Download presentation
Presentation is loading. Please wait.

1
Congenital Hypothyroidism 先天性甲状腺功能减低症 Congenital Hypothyroidism 先天性甲状腺功能减低症 Xue Fan Gu, MD, PhD Xinhua Hospital Shanghai Jiao Tong University School of Medicine

2
Incidence Incidence Thyroid hormone deficiency may: or acquired Congenital:most cases are hypoplasia or aplasia of the thyroid gland World: 1:3 000 ~ 5 000 1:3 200 China: 1:3 200

3
8th gestational weeks: synthesis of thyroglobulin 10~12th gestational weeks: pitutary gland begins to secrete TSH,thyroid gland synthesis of T3 、 T4 30th gestational weeks: hypothalamic- pitutary-thyroid axis is functioning and independent of the maternal axis Thyroid Ontogenesis Thyroid Ontogenesis

4
After delivery, TSH rapidly rise reaching 60~80 uU/ml levels, and then slowly decline over the next few days(5~7d) to <5 uU/ml levels
 to <5 uU/ml levels")
5
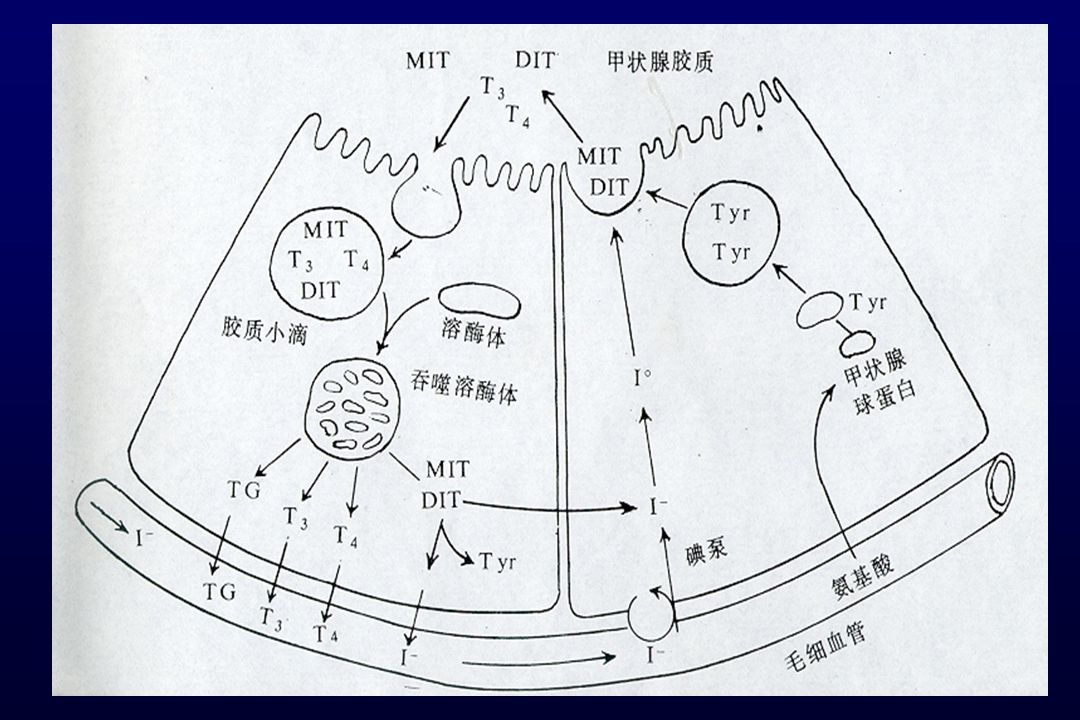
Thyroid hormone synthesis and metabolism The thyroid follicle is stimulated by TSH by increase with TSH receptor Iodine from the circulation is concentrated and rapidly oxidized by peroxidase to iodine Iodine incorporated into tyrosyl residures on thyroglobuline Iodothyrosines are couple an ether linkage to form T4 and T3

7
T3 and T4 Metabolic potency of T3 is 3~4 times that of T4. Only 20% of circulating T3 is secreted by the thyroid T3, T4 in circulation Binding form : 70 % with TBG , other with Alb. Free form : T4 0.03%, T3 0.3%

8
TRH TSH - Hypothalamus Anterior pituitary gland Thyroid gland rT3 T3 T4 Hypothylamic-pitutary-thyroid feedback regulation

