Download presentation
Presentation is loading. Please wait.

1
Pathology of the thyroid

2
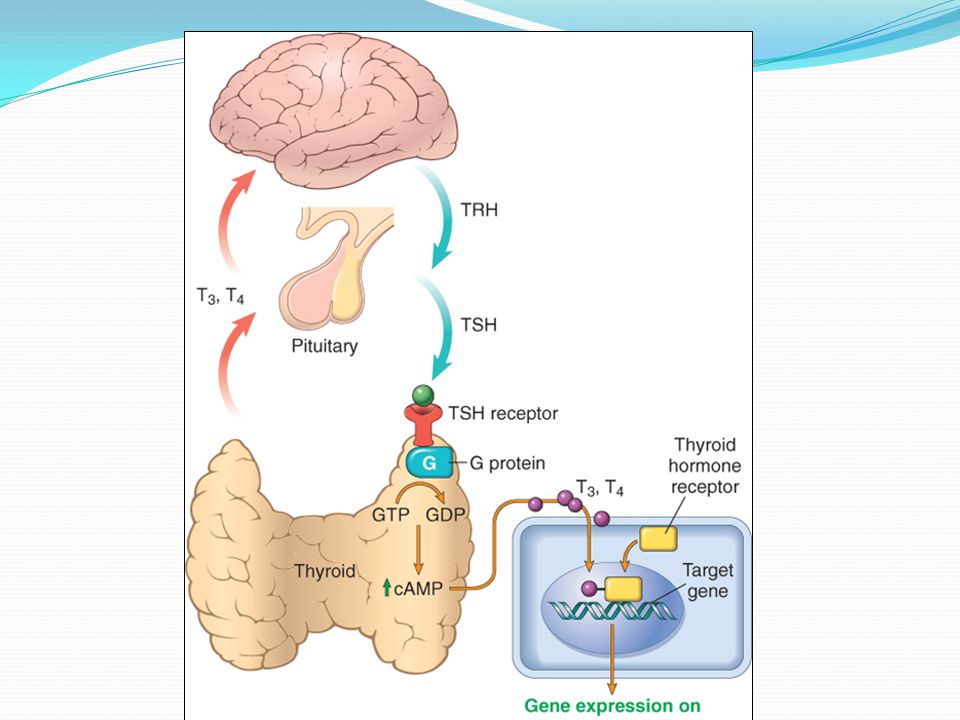
Derived from pharyngeal epithelium Descends from foramen cecum to lower neck Lingual thyroid or ectopic in neck 2 lobes and isthmus, 15-25 gr, richly vascular Follicular cells : T4 Parafollicular cells : Calcitonin T4,3 mostly bind to TBG, the remaining FT4,3 T3 10 folds greater affininty than T4 TRH TSH T4 T3

4
Normal thyroid gland

6
Thyroid diseases Hyperthyroidism Hypothyroidism Mass lesions

7
Causes of thyrotoxicosis With hyperthyroidism Primary 1. Graves disease 2. Toxic multinodular goiter 3. Toxic adenoma Secondary TSH-secreting pituitary adenoma (rare) Without Hyperthyroidism Thyroiditis (Subacute granulomatous/lymphocytic) Struma ovarii Factitious thyrotoxicosis
 Without Hyperthyroidism Thyroiditis (Subacute granulomatous/lymphocytic) Struma ovarii Factitious thyrotoxicosis.")
8
Hyperthyroidism (#thyrotoxicosis)
")
9
Clinical features of hyperthyroidism 1. Constitutional 2. Gastrointestinal 3. Cardiac 4. Neuromuscular 5. Ocular 6. Thyroid storm 7. Apathetic

10
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Hyperthyroidism
 © 2005 Elsevier Hyperthyroidism")
11
Diagnosis of hyperthyroidism 1. Low TSH 2. High T4 3. Radioiodine uptake In secondary hyperthyroidism, TSH is normal or raised T3 toxicosis: Normal T4, High T3

