Download presentation
Presentation is loading. Please wait.

1
Introduction to simulation and debriefing Role of simulation in Emergency Department DKA Guidelines Shahzad B. Waheed, M.B.B.S, FRCPC, FAAP Assistant Professor Pediatric Critical Care Medicine

2
Outline Introduction to simulation Demonstration of case Basic structure of Debriefing Diabetic Ketoacidosis

3
Introduction to Simulation

4
Wha What is Simulation Simulation is a technique – not a technology Use in Medical Education is to: “replace or amplify real experiences with guided experiences that evoke or replicate aspects of the real world.”

5
Definition Simulation is defined as: “the artificial replication of sufficient components of a real-world situation to achieve certain goals.”

6
Simulation Based Medical Education Simulation is a complimentary teaching method in the medical profession: “any educational activity that uses simultative aids to enhance medical educational message” “not to replace traditional methods, but to add to”

7
Why Simulation 1999 Institute of Medicine report – ‘to err is human’ Highlighted the cognitive and technical errors in medical education Patient safety became an important agenda item Licensing and governing bodies challenged to improve physician confidence and patient safety

8
Ethical Theme of Simulation 1. Best standards of care and training 2. Error management and patient safety 3. Social justice – resource allocation “patients are to be protected whenever possible and they are not commodities to be used as conveniences of training.”

9
Best Standards Best standard for patient care First do no harm to patients Using patients as learning instruments is only justified when all approaches to minimize risks have been taken Simulation allows trainees’ first encounters with real patients to be at higher technical and clinical proficiencies

10
Best Standards Best standard for education Responsibility of educators to provide clinicians with best training Best standard for evaluation Traditional evaluation focused on cognitive domain With simulation can assess attitudinal and psychomotor as well

11
Error management Even with supervision it is inevitable that trainees cause preventable injuries In clinical setting errors must be stopped promptly In simulation errors may be allowed to progress Errors can occur at any level in medical education

12
Social Justice Basic principle of distributive justice states: Citizens equally share the risks of medical innovation, research and practice training Most teaching institutions are urban and provide disproportionate care to the poor and under privileged SBME may help equilibrate this imbalance

13
How could we use it To improve procedural and surgical skills Helps in improving communication Can be used to diagnose deficiencies in team management of critical care issues Can be used to help assess competency

14
Reviewed 40 consecutive charts in preceding 6 months Intervention was a instruction of LP on manikin and proforma Prospectively reviewed 25 next consecutive patient charts Findings: 4/12 clinical markers improved to 12/12 (p<0.01) Improved charting Change in behavior of junior staff No change in % of traumatic taps
 Improved charting Change in behavior of junior staff No change in % of traumatic taps")
16
Demonstration of Case

17
http://www.youtube.com/watch?v=0YJxz-Sxx90

18
Glucometer reading: 32mmol/L

19
Cap Gas: pH 7.05, pCO 2 18, pO 2 60 HCO3 3 BE -12 Blood glucose is 35mmol/L

22
50 units of regular insulin in 50 cc of Normal Saline Start insulin at 0.1 unit/kg/hr If Patient weight is 12 kg therefore you need to run at 1.2 cc/hr

23
Cap Gas: pH 7.05, pCO 2 18, pO 2 60 HCO3 3 BE -12 Blood glucose is 35mmol/L

24
HR 100 RR 25 BP 100/50 MAP 55 GCS 11

25
Structure of Debriefing

26
Basic Structure of Debriefing Venting Emotional energy Clarify what you want to achieve during the debrief / ground rules How do you feel now? What was it like in the scenario? Did it feel realistic?

27
Descriptive Phase Summary of the events – hot seat / leader Summary of the events – hot seat / leader Chronological order Chronological order Original problems, assessment, treatments Original problems, assessment, treatments “Can you summarise the events of the scenario and what you did” Pull in the rest of the group

28
Analytical Phase Participants analyse the events in the scenario Participants analyse the events in the scenario key CRM principles & medical / technical aspects key CRM principles & medical / technical aspects Any ‘golden moments’ Any ‘golden moments’ Identify weaknesses Identify strengths, then weaknesses ‘’What did you do well in this scenario – why?’’ ‘’Anything you would you like to do

29
Generalisation Generalising what they have learnt to the next scenario. Generalising what they have learnt to the next scenario. Generalising to the workplace in the future. Generalising to the workplace in the future. “Have you taken something new away from the scenario?” “Will this change any aspect of your practice at work tomorrow?” “What have you learnt?”

