Download presentation
Presentation is loading. Please wait.

1
SHAWN RICHARDS, MD MOSES LAKE CLINIC MOSES LAKE, WA Common Retinal Diseases

2
Anatomy Review

4
Retina Photosensitive neurosensory tissue Photoreceptors Rods – Rhodopsin Cones – Vitamin A and opsin Support cells Ganglion cells

5
Retinal Layers

6
www.siumed.edu/~dking2/ssb/EE020b.htm David King, PhD

7
Anatomy of the Retina Macula Fovea – avascular, cones Foveola – only photoreceptors Equatorial retina – mainly rods Peripheral retina Ora serrata Pars plana

8
Retinal Layers

9
Retinal Vasculature Central Retinal Artery Branch of Ophthalmic Artery From Internal Carotid Artery Inner 2/3 of retina Central Retinal Vein Capillaries – inner blood-retina barrier

10
Retinal Pigment Epithelium Serves many functions Photoreceptor metabolism Outer blood-retina barrier Potential space

11
Common Retinal Diseases Diabetic eye disease Retinopathy Edema Age Related Macular Degeneration (ARMD) Non-exudative Exudative Vitreomacular traction (VMT) Posterior Vitreous Detachment (PVD)
 Non-exudative Exudative Vitreomacular traction (VMT) Posterior Vitreous Detachment (PVD)")
12
Diabetes Mellitus Prevalence Leading Cause of Blindness in pts. Ages 20-64 Second leading cause overall Progression At onset of Type I No Retinopathy After 7 years 50% have some DR Rare in Kids under 10 After 20 years 99% w/ Type I 60% w/ Type II

13
Diabetes Mellitus Earliest signs in the eye Loss of pericytes - Leads to endothelial cell decompensation Basement membrane thickening - Hyperglycemia is a stimulus for increased protein synthesis, especially glycoproteins which are an important component of B.M. These lead to capillary occlusion, decrease nutrient diffusion and leakage

14
Loss of Pericytes

15
Pathogenesis Sorbitol Toxicity When glucose concentration is high, the aldose reductase pathway is used Aldose reductase converts glucose to sorbitol and fructose Sorbitol and fructose enter cells easily but cannot exit easily, thus causing osmotic effects. This causes cataract, neuropathy, and retinopathy. Aldose reductase also converts galactose to galactitol which causes the galactosemia cataract.

16
Pathogenesis Circulatory Changes Hyperglycemia causes loss of autoregulation The severity of loss is proportional to severity of DR Autoregulation is improved after PRP Hyperglycemia causes increased oxygen utilization Increased oxygen utilization leads to Relative hypoxia Vasodilation Upregulation of VEGF