12
Thyroid scan

13
Causes of hypothyroidism Primary 1. Postablative: surgery, radioiodine, radiation 2. Hashimoto thyroiditis* 3. I- deficiency* 4. Congenital defect (dyshormonogenetic goiter)* 5. Drugs (Li, I, p-aminosalicylic acid)* 6. Rare developmental abnormalities of thyroid (thyroid dysgenesis) Secondary Pituitary or hypothalamic failure (uncommon) * Goiterous hypothyroidism
* 5. Drugs (Li, I, p-aminosalicylic acid)* 6. Rare developmental abnormalities of thyroid (thyroid dysgenesis) Secondary Pituitary or hypothalamic failure (uncommon) * Goiterous hypothyroidism.")
14
Hypothyroidism Clinical Features: Cretinism Myxedema Diagnosis: high TSH Low T4

15
Thyroiditis

16
Hashimoto’s thyroiditis F>>M, 45-65 yr Most common thyroiditis in I sufficeint areas Autoimmune: CD 4 T cells (cytokine mediated), CD 8 cytotoxicity, Ab-dep cell mediated cytotoxicity by NK cells
, CD 8 cytotoxicity, Ab-dep cell mediated cytotoxicity by NK cells")
17
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Pathogenesis of Hashimoto’s thyroiditis
 © 2005 Elsevier Pathogenesis of Hashimoto’s thyroiditis")
18
Hashimoto’s thyroiditis F>>M, 45-65 yr Most common thyroiditis in I sufficeint areas Autoimmune: CD 4 T cells (cytokine mediated), CD 8 cytotoxicity, Ab-dep cell mediated cytotoxicity by NK cells AutoAbs: anti TG, anti PO, anti TSHR Genetic: HLA DR3, HLA DR5, CTLA-4 Hypothyroidism, Hashitoxicosis Increased risk of B-cell non Hodgkin lymphoma
, CD 8 cytotoxicity, Ab-dep cell mediated cytotoxicity by NK cells AutoAbs: anti TG, anti PO, anti TSHR Genetic: HLA DR3, HLA DR5, CTLA-4 Hypothyroidism, Hashitoxicosis Increased risk of B-cell non Hodgkin lymphoma")
19
Hashimoto’s thyroiditis

20
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Hashimoto’s thyroiditis
 © 2005 Elsevier Hashimoto’s thyroiditis")
22
Fibrosing variant

23
Other thyroiditis Infectious: Rare, painful Subacute granulomatous (De Quervain’s) Painful, post-viral, enlargement of 1 or 2 lobes, granulomatous inflammation, sudden or gradual hyperthyroidism, self limited Subacute lymphocytic (Silent) Painless, postpartum, Autoimmune, initial phase Of hyperthyroidism followed by euthyroidism Reidel: Autoimmune, diffuse fibrosis Palpation
 Painful, post-viral, enlargement of 1 or 2 lobes, granulomatous inflammation, sudden or gradual hyperthyroidism, self limited Subacute lymphocytic (Silent) Painless, postpartum, Autoimmune, initial phase Of hyperthyroidism followed by euthyroidism Reidel: Autoimmune, diffuse fibrosis Palpation")
24
Gran u lomato u s thyro i d itis