30
SHAHZAD B. WAHEED M.B.B.S,FRCPC,FAAP ASSISTANT PROFESSOR PEDIATRIC CRITICAL CARE MEDICINE Diabetic Ketoacidosis

31
Objectives Definition Epidemiology Pathophysiology Risk Factors Complications Treatment Prevention Conclusion

32
Archive disease of Child 2004;89(2) 188-94 Definition Hyperglycemia 14 mmol/L Venous pH <7.3 Na Bicarbonate < 15mmol/L Moderate or large ketones level (Urine/Blood )
 Definition Hyperglycemia 14 mmol/L Venous pH <7.3 Na Bicarbonate < 15mmol/L Moderate or large ketones level (Urine/Blood )")
33
Newfoundland and Labrador has one of the highest rates of Type I diabetes worldwide. Newhook et al Pediatric Diabetes 2008

34
Prevalence of DKA at the Diagnosis of T1D North America 29% Europe 15%-67% Developing countries 42-85% Pediatrics 2008;121(5):e1258–66 Arch Dis Child 2004;89(2):188–94 Pediatric Diabetes 2006;7(2):101–7 Diabetologia 2001;44(Suppl 3):B75–80
:e1258–66 Arch Dis Child 2004;89(2):188–94 Pediatric Diabetes 2006;7(2):101–7 Diabetologia 2001;44(Suppl 3):B75–80")
35
Incidence of DKA in established T1D Varies from 1 to 12 per 100 person-years Increase in females than males Associated with Insulin Omission Treatment errors