17
Diabetic Retinopathy Classification of diabetic retinopathy: Nonproliferative Diabetic Retinopathy (NPDR) Mild, Moderate, Severe, Very Severe Proliferative Diabetic Retinopathy (PDR) Early, High-risk, advanced Progression is in a stepwise fashion
 Mild, Moderate, Severe, Very Severe Proliferative Diabetic Retinopathy (PDR) Early, High-risk, advanced Progression is in a stepwise fashion")
18
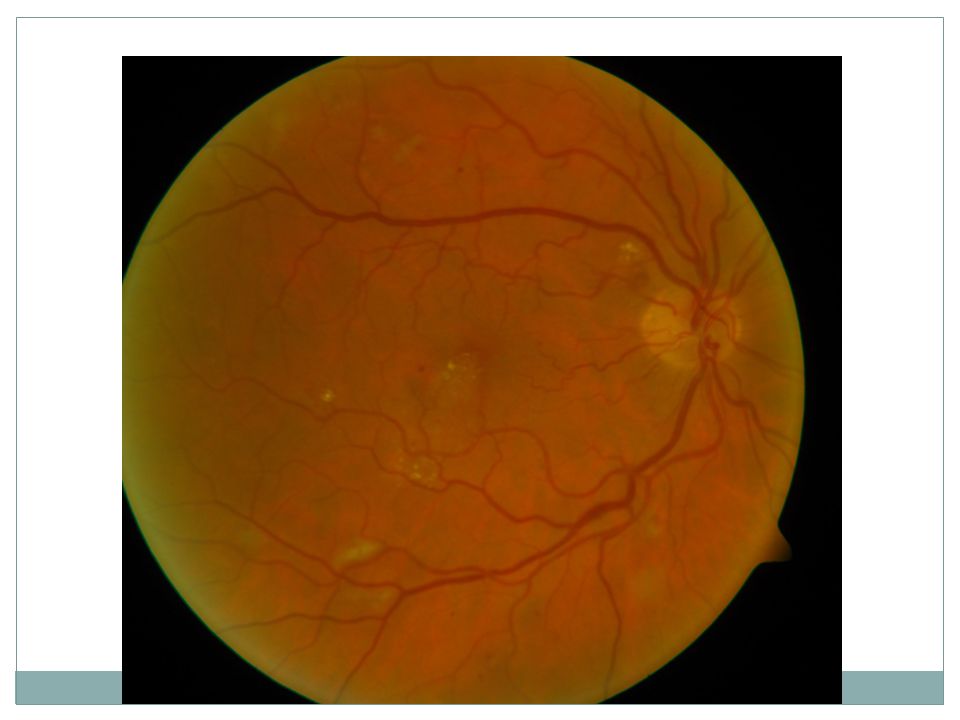
Nonproliferative Diabetic Retinopathy (NPDR) NPDR – (background) Limited to Retina by ILM Hemorrhages: Dot-Blot, Flame Hard exudates (lipid deposition in outer and inner plexiform layers) Capillary microaneurysms
 NPDR – (background) Limited to Retina by ILM Hemorrhages: Dot-Blot, Flame Hard exudates (lipid deposition in outer and inner plexiform layers) Capillary microaneurysms")
23
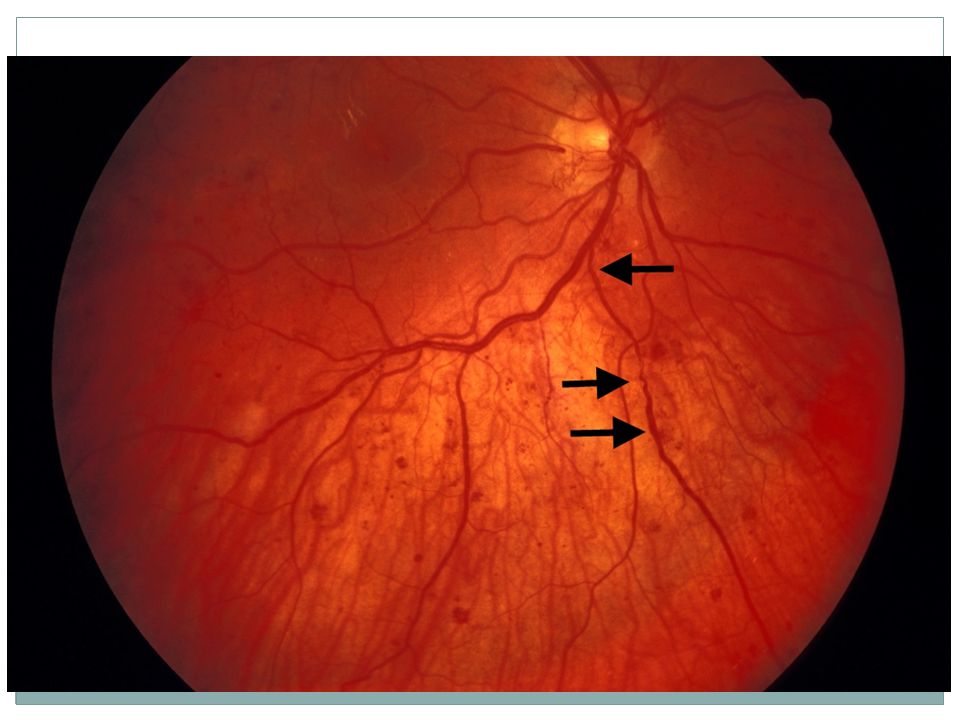
NPDR Macular edema: focal or diffuse Venous Dilation and Beading Intraretinal Microvascular Abnormalities (IRMA) Capillary occlusions Cotton wool spots (RNFL infarcts) “soft exudates, SE” Areas of non-perfusion on fluorescein angiography
 Capillary occlusions Cotton wool spots (RNFL infarcts) soft exudates, SE Areas of non-perfusion on fluorescein angiography")
24
NPDR The ETDRS 4:2:1 rule Severe NPDR is defined as Severe hemorrhages in 4 quadrants Or Venous abnormalities in 2 or more quadrants Or Intraretinal microvascular abnormality (IRMA) in one or more quadrants One of the above: severe - 15% chance of developing proliferative retinopathy within one year Two or more: very severe - 45% chance of developing proliferative retinopathy within one year
