (SRUS) Upper GI source (10% - 15%) Small bowel source (3% - 5%) Coagulopathy
 colitis Ischemic enteritis Postpolypectomy hemorrhage (0.2% - 3%) Anorectal disease (SRUS) Upper GI source (10% - 15%) Small bowel source (3% - 5%) Coagulopathy")
74
Future Direction Capsule Endoscopy 11 x 26 mm 2 live images/sec Telemetry 6 hour battery life 2 hours to review

75
Future Direction Capsule Endoscopy

76
Indications for Surgery > 6 unit blood transfused & persistent bleeding > 10 units transfused/24hrs for stable VS Bleeding continues for 72 hrs Re-bleed within 7 days

Similar presentations