Download presentation
Presentation is loading. Please wait.

1
Cranial Trauma Gabriel C. Tender, MD Assistant Professor of Clinical Neurosurgery Louisiana State University in New Orleans

2
Patient #1 Walked in the ER after being hit in the head Initial GCS 14 – E4 V4 M6 (confused, but could maintain conversation) Started vomiting in the ER In CT scan he lost consciousness and GCS dropped to 9 – E2 V2 M5 (opening eyes to pain only, muttering sounds, localizing pain)
 Started vomiting in the ER In CT scan he lost consciousness and GCS dropped to 9 – E2 V2 M5 (opening eyes to pain only, muttering sounds, localizing pain)")
3
Patient #1

5
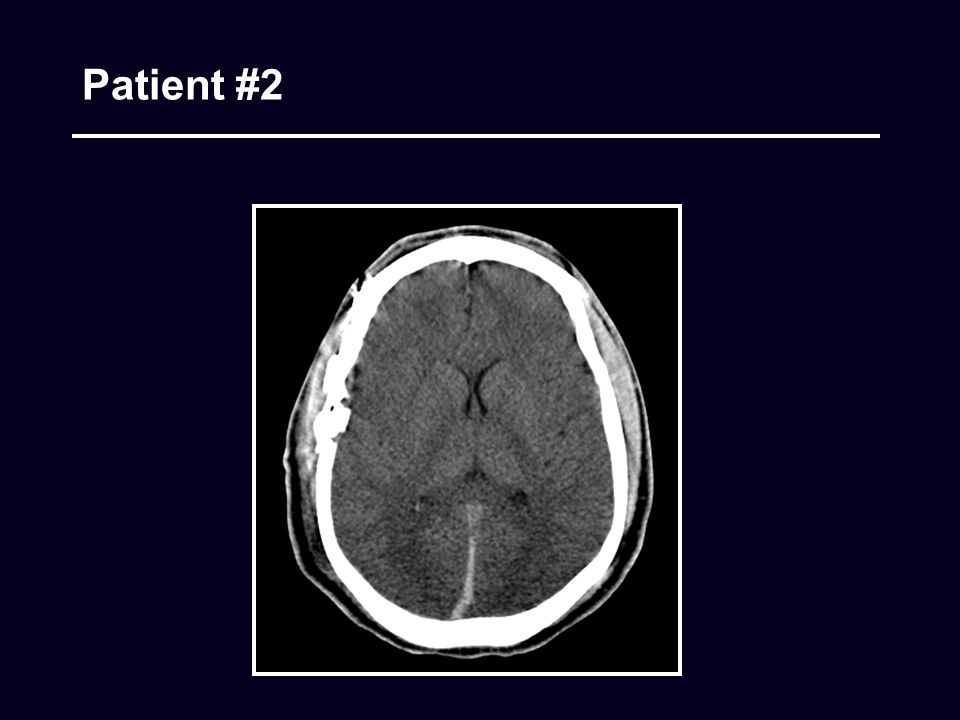
Patient #2 Involved in football accident GCS 10 – E2 V3 M5 Localize pain on R, not moving L side as much

6
Patient #2

8
Patient #3 Involved in high-speed MVA Sedated and intubated in the field Initial GCS 7 before sedation – E1 V1 M5

9
Patient #3

10
Cranial Trauma What is the most important factor on physical examination? Level of consciousness

11
Cranial Trauma GCS stratification (max: E4 V5 M6) 14-15 mild 9-12 moderate 3-8 severe NB: A confused patient cannot have a GCS of 15 (verbal is 4, so his GCS is 14 at the most)
 mild 9-12 moderate 3-8 severe NB: A confused patient cannot have a GCS of 15 (verbal is 4, so his GCS is 14 at the most)")
12
Mild Head Injury

13
Orders for minor/moderate CHI

14
Mild Head Injury

15
Moderate and Severe Head Injury What else is important (in comatose patients)? Lateralization Blown pupil Different reaction to pain (left vs. right) Babinski on one side only Rectal tone if a spinal cord injury is suspected
 Babinski on one side only Rectal tone if a spinal cord injury is suspected.")
16
General Initial Assessment