25
Palpation thyroiditis Riedel thyroiditis

26
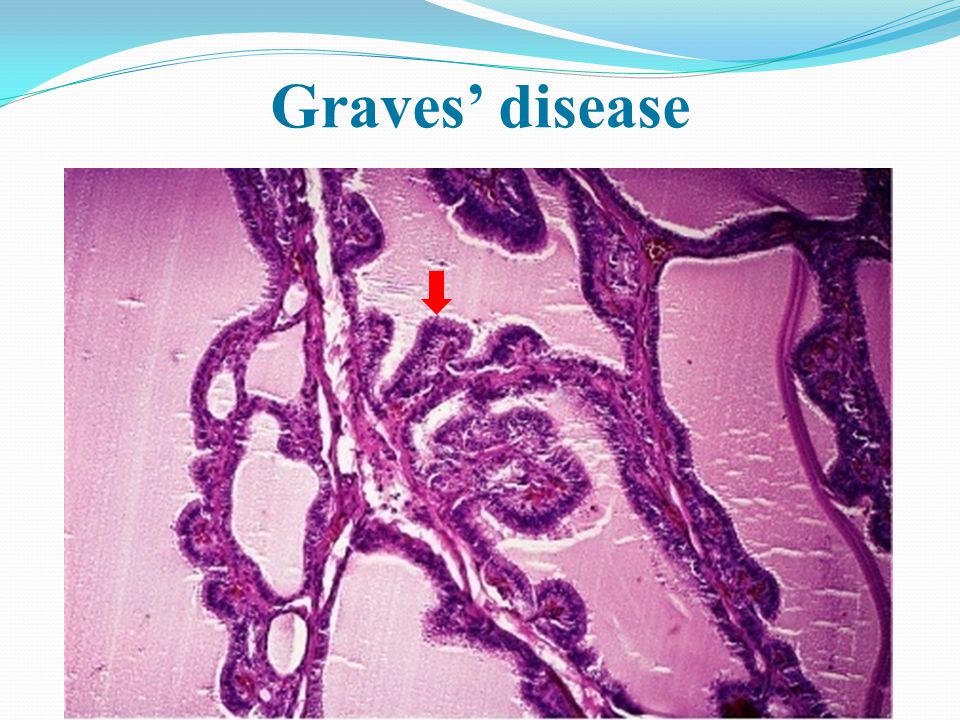
Graves’ disease F>>M, 20-40 yr Most common cause of endogenous hyperthyroidism Genetic: HLA-B8 and DR3, CTLA4, PTPN22 Anti TSHR, Anti TG, anti thyroid peroxisdase Anti TSHR: Thyroid stimulating Ig, TGI (growth), TBII (Inhibitory) Autoimmune thyroid disease span a spectrum from Graves to Hashimoto’s
, TBII (Inhibitory) Autoimmune thyroid disease span a spectrum from Graves to Hashimoto’s")
27
Triad of Graves Hyperthyriodism Ophthalmopathy Dermopathy

28
Graves’ disease

31
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Graves’ disease
 © 2005 Elsevier Graves’ disease")
32
Goiter Most common thyroid disease Diffuse / nodular Endemic goiter (Geograhpic distribution) > 10% Sporadic goiter (Increased demand, substances interfere with synthesis) Dyshormonogenetic goiter Euthyroidism, Plummer syn, hypothyroidism Nodularity: Recurrent episodes of hyperplasia/involution Variation among cells in response to external stimuli
 > 10% Sporadic goiter (Increased demand, substances interfere with synthesis) Dyshormonogenetic goiter Euthyroidism, Plummer syn, hypothyroidism Nodularity: Recurrent episodes of hyperplasia/involution Variation among cells in response to external stimuli")
33
Goiter

36
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Multinodular goiter
 © 2005 Elsevier Multinodular goiter")
37
Goiter

40
Thyroid neoplasms Often present as solitary thyroid nodule Very common Mostly benign Increased chance of malignancy if: Solitary Young Male Hx of radiation Cold nodule

41
Thyroid FNA is a diagnostic test

42
Thyroid FNA

43
Follicular adenoma Solitary in a lobe Soft to firm Cold to hot Activating mutations in TSH receptor causes high cAMP 20% mutations in RAS oncogene (Also in follicular carcinoma) Often non functional, toxic
 Often non functional, toxic")
44
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Follicular adenoma
 © 2005 Elsevier Follicular adenoma")
48
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Follicular adenoma
 © 2005 Elsevier Follicular adenoma")
49
Follicular Adenoma