37
Pathophysiology Decrease Insulin Increase glucagon, catecholamine, cortisol and growth hormone Lipolysis Production of Ketones Metabolic acidosis and Hyperglycemia Advances in Pediatrics 57 (2010) 247–267
 247–267")
38
Risk Factors for DKA Lower Socioeconomic StatusLow Societal awarenessHigh-dose glucocorticoidsAtypical antipsychoticsDiazoxideImmunosuppressive drugs Pediatrics 2008;121(5):e1258–66 Diabetes 2007;54(Suppl 1):A63–4 Clinical Pediatrics (Phila) 2003;42(7):591–7
:e1258–66 Diabetes 2007;54(Suppl 1):A63–4 Clinical Pediatrics (Phila) 2003;42(7):591–7")
39
Risk Factors for recurrent DKA Lower socioeconomic status Omit Insulin Insulin pump Eating disorder Psychiatric Disorder JAMA 2002;287(19):2511–8. J Pediatr 2001;139(2):197–203
:197–203.")
40
Complications of DKA ShockCerebral EdemaHyperkalemia or HypokalemiaHypoglycemiaHypophosphatemia N Engl J Med 2001;344(4):264–9Arch Dis Child 2001;85(1):16–22
:264–9Arch Dis Child 2001;85(1):16–22")
41
Causes of Morbidity and Mortality Cerebral edemaHypokalemia or Hyperkalemia ThrombosisSepsis Aspiration pneumonia ARDS/Pulmonary edemaAcute renal failure/Rhabdomyolysis Advances in Pediatrics 57 (2010) 247–267
 247–267")
42
Diagnosis PolyuriaPolydipsiaDehydrationGI symptomsDysuria or Thrush or TachypneaSigns of DehydrationDelayed Capillary refillAcetone-fruity breath or Kussmaul breathingLaboratory Tests Advances in Pediatrics 57 (2010) 247–267
 247–267")
43
Management Emergency Assessment Biochemical assessment Supportive measures Further clinical and biochemical monitoring Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
44
Emergency Assessment Confirm the diagnosis Look for evidence of Infection Assess severity of dehydration Prolong Capillary refillAbnormal skin turgorHyperpnea Dry mucus membrane, Sunken eyes, absent tears, weak pulses and cool extremities > 10% dehydration may presents with weak pulses, oliguria and Hypotension Assess level of consciousness Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
45
Biochemical Assessment Blood glucose and Hematocrit Urine or blood ketones Na,K,Ca,PO4, HCO3,BUN and Cr Pseudohyponatremia Measured Na +0.36 x (glucose-5.6) Blood gasSerum osmolality 2(Na+K) + Glucose+ BUN/2.8 (mOsm/L) Septic work up if indicated CT head if indicated Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
48
Goals of treatment Correct dehydration Restore blood glucose to near normal Identify and treat any precipitating event Avoid complications of therapy Correct acidosis and reverse ketosis Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
49
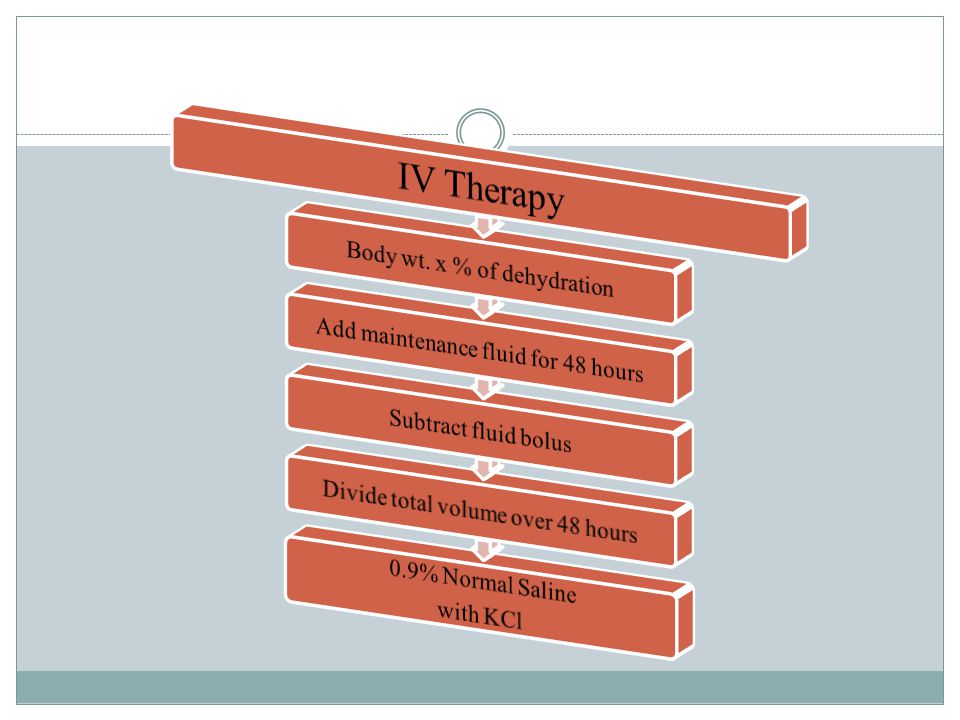
Objective of fluid management Restoration of Circulating volume Reduction of risk of cerebral edema Improve GFR with enhance clearance of glucose and ketones from the blood Replacement of Na, ECF and intracellular fluid deficit of H2O Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
53
Insulin Therapy Start insulin infusion @ 0.1 u/kg/hr 1-2 hours after fluid replacement therapy Continue insulin infusion until resolution of DKA Add dextrose once glucose level is b/w 14-17 mmol/L May need to add dextrose sooner if glucose is dropping rapidly (> 5 mmol/L/h) Aim to keep blood glucose level at about 11 mmol/L until resolution of DKA Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
54
Absolute Potassium Depletion Absolute Potassium Depletion Serum potassium may be normal to high initially Serum potassium may be normal to high initially Add potassium when K< 5 and with urination Add potassium when K< 5 and with urination K >5.5 – no potassium in IVF K >5.5 – no potassium in IVF K 4.5 – 5.5 – 20 meq/L K+ K 4.5 – 5.5 – 20 meq/L K+ K <4.5 – 40 meq/L K+ K <4.5 – 40 meq/L K+