 in one or more quadrants One of the above: severe - 15% chance of developing proliferative retinopathy within one year Two or more: very severe - 45% chance of developing proliferative retinopathy within one year")
27
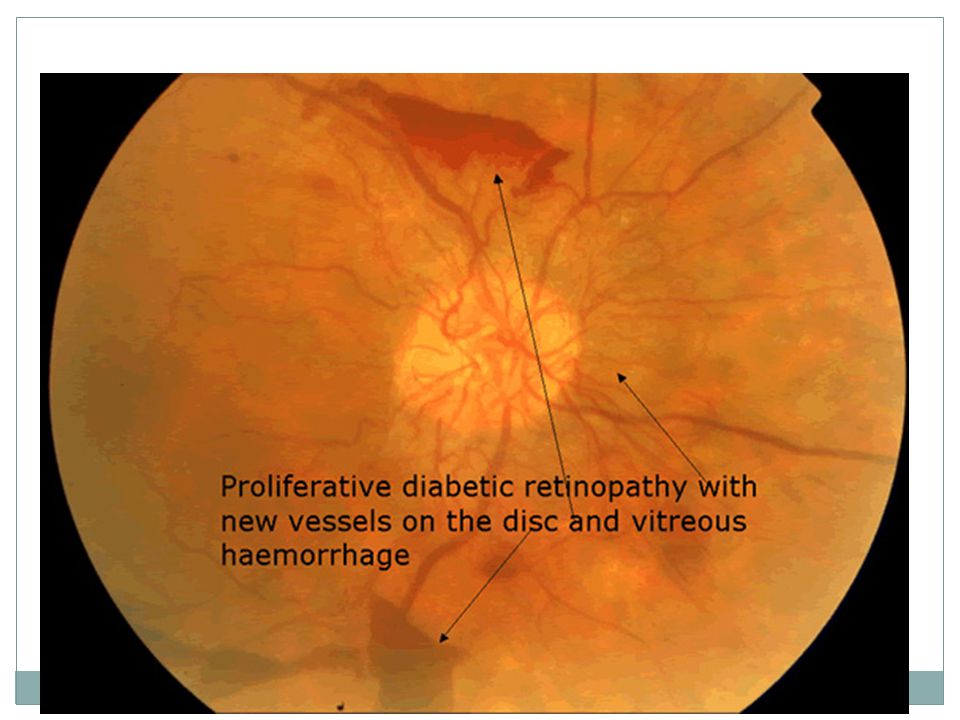
Proliferative Diabetic Retinopathy (PDR) Extraretinal fibrovascular extension (above ILM): Neovascularization of disc (NVD) Neovascularization elsewhere (NVE) Vitreous hemorrhage (VH) Tractional retinal detachment (TRD) Or combined tractional/rhegmatogenous RD Increased risk of CVA, MI, diabetic nephropathy and death
 Extraretinal fibrovascular extension (above ILM): Neovascularization of disc (NVD) Neovascularization elsewhere (NVE) Vitreous hemorrhage (VH) Tractional retinal detachment (TRD) Or combined tractional/rhegmatogenous RD Increased risk of CVA, MI, diabetic nephropathy and death")
28
Proliferative Diabetic Retinopathy High Risk Characteristics determined by the Diabetic Retinopathy Study (DRS) NVD greater then 1/4 to 1/3 disc area Any NVD with VH NVE with VH
 NVD greater then 1/4 to 1/3 disc area Any NVD with VH NVE with VH")
32
Causes for Vision Loss Macular Ischemia (Capillary Occlusion) Sequelae from neovascularization NVG, NVD, NVE, VH, RRD, TRD, Combined RRD/TRD, Laser, etc. Macular Edema (Capillary Leakage)
.")
33
Macular Ischemia