50
Hurthle cell adenoma

51
Thyroid carcinomas ~ 1% of CA related death F >M Mostly in adults, children (papillary CA) Mostly well diff Risk factors: Radiation in childhood, I-def Papillary CA: 75-85% Follicular CA: 10-20% Meduallary CA: 5% Anaplastic CA< 5%
 Mostly well diff Risk factors: Radiation in childhood, I-def Papillary CA: 75-85% Follicular CA: 10-20% Meduallary CA: 5% Anaplastic CA< 5%")
52
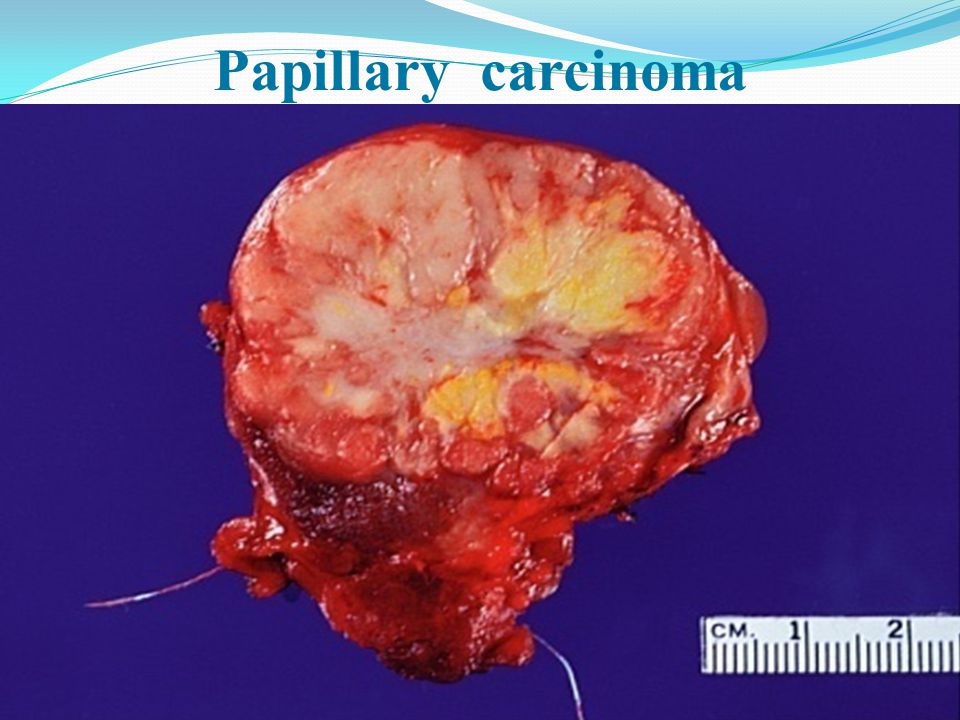
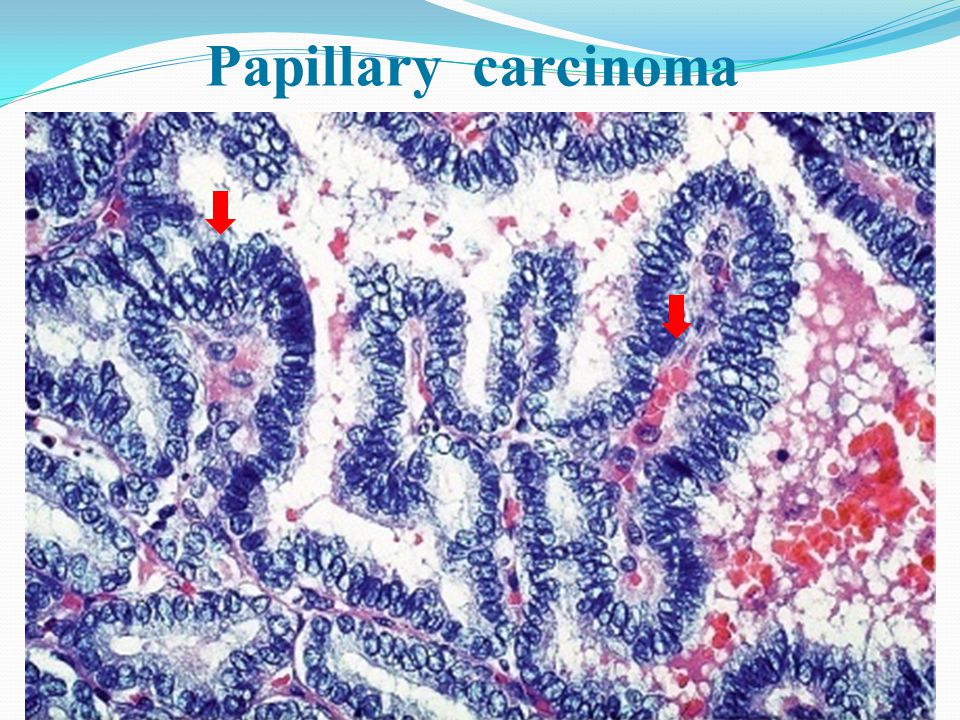
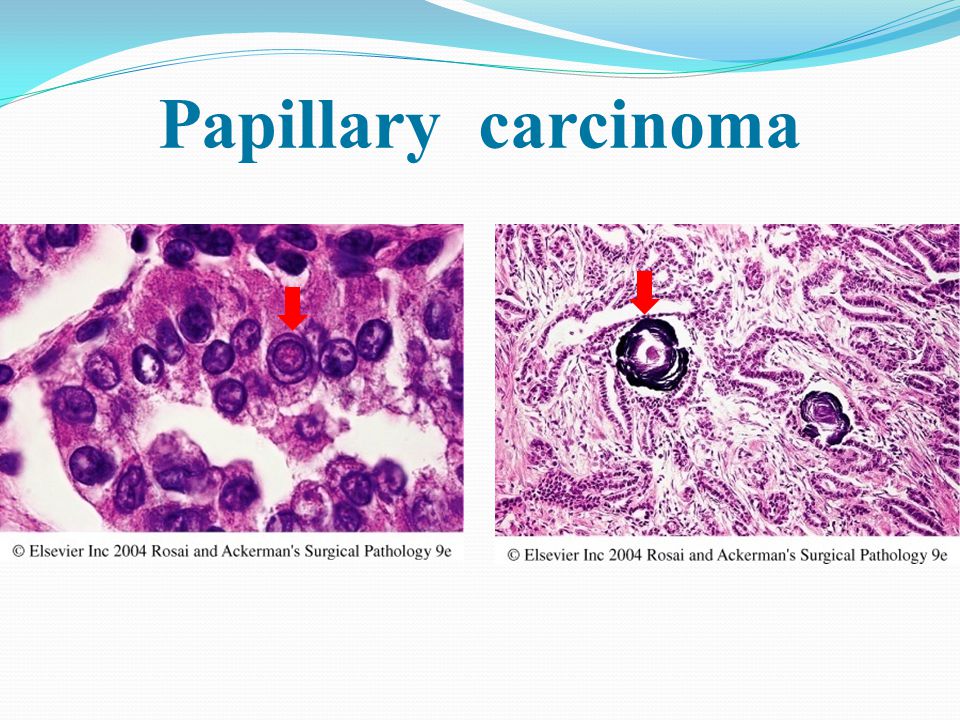
Papillary carcinoma Most common thyroid CA Young age Genetic: MAP kinase signaling pathway ret/PTC or NTRK1 rearrangements BRAF oncogene point mutation Hx of radiation in childhood (RET rearrangement) Painless mass/ cervical lymphadenopathy Indolent course
 Painless mass/ cervical lymphadenopathy Indolent course")
53
Papillary carcinoma