17
Exploratory Burrholes Indication (rare) Patient dying of rapid transtentorial herniation (ipsilateral blown pupil and/or contralateral paralysis or decerebration) not improved with mannitol and hyperventilation
 Patient dying of rapid transtentorial herniation (ipsilateral blown pupil and/or contralateral paralysis or decerebration) not improved with mannitol and hyperventilation")
18
Exploratory Burrholes

19
Head CT

20
CT evaluation – midline shift

21
CT evaluation – the basal cisterns

22
Head CT

24
Epidural Hematoma (EDH)
")
25
Acute Subdural Hematoma (SDH)
")
26
Parenchimal Lesions (Contusions)
")
27
Posterior Fossa Lesions

28
Cranial Fractures

29
ICP Monitoring

30
Insertion Point 13 cm from the nasion, or just behind the hair line 3 cm from the midline (usually on the right), or midpupillary line For ventriculostomies Aim for the ipsilateral epicanthus to hit the frontal horn, or go perpendicular to the bone (“straight down”) to hit the body of the lateral ventricle If you haven’t hit the ventricle by 5 cm, STOP! (you’re going in the wrong direction; pull out and choose a new direction)
.")
31
Ventriculostomy

35
ICP monitors

36
ICP monitors – Integra (Licox) Monitors both ICP and PaO2 Is more difficult to insert and maintain Has more drift
 Monitors both ICP and PaO2 Is more difficult to insert and maintain Has more drift")
37
ICP monitors – Integra (Licox) Tricks for insertion Use the drill that comes in the ICP monitor box, NOT the one in the cranial access kit When you drill, put the drill stop at about 1.3-1.5 cm (you have to go through the bone) Make sure you puncture the dura Don’t tighten the second knob until you’re done inserting the monitors Take all the three stylets out before inserting the Camino fiberoptic ICP monitor You will feel some resistance when you go through the dura; gently overcome it Do not insert the monitor past the black dot Once all three monitors are inserted, tighten the second knob
 Tricks for insertion Use the drill that comes in the ICP monitor box, NOT the one in the cranial access kit When you drill, put the drill stop at about cm (you have to go through the bone) Make sure you puncture the dura Don’t tighten the second knob until you’re done inserting the monitors Take all the three stylets out before inserting the Camino fiberoptic ICP monitor You will feel some resistance when you go through the dura; gently overcome it Do not insert the monitor past the black dot Once all three monitors are inserted, tighten the second knob")
38
ICP monitors – Codman Monitors ICP only Is easy to insert and maintain Has less drift

39
ICP monitors – Codman Tricks for insertion When you drill, put the drill stop at about 1.3-1.5 cm (you have to go through the bone) Make sure you puncture the dura Zero with the monitor tip in sterile water Do not insert the monitor past 5 cm (put a black mark at 5 cm from the tip)
 Make sure you puncture the dura Zero with the monitor tip in sterile water Do not insert the monitor past 5 cm (put a black mark at 5 cm from the tip)")
40
When to treat increased ICP?

41
Increased ICP Treatment - Hyperventilation

43
Increased ICP Treatment - Mannitol

44
No steroids for TBI!

45
Barbiturate Coma

46
ICP treatment

48
Nutrition

49
Posttraumatic Seizures

51
MCLNO Clinical Neurophysiology Laboratories Electroencephalography, Evoked Potentials, Polysomnography Medical DirectorElectrophysiologistsTechnologists Bruce Fisch, MDPiotr Olejniczak, MDTom Miller, REEGT Edward Mader, MD Lisa Keppard Jose Padin, MD Terri Ware