34
Sequelae From Neovascularization Panretinal Photocoagulation (PRP) Rational: conditions which destroy retina seem to prevent diabetic retinopathy Technique: 1600 to 2000 burns, 500 micron spot size burns from 2DD temporal to the FAZ out to the periphery. Theories for the efficacy of PRP Decreases quantity of vasoproliferative factors Improves the diffusion of oxygen from the choroid Reduces retinal oxygen demand Studies supporting PRP Diabetic Retinopathy Study Early Treatment Diabetic Retinopathy Study (ETDRS)
.")
35
PanRetinal Photocoagulation

36
Diabetic Retinopathy Study Panretinal photocoagulation (PRP) Eyes with PDR or very severe NPDR The DRS proved the effectiveness of PRP at preventing severe vision loss at 5 years Four major risk groups. V.A. < 5/200 with RX:without RX 1. NVD <1/2 DD (+VH)4.3%:25.6% 2. NVD>1/2 DD (-VH)8.5%:26.2% 3.NVD>1/2 DD (+VH)20.1%:36.9% 4.NVE>1/2DD (+VH)7.2%:29.7%
4.3%:25.6% 2. NVD>1/2 DD (-VH)8.5%:26.2% 3.NVD>1/2 DD (+VH)20.1%:36.9% 4.NVE>1/2DD (+VH)7.2%:29.7%.")
37
Early Treatment Diabetic Retinopathy Study (ETDRS) Scatter (PRP) Laser vs. observation Patients had mild NPDR to early PDR Aspirin 650 mg vs. placebo

38
ETDRS Results: Aspirin use recommended in DM PRP for high risk PDR reduces the incidence of severe visual loss (VA<20/800) from 30% to 15% over a three year period. NVI is not part of “HRC” but is ominous and PRP is indicated.

39
ETDRS Results Treatment of severe NPDR and with PDR less than HRC. Early PRP reduces the rate at which eyes with severe NPDR and early PDR progress to HRC by 50%, but that PRP causes an early reduction in visual acuity. PRP not recommended for mild to mod NPDR

40
ETDRS Results: Most retina specialists do not give PRP to eyes with severe NPDR and neovascularization less than HRC. However, some strongly consider PRP in patients who: Have severe bilateral NPDR Have rapidly progressing NPDR Have had a poor outcome in one eye Cannot be relied upon to return for follow-up Are pregnant

41
But what if…

42
Vitreous Hemorrhage in PDR B scan if too dense Observe if no RD PRP when able Consider other factors (fellow eye, previous PRP, NVI, patient needs)
")
43
Diabetic Vitrectomy Indications Dense, nonclearing VH TRD involving or threatening the macula Combined TRD and RRD Diffuse DME associated with posterior hyaloid traction Significant recurrent VH despite maximal PRP Diabetic Retinopathy Vitrectomy Study Type I DM with dense VH – better visual outcomes with early PPV (1-6 months) Type II DM with dense VH – no difference in visual outcome
 Type II DM with dense VH – no difference in visual outcome")
44
Diabetic Macular Edema Most common cause of visual loss in diabetics Also the most treatable Due to abnormal retinal vasculature permeability Types Focal – leakage from specific capillary lesions Diffuse – widespread retinal capillary abnormalities Diagnosis Slit lamp biomicroscopy Fluorescein angiography

45
Diabetic Macular Edema The Role of fluorescein angiography To prove that the patients decreased vision is caused by macular edema and not by ischemia. To identify leaking microaneurysms and areas of NV To identify areas of diffuse capillary leakage To identify areas of capillary non-perfusion