59
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Papillary carcinoma
 © 2005 Elsevier Papillary carcinoma")
60
Follicular Carcinoma Second most common CA Older age (middle age) I -deficiency (nodular goiter) RAS mutation, PAX-PPAR ϒ 1 Cold nodule Blood metastasis common LN metastasis uncommon
 I -deficiency (nodular goiter) RAS mutation, PAX-PPAR ϒ 1 Cold nodule Blood metastasis common LN metastasis uncommon")
61
Follicular carcinoma

62
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Follicular carcinoma
 © 2005 Elsevier Follicular carcinoma")
63
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Follicular carcinoma
 © 2005 Elsevier Follicular carcinoma")
64
Medullary carcinoma Derived from C cells 80% sporadic 20%: MEN II, familial medullary CA RET point mutations > 40 yr, MEN II younger age Mass in thyroid, secretion of hormones Raised serum calcitonin, somatostatin, serotonin, VIP Prophylactic thyroidectomy

65
Medullary carcinoma

66
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Medullary carcinoma
 © 2005 Elsevier Medullary carcinoma")
67
Downloaded from: StudentConsult (on 4 October 2010 11:26 AM) © 2005 Elsevier Medullary carcinoma
 © 2005 Elsevier Medullary carcinoma")
68
Anaplastic carcinoma Elderly, mean=65 yr Rare Lethal Hx of goiter Hx of differentiated thyroid CA Concurrent thyroid CA (papillary) Loss of funcrion of p53
 Loss of funcrion of p53")
69
Anaplastic carcinoma

Similar presentations























. Anatomy Anatomy.>")







FRCSC(Surgical Oncology) Laparoscopic and Bariatric Surgery.>")

