Download presentation
Presentation is loading. Please wait.

1
Glasgow coma scale Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics PhD (physio) Mahatma gandhi medical college and research institute, puducherry, India
 Mahatma gandhi medical college and research institute, puducherry, India.")
2
Some history Teasdale and Jennett in 1974 the Glasgow Coma Scale or GCS is a neurological scale that aims to give a reliable, objective way of recording the conscious state of a person for initial as well as subsequent assessment.

3
First use !! as a method of describing states of impairment within the consciousness continuum a quick, practical standardized system for assessing the degree of consciousness in the critically ill and for predicting the duration and ultimate outcome of coma, primarily in patients with head injuries

4
Original authors Changing level of consciousness – development of complications Depth of coma ---for ultimate recovery which can be expected Assessment at 6 h following head trauma.- influence of alcohol, drugs, hypoxia gone

6
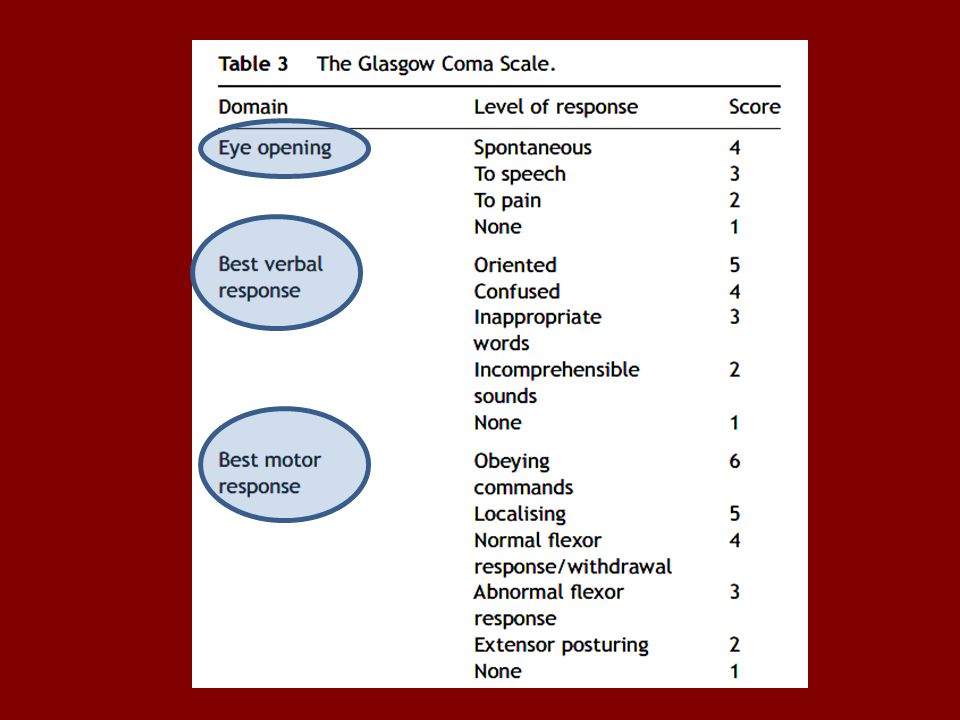
The scale involves eye opening, verbal response, and motor response, all of which are evaluated independently according to a rank order that indicates the level of consciousness and degree of dysfunction

7
Electronic Voting Machine E – 4 V – 5 M- 6

8
The sum of the numeric values for each parameter can also be used as an overall objective measurement. E + V + M 15 indicative of no impairment, 3 compatible with brain death, and 7 usually accepted as a state of coma.

9
EVM – separate analyses

13
Localize

14
Withdrawal

15
Flexor

16
Extensor

17
Clinical uses. The test score can also function as an indicator for certain diagnostic tests or treatments, such as the need for a computed tomography scan, intracranial pressure monitoring, and intubation. The scale has a high degree of consistency even when used by staff with varied experience.

18
Clinical uses The results may be plotted on a graph to provide a visual representation of the improvement, stability, or deterioration of a patient's level of consciousness, which is crucial to predicting the eventual outcome of coma. various medical conditions including drug overdose, infection, spontaneous intracranial bleeding, seizures and hepatic encephalopathy

19
v Time

20
Head Injury Classification Severe Head Injury----GCS score of 8 or less Moderate Head Injury----GCS score of 9 to 12 Mild Head Injury----GCS score of 13 to 15

21
Clinical uses To facilitate understanding, clear description and communication between clinicians For research purposes

22
Prognosis The GCS motor score 2 weeks after injury was statistically significantly associated with the 12-month functional outcome in TBI survivors. Motor response was the most useful predictor among the GCS components with respect to the long-term functional outcome in patients with severe TBI. -- Controversial !!

