Download presentation
Presentation is loading. Please wait.

2
علایم بالینی و درمان هیپوتیروییدی مادرزادی ارایه دهنده: دکتر مجید ولی زاده دکتر مجید ولی زاده

3
References: Up to date 2009 (17.3) Up to date 2009 (17.3).
 Up to date 2009 (17.3).")
4
Thyroid Embryology Derived from endodermal tissue at base of tongue Embryonal remnants form Thyroglossal duct; pyramidal lobe; lingual thyroid Fuse with C-cells (neural crest origin), derived from the the 5th branchial arch C-cells scattered through posterior/superior lobes
, derived from the the 5th branchial arch C-cells scattered through posterior/superior lobes")
5
Major causes of congenital hypothyroidism, approximate frequency Thyroid dysgenesis - ectopia, aplasia, or hypoplasia (1:4500) Thyroid dysgenesis - ectopia, aplasia, or hypoplasia (1:4500) Inborn errors of thyroxine synthesis (dyshormonogeneses) (1:30,000) Inborn errors of thyroxine synthesis (dyshormonogeneses) (1:30,000) Maternal antibody-mediated hypothyroidism (1:25,000-1:100,000) Maternal antibody-mediated hypothyroidism (1:25,000-1:100,000) Central hypothyroidism (1:25,000-1:100,000) Central hypothyroidism (1:25,000-1:100,000) Transient hypothyroidism (1:100 Europe) Transient hypothyroidism (1:100 Europe)
 Thyroid dysgenesis - ectopia, aplasia, or hypoplasia (1:4500) Inborn errors of thyroxine synthesis (dyshormonogeneses) (1:30,000) Inborn errors of thyroxine synthesis (dyshormonogeneses) (1:30,000) Maternal antibody-mediated hypothyroidism (1:25,000-1:100,000) Maternal antibody-mediated hypothyroidism (1:25,000-1:100,000) Central hypothyroidism (1:25,000-1:100,000) Central hypothyroidism (1:25,000-1:100,000) Transient hypothyroidism (1:100 Europe) Transient hypothyroidism (1:100 Europe)")
6
Lingual thyroid

8
CLINICAL MANIFESTATIONS More than 95 percent asymptomatic More than 95 percent asymptomatic –umbilical cord serum T4 concentrations are about 25 to 50 % –inadequate, functioning thyroid tissue

9
Figure 15-7. Brain neurologic development relative to thyroid function in the rat and human. TH, thyroid hormones; dpc, days postconception; dpn, days postnatal. (From Porterfield and Hendrich, with permission.)
.")
10
Clinical manifestations: Birth length and weight Birth length and weight head circumference head circumference other congenital anomalies ↑ other congenital anomalies ↑

11
CLINICAL MANIFESTATIONS Lethargy Lethargy slow movement slow movement hoarse cry hoarse cry feeding problems feeding problems constipation constipation macroglossia macroglossia umbilical hernia umbilical hernia large fontanels large fontanels hypotonia hypotonia dry skin dry skin hypothermia hypothermia prolonged jaundice prolonged jaundice A few with thyroid dyshormonogenesis : a palpable goiter A few with thyroid dyshormonogenesis : a palpable goiter