9
Physiological of thyroid hormones Increase oxygen consumption Stimulate protein synthesis Influence growth and differentiation Affect carbohydrate, lipid and vitamine metabolism

10
Etiology The cause may be sporadic or familial, goitrous or nongoitrousThe cause may be sporadic or familial, goitrous or nongoitrous Defective embryogenesis 75%Defective embryogenesis 75% Agenesis, dysgenesis, ectopia Agenesis, dysgenesis, ectopia DyshormonogenesisDyshormonogenesis Pit-1, TSH, TSHR, TTF-I, TTF-II, Pax 8, TG, TPO defect, etc. Pit-1, TSH, TSHR, TTF-I, TTF-II, Pax 8, TG, TPO defect, etc. Iodide transport defect, organification defect, coupling defect, iodothyrosine deiodinase defect, inability of tissueses to convert T4 to T3 Iodide transport defect, organification defect, coupling defect, iodothyrosine deiodinase defect, inability of tissueses to convert T4 to T3 Deficiency or excess of iodine

11
Transient Hypothyroidism Premature Maternal medications (propylthiouracil,methimazol) Maternal antibody Iodine deficiency hypothyroidism in iodine deficiency area
 Maternal antibody Iodine deficiency hypothyroidism in iodine deficiency area")
12
Other Causes Pitutary/hypothalamis hypothyroidismPitutary/hypothalamis hypothyroidism Rare , <5 %, measurement of TSH levels fail to revel patient with pitutary-hypothalamic hypothyroidism, since they have low TSH

13
Classification According To TSH Level TSH level rise Primary hypothyroidism Transient hypothyroidism TSH level in normal Pitutary/hypothalamis hypothyroidism low TBG

14
Clinical Findings In Newborns and Infants Absent symptom during the first few weeks of life A few have birth weight>3.5kg prolongation of physiological icterus,constipation, hoarse cry, feeding or sucking difficulties

15
Progress Manifestation Pulse is slow, heart murnures, cardiomegaly,hypothermia, hypotonia, enlarged tongue, skin cold and dry, umbilical hernia, hair is dry Mental retardation growth stunted

16
甲低特殊外表 8y

17
Pituitary- hypothalamis Hypothyroidism caused by Pituitary- hypothalamis Without symptom in neonatal period May be with other pituitaty hormone deficiency GH deficiency : short stature ACTH deficiency : hypoglycemia ADH deficiency : diabetes incipidus

18
mu/L TSH in neonatal screening programs: <10~15 mu/L Normal range for neonate T4 84-210 nmol/l(6.5-16.3ug/dl) FT4 12-28 pmol/l(0.9-2.2ng/dl) TSH 1.7-9.1 mu/L(1.7-9.1 uU/ml) TSH 1.7-9.1 mu/L(1.7-9.1 uU/ml) Laboratory findings
 FT pmol/l( ng/dl) TSH mu/L( uU/ml) TSH mu/L( uU/ml) Laboratory findings")
19
Scintigraphy 99mTc 、 123 I scintigraphy B ultrasound examination X ray: retardation of skeletal maturation (bone age)
")
20
Treatment Principal Give thyroxine as early as possible TSH and FT4 should be monitored and maintained in the normal range Confirmation of diagnosis may be necessary for some infant to rule out the possibility of transient hypothyroidism at 2~3 years old

21
Dose of thyroxine Dose of thyroxine ( L-T4) ────────────────────── Age μg/day ug/kg/day ────────────────────── 0~6m 25~50 8.5~10 6~12m 50~100 5~8 1~5y 75~100 5~6 6~12y 100~150 4~5 12y to adult 100~200 2~3 ──────────────────────
 ────────────────────── Age μg/day ug/kg/day ────────────────────── 0~6m 25~50 8.5~10 6~12m 50~100 5~8 1~5y 75~100 5~6 6~12y 100~150 4~5 12y to adult 100~200 2~3 ──────────────────────")
22
CH (4y) before treatment after one year treatment
 before treatment after one year treatment")
23
Flow Chart of Neonatal Screening for CH TSH of retesteted sample > Cut off point Recall of neonate retested TSH level> Cut off point Serum FT3,FT4,TSH X-ray of knee FT4 TSH delayed BA FT4 normal , TSH normal BA CH Hyperthyrotropinemia

Similar presentations









 Triiodothyronine (T3) T4 and T3 regulate body metabolism.>")