23
In stroke !! The GCS verbal component may be misleading in acute stroke: a focal neurological deficit leading to dysphasia could affect the score, independently of level of consciousness.

24
Which will confuse GCS ?? Ocular trauma, Cranial nerve injuries, edema of tongue Facial trauma Injuries (spinal cord, peripheral nerves, extremities) Pain, Intoxication (alcohol, drugs) Medications (anaesthetics, sedatives) Dementia, Psychiatric diseases Developmental impairments Intubation, tracheostomy, Laryngectomy Mutism Hearing impairments
 Pain, Intoxication (alcohol, drugs) Medications (anaesthetics, sedatives) Dementia, Psychiatric diseases Developmental impairments Intubation, tracheostomy, Laryngectomy Mutism Hearing impairments.")
25
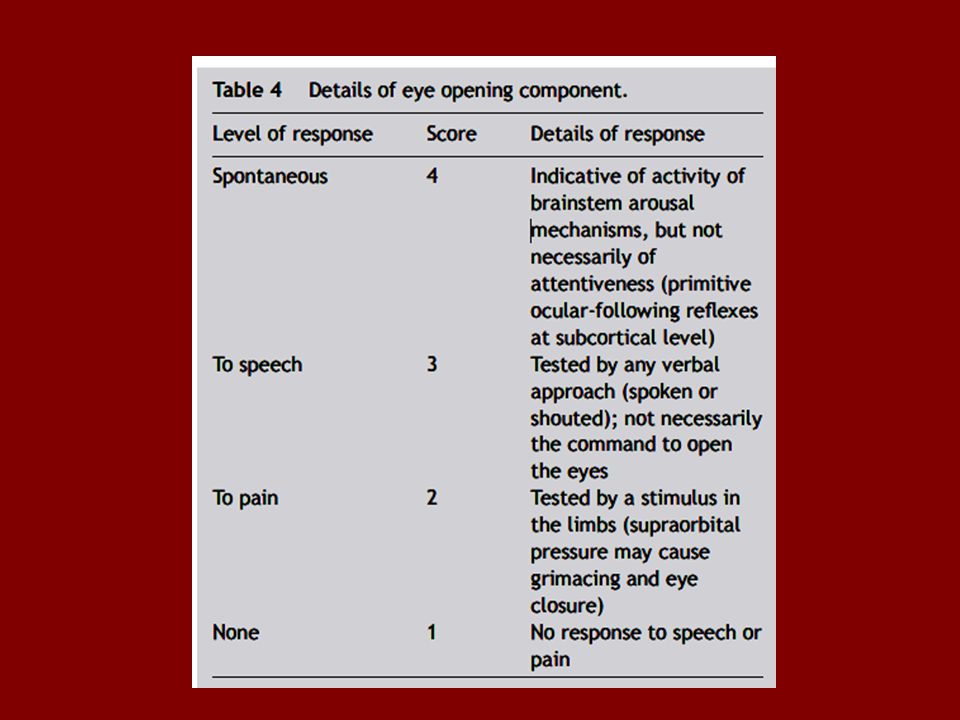
Detailed breakdown of GCS components Eyes GCS 0f 3- 4 – brain stem may be ok but 2 or less ?? Vegetative state can have rarely spontaneous reflexive eye opening !!!