20
Figure 15-12. Ten year old female with severe 1° hypothyroidism due to primary myxedema before (A) and after (B) treatment. Presenting complaint was poor growth. Note the dull facies, relative obesity and immature body proportions prior to treatment. At age 10 years she had not lost a single deciduous tooth. After treatment was initiated (indicated by the arrow in Panel C), she lost 6 teeth in 10 months and had striking catch up growth. Bone age was 5 years at a chronologic age of 10 years. TSH receptor blocking antibodies were negative.
 and after (B) treatment. Presenting complaint was poor growth. Note the dull facies, relative obesity and immature body proportions prior to treatment. At age 10 years she had not lost a single deciduous tooth. After treatment was initiated (indicated by the arrow in Panel C), she lost 6 teeth in 10 months and had striking catch up growth. Bone age was 5 years at a chronologic age of 10 years. TSH receptor blocking antibodies were negative..")
22
Figure 15-4. Postnatal TSH, T4, T3, and rT3 secretion in the full-term and premature infant in the first week of life (modified from Fisher DA: Disorders of the thyroid in the newborn and infant. In: Sperling M (ed) Pediatric Endocrinology, WB Saunders Co., Philadelphia, 51, 1996).
 Pediatric Endocrinology, WB Saunders Co., Philadelphia, 51, 1996)..")
24
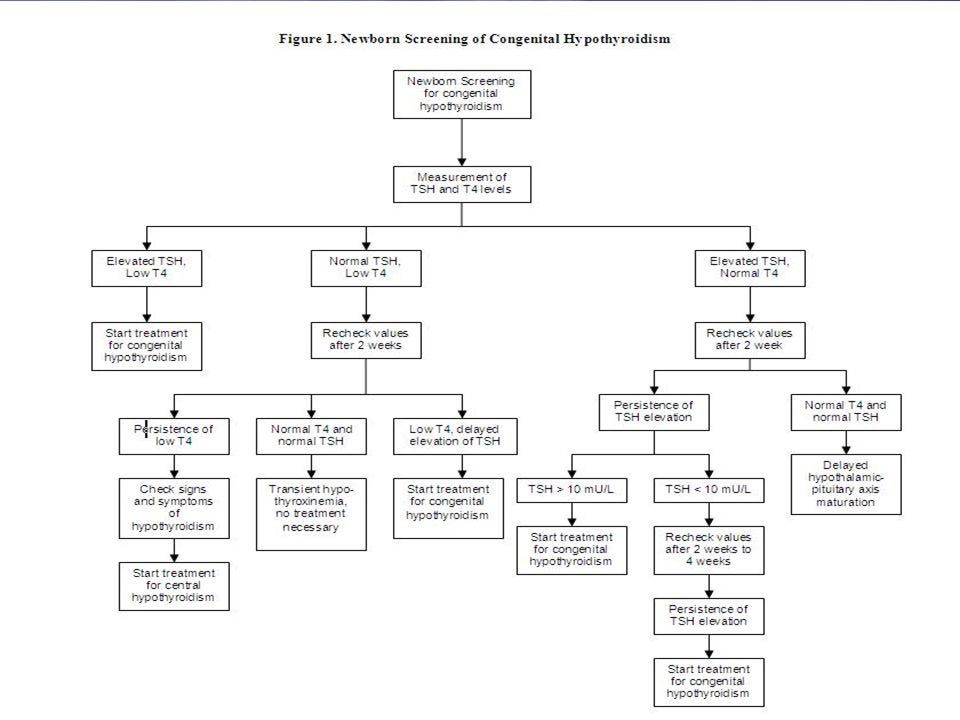
Low T4 and Elevated TSH Values Low T4 + TSH > 40 :is considered to have primary hypothyroidism (Iran: TSH> 5 ) Low T4 + TSH > 40 :is considered to have primary hypothyroidism (Iran: TSH> 5 ) examination (immediately ) + confirmatory serum testing to verify the diagnosis. examination (immediately ) + confirmatory serum testing to verify the diagnosis. screening TSH concentration is only slightly elevated but < 40 mU/L, another filter-paper specimen should be obtained for a second newborn screening. screening TSH concentration is only slightly elevated but < 40 mU/L, another filter-paper specimen should be obtained for a second newborn screening.
 + confirmatory serum testing to verify the diagnosis. screening TSH concentration is only slightly elevated but < 40 mU/L, another filter-paper specimen should be obtained for a second newborn screening. screening TSH concentration is only slightly elevated but < 40 mU/L, another filter-paper specimen should be obtained for a second newborn screening..")
25
Low T4 + high TSH 10% Hypothyroids ( TSH : 20-40) 10% Hypothyroids ( TSH : 20-40) It is important that age appropriate normative values be used. It is important that age appropriate normative values be used. Range for TSH for the most common time of TSH re-evaluation (between 2 and 6 weeks of age) is 1.7 to 9.1 mU/L. Range for TSH for the most common time of TSH re-evaluation (between 2 and 6 weeks of age) is 1.7 to 9.1 mU/L.
 is 1.7 to 9.1 mU/L. Range for TSH for the most common time of TSH re-evaluation (between 2 and 6 weeks of age) is 1.7 to 9.1 mU/L..")
26
Normal T4 and Elevated TSH Values ( Hyperthyrotropinemia) Etiology : Etiology : 1) transient or permanent thyroid abnormality 2) delayed maturation of the hypothalamic- pituitary axis. 3) Inactivation mutations in the TSH-R cause compensated, mild (subclinical) primary hypothyroidism in the neonatal period.
 Inactivation mutations in the TSH-R cause compensated, mild (subclinical) primary hypothyroidism in the neonatal period..")
27
There is controversy regarding the need for TH therapy in this setting.