55
Potassium Intracellular K depletion Increase plasma osmolalityGlycogenolysis and proteolysisVomiting Replacement If patient is Hypokalemic at presentation start K supplement from beginning If patient is Hyperkalemia, wait till K level drops below 4.5 mmol/L and documented urine output Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
56
Intracellular PO4 depletion Osmotic DiuresisInsulin infusion Hypophosphatemia may be treated with phosphate infusion PO4 replacemet may cause hypocalcemia Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
57
Acidosis Insulin infusion stops ketoacid production Fluid therapy improves tissue perfusion and renal function, increases renal excretion of organic acids HCO3 therapy is contraindicated except if pH < 6.9 with hemodynamic compromise Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
58
Cerebral Edema Incidence 0.5% to 0.9% High Risk Age < 5 yearsNew onset DMLonger duration of SxSeverely Dehydrated Acidosis pH < 7.1 pCO2 < 20Fluid >50cc/kg first 4 hrsHigh BUNNaHCO3 treatment Insulin tx before rehydration Mortality 21-24% Archives Disease Child 2001;85(1):16–22 New England Journal of Medicine 2001;344(4):264–9Pediatric Neurolurolgy1999;21(4):721–7
:16–22 New England Journal of Medicine 2001;344(4):264–9Pediatric Neurolurolgy1999;21(4):721–7")
60
New England Journal of Medicine 2001;344(4):264–9
:264–9")
61
Treatment of Cerebral edema Reduce the fluid administration by one-thirdGive mannitol 0.5-1 g/kg IV over 20 minutes Hypertonic saline 5-10 ml/kg over 30 min as an alternative to mannitol or second line of therapy Elevate the head of the bedIntubation may be necessaryCT head to r/o thrombosis or hemorrhage New England Journal of Medicine 2001;344(4):264–9
:264–9")
62
When ketoacidosis is resolving (mild acidosis or ketosis may be present) Tolerates oral fluid and diet SC injection should be given 10-15 min (rapid acting) or 1-2 hours (regular insulin) before stopping insulin infusion SC Insulin Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133.")
63
Advances in Pediatrics 57 (2010) 247–267
 247–267")
64
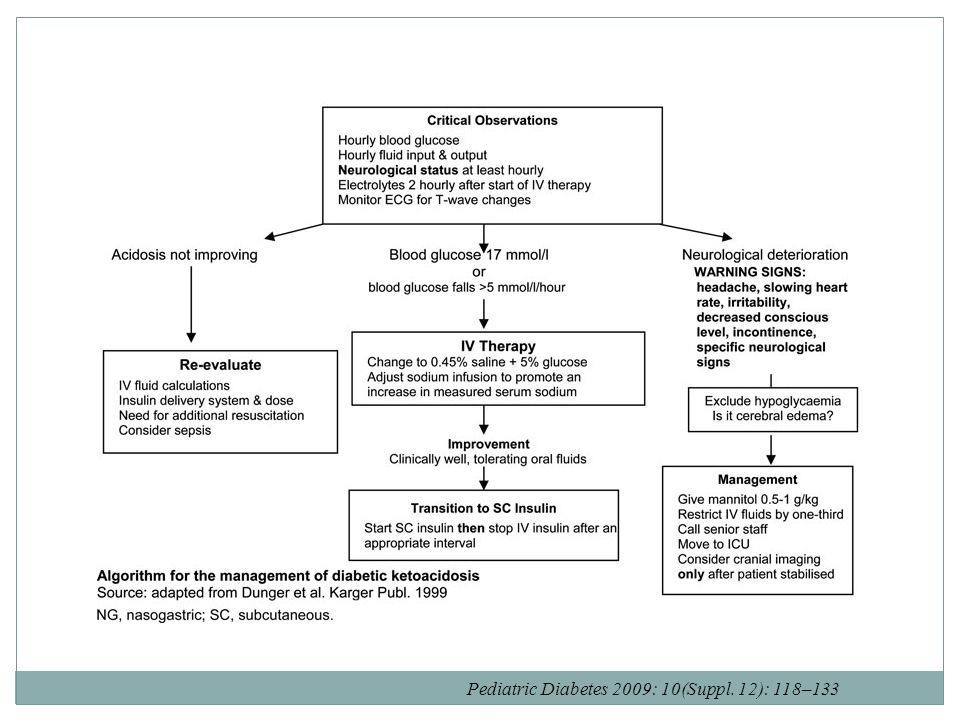
Pediatric Diabetes 2009: 10(Suppl. 12): 118–133
: 118–133")
66
4 years old male with a history of polyuria, polydipsia x 3 weeks, vomiting x 24hrs,agitated, equal pupils, Capillary refill 3 secconds, good pulses presented to ER at 02:00 Vitals Sings: T 37C, HR 165, RR 50, BP 85/45 MAP 55 O2 sat 95% on RA Next step

67
Labs: Na 134 K 5.5 Cl 98 HCO3 8 BUN 12 Cr 77 Glucose 32 Gas: pH 7.1 PCO2 17 PO2 85 Lacatate 1.2 Next Step

68
Dose of benzodiazapine?Fluid bolus?NaHCO3?Mannitol?

70
Conclusion Simulation is a complimentary teaching method in the medical profession Simulation could be used to improve patient safetyDebriefing is essential component of simulation

71
Conclusion DKA is caused by either relative or absolute insulin deficiency Begin with fluid replacement before starting insulin therapySubsequent fluid administration over 48 hrs Begin with 0.1 U/kg/h. 1–2 hours after starting fluid replacement therapy

72
Conclusion May need to add dextrose early if blood glucose is dropping quickly No evidence that HCO3 is effective or safe except in rare circumstances Monitor signs of cerebral edema May use mannitol or Hypertonic solution if suspicion of cerebral edema All cases of recurrent DKA are preventable

Similar presentations