46
Fluorescein Angiography

47
Risks Pain Extravasation Nausea/vomiting – 10% Anaphylaxis – 0.001% Death Considerations Pregnancy Renal disease

48
Optical Coherence Tomography Based on imaging reflected light Analogous to ultrasound – optical vs. acoustic reflectivity Produces cross-sectional images of ocular tissue Micrometer resolution Noninvasive, noncontact Quick No Death

49
Optical Coherence Tomography

50
Diabetic macular edema - ETDRS Eyes with diabetic macular edema Vision of 20/200 or better Argon grid laser End point was a doubling of the visual angle 20/30 20/60 20/40 20/80 3 year results – doubling of visual angle Treated --12% Untreated – 24% Treated eyes had an increased chance of halving of the visual angle

51
Diabetic Macular Edema Definition of clinically significant macular edema from ETDRS: Retinal thickening at or within 500 microns of the center of the foveal avascular zone (FAZ) Hard exudates at or within 500 microns of the center of the FAZ, If associated with edema Retinal thickening one disc area or larger within one disc area of the FAZ Visual acuity is not a criterion for treatment
 Hard exudates at or within 500 microns of the center of the FAZ, If associated with edema Retinal thickening one disc area or larger within one disc area of the FAZ Visual acuity is not a criterion for treatment")
52
Diabetic Macular Edema ETDRS treatment strategy Try to close all leaking microaneurysms End point: whitening or blackening Do not treat within 500 microns of the center of the FAZ Use a grid (100 or 200 micron) pattern in areas of: Diffuse capillary leakage Areas of capillary nonperfusion
 pattern in areas of: Diffuse capillary leakage Areas of capillary nonperfusion")
53
Diabetic Macular Edema Prognosis is not good with: Significant central capillary nonperfusion Severe cystoid macular edema Hard exudates in the FAZ Visual acuity 20/200 or less Nevertheless, these eyes can have a statistically significant improvement over untreated eyes with laser therapy

54
Diabetic Macular Edema Follow up: The treatment may cause an initial worsening of vision It may take a few months before the benefits are seen Indications for retreatment. Persistent macular edema Do not retreat for residual hard exudates if not associated with macular edema.

55
Diabetic Macular Edema Follow up continued: Consider treatment as close as 300 microns of the center of the FAZ if: There is residual macular edema Leaking spots can be clearly identified The treatment will not increase foveal capillary nonperfusion

56
Diabetic Macular Edema Risks of grid/focal laser Paracentral scotoma Transient increased edema Choroidal neovascularization Subretinal fibrosis Laser creep Inadvertent foveal burn

57
That was 1985

58
Diabetic Retinopathy Clinical Research Network 854 eyes Vision between 20/32 and 20/320 Diabetic macular edema Four arms Ranibizumab + prompt laser Ranibizumab + deferred laser Triamcinolone + prompt laser Sham injection + prompt laser

59
Diabetic Retinopathy Clinical Research Network 12 month results – visual acuity increase Ranibizumab + prompt laser – 9 letters(P<0.001) Ranibizumab + deferred laser – 9 letters (P<0.001) Triamcinolone + prompt laser – 4 letters Sham injection + prompt laser – 3 letters 12 months results – CMT decrease Ranibizumab + prompt laser – 131 um(P<0.001) Ranibizumab + deferred laser – 137 um(P<0.001) Triamcinolone + prompt laser – 127 um(P<0.001) Sham injection + prompt laser – 102 um
 Ranibizumab + deferred laser – 9 letters (P<0.001) Triamcinolone + prompt laser – 4 letters Sham injection + prompt laser – 3 letters 12 months results – CMT decrease Ranibizumab + prompt laser – 131 um(P<0.001) Ranibizumab + deferred laser – 137 um(P<0.001) Triamcinolone + prompt laser – 127 um(P<0.001) Sham injection + prompt laser – 102 um")
60
RESTORE Study 354 patients Vision between 20/32 and 20/160 Visual impairment due to DME Three arms Ranibizumab + sham laser Ranibizumab + laser Sham injection + laser Ranibizumab and ranibizumab + laser were superior to laser alone at 12 months Improvement of BCVA Mean central retinal thickness