26
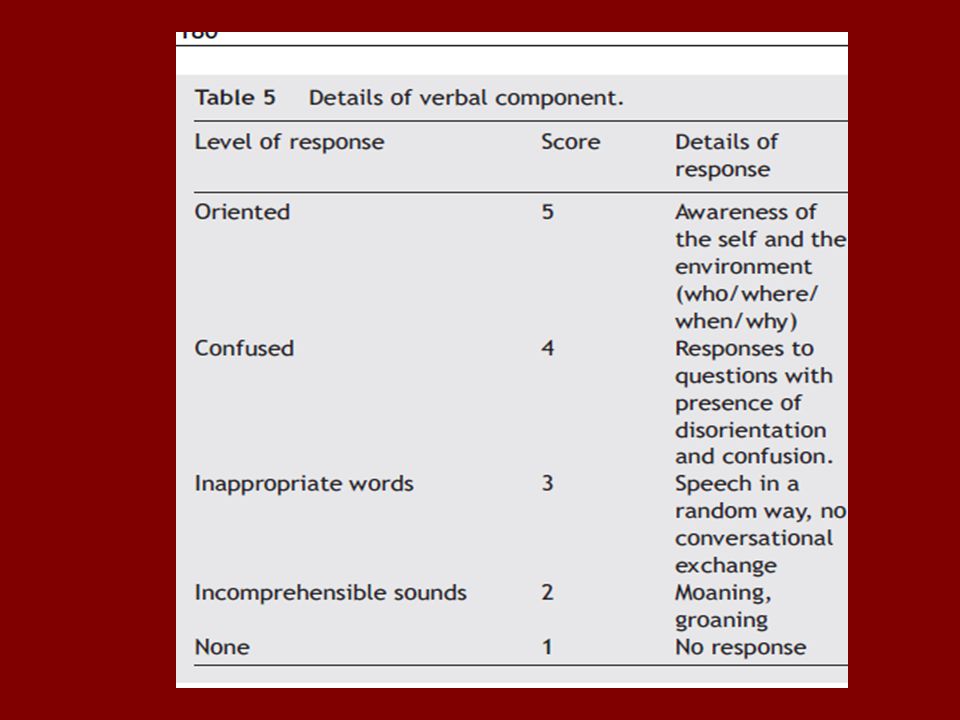
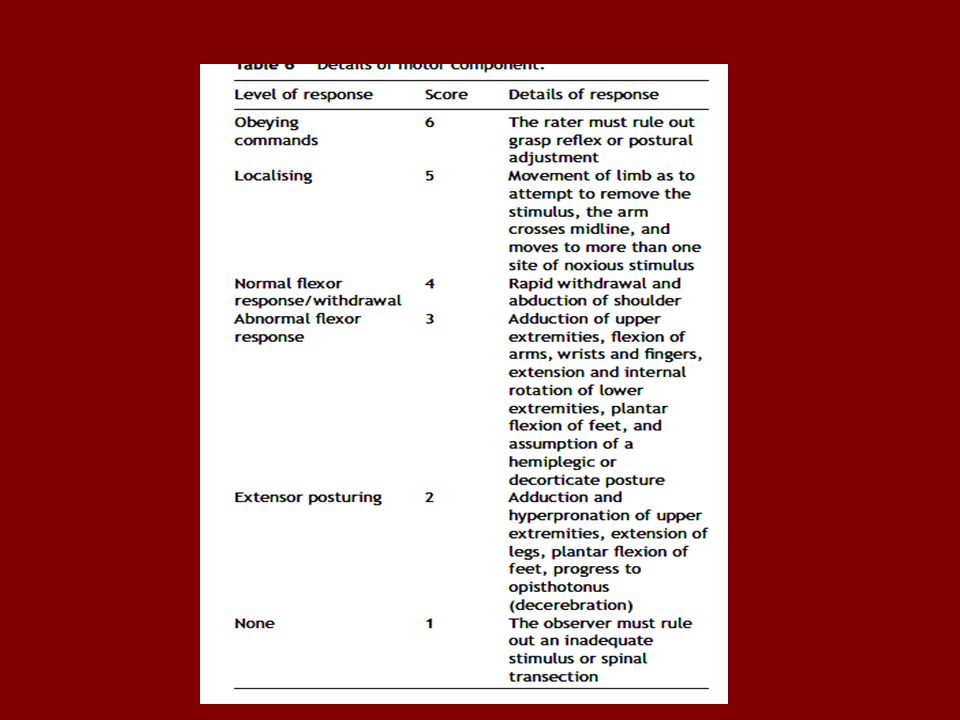
Verbal Presence of speech implies a high level of integration in the nervous system Motor scores of 6, 5 and 4 imply the presence of cerebral function and the ability to react appropriately to a noxious stimulus. 2 or 3 – may be brainstem ??

27
Children – verbal response

28
Compare with other scores

29
FOUR score The FOUR (Full Outline of UnResponsiveness) score, not surprisingly, has four components, each of which has 4 as the maximal grade. Eye, motor, brainstem reflexes, respiration

30
AVPU score The GCS was compared to the AVPU Alert, responds to Verbal stimuli, responds to Painful stimuli, Unresponsive score and median GCS scores of 15, 13, 8 and 3 corresponded to AVP and U respectively A, V, P, U 15, 13, 8, 3

31
WFNS GCS motor deficit I 15 absent II 14- 13 absent III 14 – 13 present IV 12 -7 present or absent V 6 -3 present or absent

32
Conclusions All the advantages But Concerns have been raised about the potential for misleading levels of precision engendered by the use of the GCS, and the use of simpler scales suggested.

33
Thank you all

Similar presentations


>")
















 injury or illness Mental status : clinical state.>")