28
High TSH + normal T4 Most physicians would consider a persistent basal TSH concentration higher than 10 mU/L (after the first 2 weeks of age) to be abnormal. Most physicians would consider a persistent basal TSH concentration higher than 10 mU/L (after the first 2 weeks of age) to be abnormal. If such infants are not treated, measurement of FT4 and TSH should be repeated in 2 and 4 weeks, and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized. If such infants are not treated, measurement of FT4 and TSH should be repeated in 2 and 4 weeks, and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized.
 to be abnormal. If such infants are not treated, measurement of FT4 and TSH should be repeated in 2 and 4 weeks, and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized. If such infants are not treated, measurement of FT4 and TSH should be repeated in 2 and 4 weeks, and treatment should be initiated promptly if the FT4 and TSH concentrations have not normalized..")
29
High normal TSH The management of infants with TSH elevations between 6 and 10 mU/L that persist after the first month of life is even more controversial. The management of infants with TSH elevations between 6 and 10 mU/L that persist after the first month of life is even more controversial. A TSH range of 1.7 to 9.1 mU/L has been reported for children 2 to 20 weeks of age A TSH range of 1.7 to 9.1 mU/L has been reported for children 2 to 20 weeks of age if a decision is made to treat such children, a trial off therapy at 3 years of age should be performed. if a decision is made to treat such children, a trial off therapy at 3 years of age should be performed.

30
Low T4 and Normal TSH Values 2 SDs below the mean for the reference range for age, usually < 10 µg/dL in the newborn infant 2 SDs below the mean for the reference range for age, usually < 10 µg/dL in the newborn infant 1) Hypothalamic immaturity 2) during illness 3) protein-binding disturbances such as TBG deficiency(1 in 5000) 4) central hypothyroidism (l in 25 000 to l in 50 000 newborn infants) 5) primary hypothyroidism and delayed TSH elevation (l in 100 000 newborn infants). Transient hypothyroxinemia is seen to some extent in many preterm infants Transient hypothyroxinemia is seen to some extent in many preterm infants

31
Figure 15-4. Postnatal TSH, T4, T3, and rT3 secretion in the full-term and premature infant in the first week of life (modified from Fisher DA: Disorders of the thyroid in the newborn and infant. In: Sperling M (ed) Pediatric Endocrinology, WB Saunders Co., Philadelphia, 51, 1996).
 Pediatric Endocrinology, WB Saunders Co., Philadelphia, 51, 1996)..")
32
Hypothyroxinemia Take no further action, to follow-up with serial filter-paper screening tests until the T4 value becomes normal, or to request second blood sample for measurement of FT4 and TSH concentration. Take no further action, to follow-up with serial filter-paper screening tests until the T4 value becomes normal, or to request second blood sample for measurement of FT4 and TSH concentration. Most infants with low T4 and normal TSH have normal FT4 values, and subsequent thyroid function test results are normal Most infants with low T4 and normal TSH have normal FT4 values, and subsequent thyroid function test results are normal