61
RESTORE Study 12 month results – visual acuity increase Ranibizumab + sham laser6.1 lettersP<0.0001 Ranibizumab + laser5.9 lettersP<0.0001 Sham injection + laser0.8 letters 12 month results – CMT decrease Ranibizumab + sham laser118.7 umP<0.001 Ranibizumab + laser128.3 umP<0.001 Sham injection + laser 61.3 um

62
Diabetic Macular edema 2 weeks ago Vision 20/400 CMT of 498 Treated with intravitreal ranibizumab 0.3 mg 10 days later Vision 20/80 CMT of 354

63
Diabetes Control and Complications Trial Type 1 diabetics Slow development +/- progression 726 pts w/o DR 715 pts w/ mild to mod DR Treatment and Control Groups Treatment—4 injections per day or pump— End goal was hgb A1C <6.1% Control – 1 to 2 injections per day Mean follow up – 6.5 years

64
DCCT Results Treatment Group: Decreased risk of development of retinopathy by 76%, nephropathy - 54%, neuropathy - 60%. Slowed progression of retinopathy by 54% Mortality was higher in the Treatment Group, but the difference was not statistically significant between the groups

65
Clinical Observation Type I: Initial exam 5 years after diagnosis Type II: At time of diagnosis If pt. becomes pregnant: examine in first trimester and then as needed based upon examination and control Mild – 9 months Mod – 6 months Severe/CSME – 2-4 months PDR – 2-3 months

66
Prevention is best medicine Some abnormalities are reversible with good control in humans Vitreous fluorophotometry Photostress test Oscillatory potential Capillary basement membrane thickness

67
Role of the Practitioner Tight Blood Sugar/Blood Pressure/lipid control D/C Smoking Control of glucose is good no matter how long (DCCT), especially if before retinopathy develops
, especially if before retinopathy develops")
68
Hypertensive Retinopathy Vasoconstriction Arteriole narrowing Arteriosclerosis Copper and silver wiring Arterio-venous nicking

69
Hypertensive Retinopathy Retinal hemorrhage Macular edema and exudate Optic disc edema Due to acute, severe HTN Treatment – Control blood pressure

70
Age Related Macular Degeneration Leading cause of severe central visual acuity loss in people over 50 years of age Affects 15 million North Americans Types Nonexudative (dry) – 85-90% Exudative (wet) – 10-15%
 – 85-90% Exudative (wet) – 10-15%")
71
ARMD Risk – Framingham Eye Study 65 to 74 years old – 6.4% Over 75 years old – 19.7% Risk factors Family history- Hypertension Smoking- Hypercholesterolemia Hyperopia- Female gender Light iris color- Cardiovascular disease

72
Nonexudative ARMD Drusen Focal hyperpigmentation Geographic atrophy

73
AREDS Daily supplementation Vitamin C – 500 mg Vitamin E – 400 IU Beta carotene – 15 mg Zinc oxide – 80 mg Cupric oxide – 2 mg In patients with intermediate ARMD or advanced unilateral ARMD 25% reduction of risk for progression to advanced ARMD 19% risk reduction in rates of moderate vision loss by 5 years

74
Indications for Vitamins Individuals with high risk for progression and vision loss Extensive intermediate drusen At least one large druse Noncentral geographic atrophy Advanced ARMD in one eye Smokers – avoid beta carotene Possible increased risk of thromboembolic events

75
Exudative ARMD Choroidal neovascular membrane Subretinal fluid Subretinal blood Subretinal lipid Irregular elevation of the RPE Subretinal gray-white lesion Cystoid macular edema