52
IVF Do NOT use D5; use ½ NS w/ 20 KCl Keep them euvolemic to dry (about 1cc/kg/hr) If brain edema is an issue, keep serum Na above 140 Mannitol and/or 3% saline (start at 15cc/hr, increase up to 50/hr) Check serum Na and osmol q6 hrs – do not exceed serum Na of 155 or serum osmol of 320
 If brain edema is an issue, keep serum Na above 140 Mannitol and/or 3% saline (start at 15cc/hr, increase up to 50/hr) Check serum Na and osmol q6 hrs – do not exceed serum Na of 155 or serum osmol of 320")
53
Admit Orders for Severe CHI Admit to ICU S/P TBI Cond: critical Vitals q1hr w/ neuro checks (if on Propofol, stop and check q4 hrs) Bedrest, HOB to 30*, loosen c-collar when patient sedated NPO IVF ½ NS w/ 20 K @ 80-100 cc/hr If significant brain edema, start 3%NS @ 15/hr, increase up to 50/hr (keep serum Na at 145-155, serum osmol 300-320) Vent No or low PEEP Keep PaCO2 at 30-35 (see hyperventilation above) Meds Propofol drip or Ativan 2-10mg iv q1hr for sedation or ICP>20 for>5’ MSO4 2-10 mg iv q1hr prn pain or ICP>20 for>5’ Mannitol 25g iv q4hrs prn ICP>20 for>5’ (hold if serum Na >155 or osmol>320) Cerebyx 1g iv now (loading dose), then 100mg q8 Pepcid 20mg iv bid Ancef 1g iv q8 if scalp wound or ICP monitor Nursing – per ICU routine Labs CBC, CMP, Dilantin level qAM Serum Na and osmol q6 if on 3% NaCl or Mannitol Repeat head CT in am (at least 2 CTs per patient, one on arrival and one next day) Call for problems
 Bedrest, HOB to 30*, loosen c-collar when patient sedated NPO IVF ½ NS w/ cc/hr If significant brain edema, start 15/hr, increase up to 50/hr (keep serum Na at , serum osmol ) Vent No or low PEEP Keep PaCO2 at (see hyperventilation above) Meds Propofol drip or Ativan 2-10mg iv q1hr for sedation or ICP>20 for>5’ MSO mg iv q1hr prn pain or ICP>20 for>5’ Mannitol 25g iv q4hrs prn ICP>20 for>5’ (hold if serum Na >155 or osmol>320) Cerebyx 1g iv now (loading dose), then 100mg q8 Pepcid 20mg iv bid Ancef 1g iv q8 if scalp wound or ICP monitor Nursing – per ICU routine Labs CBC, CMP, Dilantin level qAM Serum Na and osmol q6 if on 3% NaCl or Mannitol Repeat head CT in am (at least 2 CTs per patient, one on arrival and one next day) Call for problems")
54
Brain Death Exam in Adults Absence of brainstem reflexes Fixed pupils Absent corneal reflexes Absent oculovestibular reflex (cold water calorics) Absent oculocephalic reflex (not if C-spine not cleared) Absent gag and cough reflex No response to deep central pain Apnea test (last test to perform!) Vital signs Core temp > 32.2*C (90*F) SBP>90 mm Hg No drugs in the system!
 Absent oculocephalic reflex (not if C-spine not cleared) Absent gag and cough reflex No response to deep central pain Apnea test (last test to perform!) Vital signs Core temp > 32.2*C (90*F) SBP>90 mm Hg No drugs in the system!")
55
GSW to the Brain Immediate actions Control bleeding from scalp Shave scalp to identify entrance/exit wounds Assume ICP is elevated and treat Start antibiotics Obtain CT, rarely angio Patients with GCS 3 and no hematoma should usually not be operated upon

56
GSW to the Brain - Goals of Surgery

57
Summary On arrival, check Level of consciousness (GCS) Signs of lateralization Ipsilateral blown pupil Contralateral hemiplegia Unilateral Hoffman / Babinski CT scan Size of the hematoma / contusions Midline shift / effaced cisterns ICP monitor if GCS<8* For decreasing GCS, time is of essence
 Signs of lateralization Ipsilateral blown pupil Contralateral hemiplegia Unilateral Hoffman / Babinski CT scan Size of the hematoma / contusions Midline shift / effaced cisterns ICP monitor if GCS<8* For decreasing GCS, time is of essence")
Similar presentations

























, Dip. Diab.DCA, Dip. Software statistics PhD (physio) Mahatma gandhi medical college and.>")
>")