33
Transient TSH Elevation Intrauterine exposure to maternal anti thyroid drugs, maternal TRBAbs Intrauterine exposure to maternal anti thyroid drugs, maternal TRBAbs Heterozygous thyroid oxidase 2 deficiency Heterozygous thyroid oxidase 2 deficiency Germ-line mutations in the TSH-R, endemic Germ-line mutations in the TSH-R, endemic Iodine deficiency Iodine deficiency Prenatal or postnatal exposure to excess iodides ( povidone iodine, iodinated contrast materials) Prenatal or postnatal exposure to excess iodides ( povidone iodine, iodinated contrast materials)
 Prenatal or postnatal exposure to excess iodides ( povidone iodine, iodinated contrast materials)")
34
CLINICAL MANAGEMENT OF NEWBORN INFANTS WITH LOW T4 AND ELEVATED TSH VALUES Infants with low T4 and elevated TSH concentrations have CH until proven otherwise. Infants with low T4 and elevated TSH concentrations have CH until proven otherwise. 1) Consultation with a endocrinologist is recommended to facilitate diagnostic evaluation and optimal management.
 Consultation with a endocrinologist is recommended to facilitate diagnostic evaluation and optimal management..")
35
Clinical management... 2) A complete history, including prenatal thyroid status (maternal drugs and medications) and family history should be obtained, and physical examination should be performed. 3) Serum should be obtained for confirmatory measurements of TSH and FT4.
 A complete history, including prenatal thyroid status (maternal drugs and medications) and family history should be obtained, and physical examination should be performed. 3) Serum should be obtained for confirmatory measurements of TSH and FT4..")
36
Clinical management... 4) Education of parents by trained personnel using booklets or visual aids is highly desirable. 5) Optional diagnostic studies include - -thyroid ultrasonography -iodine 123 ( 123 I) -iodine 123 ( 123 I) - sodium technetium 99m pertechnetate (99mTc) thyroid uptake -and/or scan to identify functional thyroid tissue.
 Education of parents by trained personnel using booklets or visual aids is highly desirable. 5) Optional diagnostic studies include - -thyroid ultrasonography -iodine 123 ( 123 I) -iodine 123 ( 123 I) - sodium technetium 99m pertechnetate (99mTc) thyroid uptake -and/or scan to identify functional thyroid tissue..")
38
Treatment Treatment Should Begin As Soon As Possible, Preferably Within The First Two Weeks of Life Treatment Should Begin As Soon As Possible, Preferably Within The First Two Weeks of Life

39
Treatment The Goal Of Treatment To Ensure Normal Growth &Development To Ensure Normal Growth &Development T4 10 To 16 µg/dl TSH Around 1 mIu/L

40
Treatment : The goal of therapy is to normalize T4 within 2 weeks and TSH within 1 month. The goal of therapy is to normalize T4 within 2 weeks and TSH within 1 month. An initial dosage of 10 to 15 g/kg of L-T4 (depending on the severity of the initial hypothyroidism) An initial dosage of 10 to 15 g/kg of L-T4 (depending on the severity of the initial hypothyroidism) Administration of L-T4 is the treatment of choice. Administration of L-T4 is the treatment of choice.
 An initial dosage of 10 to 15 g/kg of L-T4 (depending on the severity of the initial hypothyroidism) Administration of L-T4 is the treatment of choice. Administration of L-T4 is the treatment of choice..")
41
Treatment : The pill should be crushed and suspended in a few milliliters of formula, breast milk, or water. The pill should be crushed and suspended in a few milliliters of formula, breast milk, or water. Only T4 tablets should be used Only T4 tablets should be used T4 is expected to increase to more than 10 µg/dL T4 is expected to increase to more than 10 µg/dL FT4 is expected to increase to more than 2 ng/dL by 2weeks after initiating therapy FT4 is expected to increase to more than 2 ng/dL by 2weeks after initiating therapy TSH should normalize by 1 month. TSH should normalize by 1 month.

42
Treatment : The L-T4 dose should be adjusted according to the infant’s clinical response and serum FT4 and TSH concentrations. The L-T4 dose should be adjusted according to the infant’s clinical response and serum FT4 and TSH concentrations. During therapy, the serum total T4 or FT4 should and might be in the upper half of the reference range (target values depend on the assay method used [T4: 10–16 g/dL (130–206 nmol/L); FT4: 1.4 –2.3 ng/dL (18–30 pmol/L)]) during the first 3 years of life with a low normal serum TSH. During therapy, the serum total T4 or FT4 should and might be in the upper half of the reference range (target values depend on the assay method used [T4: 10–16 g/dL (130–206 nmol/L); FT4: 1.4 –2.3 ng/dL (18–30 pmol/L)]) during the first 3 years of life with a low normal serum TSH. The latter may sometimes be delayed because of relative pituitary resistance. The latter may sometimes be delayed because of relative pituitary resistance.
; FT4: 1.4 –2.3 ng/dL (18–30 pmol/L)]) during the first 3 years of life with a low normal serum TSH. During therapy, the serum total T4 or FT4 should and might be in the upper half of the reference range (target values depend on the assay method used [T4: 10–16 g/dL (130–206 nmol/L); FT4: 1.4 –2.3 ng/dL (18–30 pmol/L)]) during the first 3 years of life with a low normal serum TSH. The latter may sometimes be delayed because of relative pituitary resistance. The latter may sometimes be delayed because of relative pituitary resistance..")
43
Between 1 and 5 days of life, the normal range for serum total T4 concentrations is about 10 to 22 µg/dL Between 1 and 5 days of life, the normal range for serum total T4 concentrations is about 10 to 22 µg/dL Between 1 and 4 weeks of life, the normal range for serum total T4 concentrations is 7 to 16 µg/dL Between 1 and 4 weeks of life, the normal range for serum total T4 concentrations is 7 to 16 µg/dL