76
Exudative ARMD Choroidal neovascular membrane Classic Occult

77
Treatment Nothing Conventional laser Photodynamic therapy Light activated - short-lived reactive oxygen radicals

78
Treatment Laser photocoagulation

79
Colon Cancer Bevacizumab Full length monoclonal antibody to VEGF Ranibizumab Antibody fragment (Fab) to VEGF
 to VEGF")
80
MARINA Study 716 patients Minimally classic or occult CNVM Three arms 0.3 mg ranibizumab monthly 0.5 mg ranibizumab monthly Sham injection monthly

81
ETDRS Chart

82
MARINA Study 12 month results Lost less than 15 letters 0.3 mg – 94.5%(P<0.001) 0.5 mg – 94.6%(P<0.001) Sham – 62.2% Gained 15 or more letters 0.3 mg – 24.8%(P<0.001) 0.5 mg – 33.8%(P<0.001) Sham – 5.0%
 0.5 mg – 94.6%(P<0.001) Sham – 62.2% Gained 15 or more letters 0.3 mg – 24.8%(P<0.001) 0.5 mg – 33.8%(P<0.001) Sham – 5.0%")
83
MARINA Study 12 month results Average change in visual acuity 0.3 mg – 6.5 letter increase(P<0.001) 0.5 mg – 7.2 letter increase(P<0.001) Sham – 10.4 letter decrease
 0.5 mg – 7.2 letter increase(P<0.001) Sham – 10.4 letter decrease")
84
ANCHOR Study 423 patients Predominantly classic CNVM 3 arms 0.3 mg ranibizumab monthly + sham PDT 0.5 mg ranibizumab monthly + sham PDT Sham injection monthly + PDT

85
ANCHOR Study 24 month results Lost less than 15 letters 0.3 mg – 89.9%(P<0.001) 0.5 mg – 90.0%(P<0.001) PDT – 65.7% Gained 15 or more letters 0.3 mg – 34.0%(P<0.001) 0.5 mg – 41.0%(P<0.001) PDT – 6.3%
 0.5 mg – 90.0%(P<0.001) PDT – 65.7% Gained 15 or more letters 0.3 mg – 34.0%(P<0.001) 0.5 mg – 41.0%(P<0.001) PDT – 6.3%")
86
ANCHOR Study 24 month results Average change in visual acuity 0.3 mg – 8.1 letter increase(P<0.001) 0.5 mg – 10.7 letter increase(P<0.001) PDT – 9.8 letter decrease
 0.5 mg – 10.7 letter increase(P<0.001) PDT – 9.8 letter decrease")
87
Anti VEGF Cost Ranibizumab - $2,000 per injection Bevacizumab - $50 per injection Off label Difference $1,950 per injection $23,400 per year Ramen noodles 117,000 packs

88
CATT Study 1,107 patients Neovascular ARMD – no differentiation 4 arms Ranibizumab 0.5 mg monthly Ranibizumab 0.5 mg as needed Bevacizumab 1.25 mg monthly Bevacizumab 1.25 mg as needed

89
CATT Study 24 month results Average change in visual acuity Ranibizumab 0.5 mg monthly – 8.8 letter increase Bevacizumab 1.25 mg monthly – 7.8 letter increase P = 0.21 As needed both inferior One or more serious adverse events Ranibizumab – 31.7% Bevacizumab – 39.9% P = 0.004

90
Lifestyle Changes Smoking Ultraviolet light Obesity

91
Vitreous Humor

92
80% of the volume of the eye Collagen, water, and hyaluronic acid Sites of attachment Base – around the ora serrata Retinal vessels Optic nerve Macula

93
The Aging Vitreous Destabilization Crosslinking of collagen fibers Free radical damage Decrease in network density of collagen fibers Shrinkage of vitreous Traction on points of strongest attachment

94
Vitreomacular Traction

95
Macular hole

96
Vitreomacular Traction Treatment Pars plana vitrectomy Posterior hyaloid release Risks Infection Retinal tears Bleeding But now…