44
Delay in normalization of TSH: Normal or increased serum ( → or ↑ ) T4 and an inappropriately high TSH concentration, the T4 value is used to titrate the dose. Normal or increased serum ( → or ↑ ) T4 and an inappropriately high TSH concentration, the T4 value is used to titrate the dose. Nonadherence to the treatment is the most common cause of persistent TSH elevation and should be excluded. Nonadherence to the treatment is the most common cause of persistent TSH elevation and should be excluded.
 T4 and an inappropriately high TSH concentration, the T4 value is used to titrate the dose. Nonadherence to the treatment is the most common cause of persistent TSH elevation and should be excluded. Nonadherence to the treatment is the most common cause of persistent TSH elevation and should be excluded..")
45
Target of treatment: TSH levels should be maintained between 0.5 and 2.0 mU/L during the first 3 years of life TSH levels should be maintained between 0.5 and 2.0 mU/L during the first 3 years of life During TH therapy, 4 or more episodes of insufficiently suppressed TSH (5 mU/L) after the age of 6 months were the most important variables associated with school delay During TH therapy, 4 or more episodes of insufficiently suppressed TSH (5 mU/L) after the age of 6 months were the most important variables associated with school delay
 after the age of 6 months were the most important variables associated with school delay During TH therapy, 4 or more episodes of insufficiently suppressed TSH (5 mU/L) after the age of 6 months were the most important variables associated with school delay")
49
DIAGNOSTIC STUDIES venipuncture to confirm venipuncture to confirm If the diagnosis of hypothyroidism is confirmed If the diagnosis of hypothyroidism is confirmed –thyroid radionuclide uptake and imaging –Ultrasonography –serum thyroglobulin assay –thyroid autoantibodies –urinary iodine excretion These tests usually do not alter treatment

50
Recommended follow-up At 2 and 4 weeks after the initiation of T4 treatment At 2 and 4 weeks after the initiation of T4 treatment Every 1 to 2 months during the first year of life Every 1 to 2 months during the first year of life Every 2 to 3 months between 1 and 3 years of age Every 2 to 3 months between 1 and 3 years of age Every 3 to 12 months thereafter until growth is complete Every 3 to 12 months thereafter until growth is complete Two weeks after any change in dosage

51
Other neurologic sequelae gross and fine motor incoordination gross and fine motor incoordination – ataxia, – increased or decreased muscle tone – short attention span – speech defects – strabismus Studies before the initiation of newborn screening reported that up to 20 percent of children had sensorineural hearing loss Studies before the initiation of newborn screening reported that up to 20 percent of children had sensorineural hearing loss

53
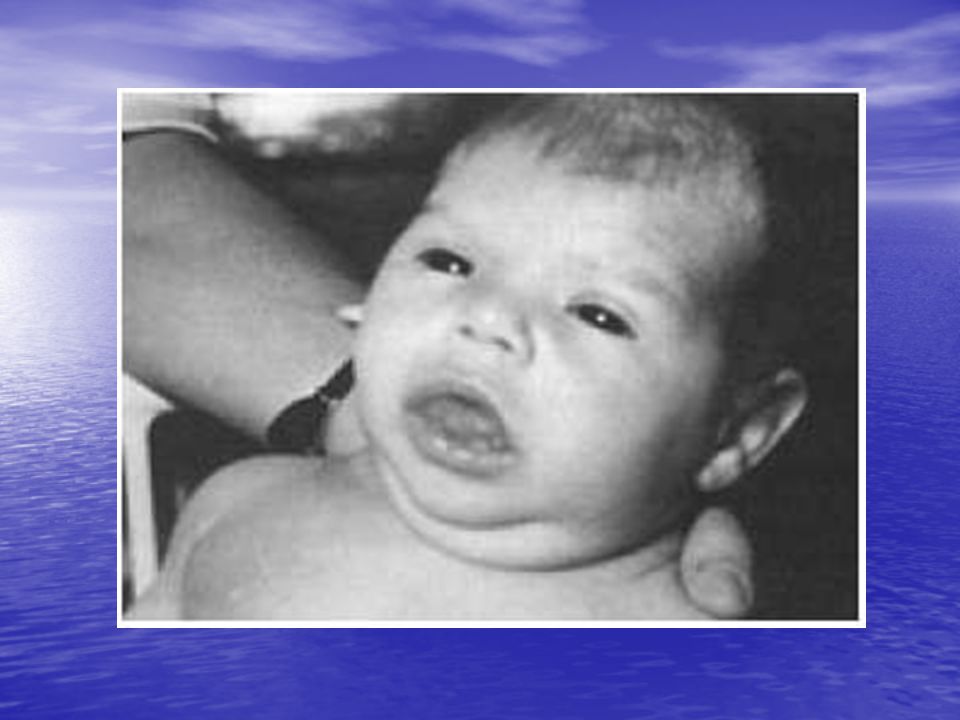
Figure 15-11. (Left panel) Infant with severe, untreated congenital hypothyroidism diagnosed prior to the advent of newborn screening. (Right panel) Infant with congenital hypothyroidism identified through newborn screening. Note the striking difference in the severity of the clinical features.
 Infant with severe, untreated congenital hypothyroidism diagnosed prior to the advent of newborn screening. (Right panel) Infant with congenital hypothyroidism identified through newborn screening. Note the striking difference in the severity of the clinical features..")
54
PROGNOSIS If treated at appropriate time In general, these infants grow and develop normally If treated at appropriate time In general, these infants grow and develop normally

55
Untreated CH Patients at Risk for Severe Mental Retardation Klein et al, J Pediatr 81:912-915, 1972

56
IQ of CH patients is normal if treatment early and adequate NECHC. Lancet 2:1095-1098, 1981

57
But small differences in T4 dose have enormous impact on IQ MDI- Mental Development Index T4 dose Bongers-Shokking JJ et al, J Pediatr 136:292-297,2000 *

59
Thyroid hormones effects Growth & development ( skeletal & nervous system) Growth & development ( skeletal & nervous system) General metabolism ( ↑ oxidation) General metabolism ( ↑ oxidation) Protein metabolism Protein metabolism Lipid metabolism Lipid metabolism Carbohydrate metabolism Carbohydrate metabolism
 Growth & development ( skeletal & nervous system) General metabolism ( ↑ oxidation) General metabolism ( ↑ oxidation) Protein metabolism Protein metabolism Lipid metabolism Lipid metabolism Carbohydrate metabolism Carbohydrate metabolism")
60
Thyroid Hormones Hypothalamus TRH (Thyrotropin releasing hormone) Pituitary TSH (Thyroid stimulating hormone) TSH (Thyroid stimulating hormone)Thyroid T4 thyroxine T3 thyronine iodine Permissive role: Allow for normal cell function & growth Induce N retention for protein synthesis Stimulate growth H release Increases metabolic rate
 Pituitary TSH (Thyroid stimulating hormone) TSH (Thyroid stimulating hormone)Thyroid T4 thyroxine T3 thyronine iodine Permissive role: Allow for normal cell function & growth Induce N retention for protein synthesis Stimulate growth H release Increases metabolic rate")
61
Roles Metabolic Rate Metabolic Rate BMR BMR ↑ heat production↑ heat production Newborns Newborns Stress Stress Weight regulationWeight regulation SNS Activity SNS Activity ↑ -receptors↑ -receptors ↑ Heart rate↑ Heart rate Brain activity, muscle activityBrain activity, muscle activity Brain development and body growth Brain development and body growth Stimulates GH releaseStimulates GH release

62
Congenital hypothyroidism approximately 1:4000 newborns approximately 1:4000 newborns the most common treatable cause of mental retardation the most common treatable cause of mental retardation inverse relationship between age at diagnosis and intelligence quotient (IQ) later in life inverse relationship between age at diagnosis and intelligence quotient (IQ) later in life
 later in life inverse relationship between age at diagnosis and intelligence quotient (IQ) later in life")
Similar presentations



































. Its size depends on: 1. age … age size. 2. sex … female > male. 3.>")