97
Ocriplasmin Recombinant protease Activity against fibronectin and laminin Components of the vitreoretinal interface

98
Ocriplasmin MIVI-TRUST study group 652 patients Vision worse then 20/25 Vitreomacular traction on OCT Two arms Single intravitreal injection of ocriplasmin (125 μg) Single placebo injection Primary end point Resolution of vitreomacular adhesion Secondary end points Nonsurgical closure of a macular hole Change in best-corrected visual acuity
 Single placebo injection Primary end point Resolution of vitreomacular adhesion Secondary end points Nonsurgical closure of a macular hole Change in best-corrected visual acuity")
99
Ocriplasmin MIVI-TRUST study group Vitreomacular adhesion resolved – 28 days Ocriplasmin-injected eyes26.5%P<0.001 Placebo-injected eyes 10.1% Nonsurgical closure of macular holes – 28 days Ocriplasmin-injected eyes 40.6%P<0.001 Placebo-injected eyes 10.6% Improvement in best-corrected visual acuity by at least 3 lines – 6 months Ocriplasmin-injected eyes12.3%P=0.02 Placebo-injected eyes6.4%

100
Posterior Vitreous Detachment Common associations Age Increased axial length Other associations Aphakia Trauma Inflammatory disease

101
Posterior Vitreous Detachment Incidence Less then 10% before 50 years of age 63% after 70 years of age Symptoms Flashing lights New floaters Decreased vision (less common)
")
102
Posterior Vitreous Detachment Associated retinal tears

103
Posterior Vitreous Detachment Who has retinal tears? 15% of all patients with PVD 50-70% of all patients with PVD and vitreous hemorrhage 10-12% of patients PVD but no vitreous hemorrhage

104
Retinal Tears Treatment Observation Laser demarcation (barrier) Take home message – new flashes and floaters need seen that day
 Take home message – new flashes and floaters need seen that day")
105
Questions?

106
References Ranibizumab for neovascular age-related macular degeneration. Rosenfeld PJ, Brown DM, Heier JS, Boyer DS, Kaiser PK, Chung CY, Kim RY; MARINA Study Group. N Engl J Med. 2006 Oct 5;355(14):1419-31. Ranibizumab for neovascular age-related macular degeneration.Rosenfeld PJBrown DMHeier JSBoyer DSKaiser PKChung CYKim RYMARINA Study Group N Engl J Med. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T; ANCHOR Study Group. Ophthalmology. 2009 Jan;116(1):57-65.e5. doi: 10.1016/j.ophtha.2008.10.018. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study.Brown DMMichels MKaiser PKHeier JSSy JPIanchulev TANCHOR Study Group Ophthalmology. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two- year results. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, Toth C, Redford M, Ferris FL 3rd. Ophthalmology. 2012 Jul;119(7):1388-98. doi: 10.1016/j.ophtha.2012.03.053. Epub 2012 May 1. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two- year results.Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research GroupMartin DFMaguire MGFine SLYing GSJaffe GJGrunwald JEToth CRedford MFerris FL 3rd Ophthalmology. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol. 1985 Dec;103(12):1796-806. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group.
: Ranibizumab for neovascular age-related macular degeneration.Rosenfeld PJBrown DMHeier JSBoyer DSKaiser PKChung CYKim RYMARINA Study Group N Engl J Med. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study. Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T; ANCHOR Study Group. Ophthalmology Jan;116(1):57-65.e5. doi: /j.ophtha Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: Two-year results of the ANCHOR study.Brown DMMichels MKaiser PKHeier JSSy JPIanchulev TANCHOR Study Group Ophthalmology. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two- year results. Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Martin DF, Maguire MG, Fine SL, Ying GS, Jaffe GJ, Grunwald JE, Toth C, Redford M, Ferris FL 3rd. Ophthalmology Jul;119(7): doi: /j.ophtha Epub 2012 May 1. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two- year results.Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research GroupMartin DFMaguire MGFine SLYing GSJaffe GJGrunwald JEToth CRedford MFerris FL 3rd Ophthalmology. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol Dec;103(12): Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group..")
Similar presentations











 Waxman MD PhD>")




 Giovanni Caboto Club October 3, 2012>")








 occludes a branch of the central retinal vein Blockage causes bleeding from that branch Concerned about neovascularization.>")
