Download presentation
Presentation is loading. Please wait.

1
Presented by Keith W. Crawford, R.Ph., Ph.D. Clinical Research Associate, Department of Clinical Pharmacology, Johns Hopkins School of Medicine, Clinical Pharmacology Baltimore, MD.

2
Identify two ways that the course of HIV infection might be different in individuals infected by different subtypes/clades. Define polymorphism and understand that these genetic variations that may affect protein function can occur at different frequencies across racial/ethnic groups Provide an example of how a polymorphism can affect the response to a drug and why a particular population may be at higher risk for such an effect. Understand that herbal products used in traditional medicines may have unpredictable effects on HIV control.

3
Ethnopharmacology refers to the unique use of drugs and effects of drugs in different ethnic populations From one angle, we can examine the use of medicinal plants among different ethnic groups We can also study varying responses of drugs between different ethnic groups (Pharmacogenetics). We will focus on this area and how it applies to HIV disease.

5
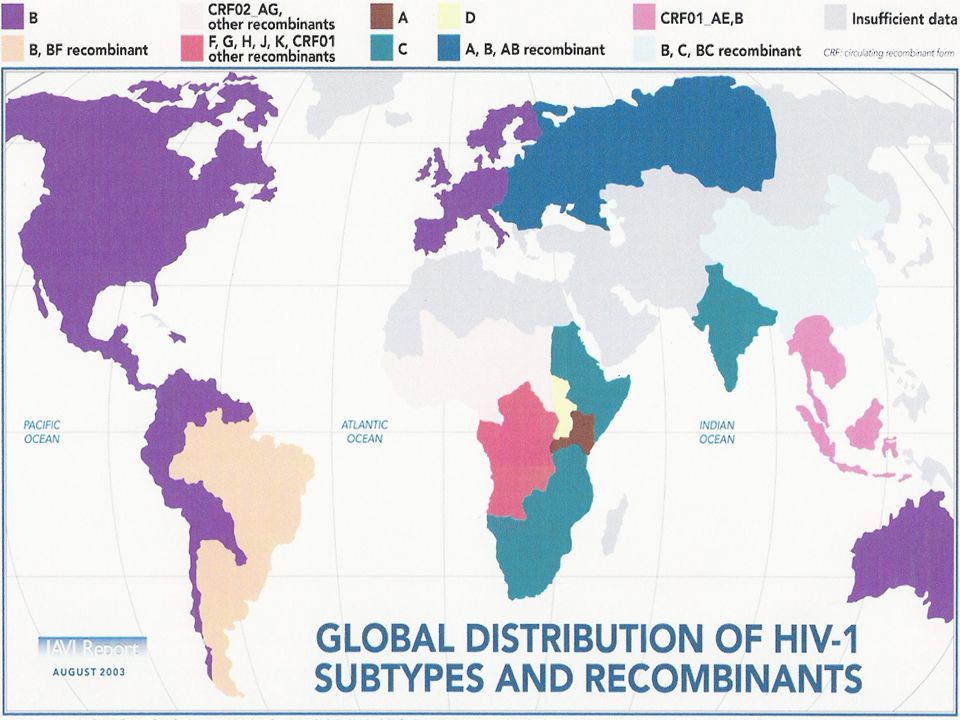
HIV-1HIV-2 Group: O M N Clade:A,C,FBEOthers (Africa)(U.S., Europe)(S.E. Asia) HIV-1 (Cameroon) (less pathogenic) Levy JA. HIV and the Pathogenesis of AIDS. 2nd ed. Washington, DC: American Society for Microbiology; 1998:152-158.
 HIV-1 (Cameroon) (less pathogenic) Levy JA. HIV and the Pathogenesis of AIDS. 2nd ed. Washington, DC: American Society for Microbiology; 1998:")
7
Different clades/subtypes have different efficiencies of heterosexual transmission Different clades/subtypes have different rates of mother-to- child transmission Clades/subtypes produce disease progression at different rates (in the absence of therapy) Whether differences exist between clades/subtypes in anti- retroviral drug potency and treatment response is an area of active clinical investigation.
 Whether differences exist between clades/subtypes in anti- retroviral drug potency and treatment response is an area of active clinical investigation.")
8
CXCR4 CCR5 CD4 T-cell lines Primary lymphocytesMonocyte/macrophages R5X4X4/R5 Dual

9
Phenotypic coreceptor tropism of gp160 env sequences cloned from 68 antiretroviral-naive, pregnant Ugandan women 36% of subtype D samples vs none of subtype A or A/D samples were D/M Phenotypic Tropism Test Result, % Subtype A (n = 33) Subtype A/D (n = 10) Subtype D (n = 25) CCR5 tropic*100 CXCR4 tropic † 0036 *Response range ~ 10 4 -10 6 RLU. † Response range ~ 200-10 5 RLU. Threshold for CXCR4 use = 200 RLU. Huang W, et al. J Virol. 2007;81:7885-7893.

10
Subtype C HIV is among the most widely distributed variants in east and southern Africa In some studies, X4 tropism is not found in treatment- naïve patients with subtype C virus (Cecilia et al., 2000,Virology 271:253-258, Bjorndal et al. AIDS Res. Hum. Retrovir. 1999, 15:647-653, Tscherning,et al. Virology, 1998 241:181-188) X4-tropism (dual/mixed) is seen with increasing frequency upon treatment failure, similar to the case in subtype B virus (Johnston et al.,Virol. 2003 Jul;77(13):7682-8.)
 X4-tropism (dual/mixed) is seen with increasing frequency upon treatment failure, similar to the case in subtype B virus (Johnston et al.,Virol Jul;77(13): ).")
11
Chaplin et al., AIDS Res Hum Retroviruses. 2011 Jan;27(1):71-80. Munerato P et al. AIDS Res Hum Retroviruses. 2010 Mar;26(3):265-73.
:")
12
T.G. is a 32 yo woman originally from Sierra Leone. She is first diagnosed with HIV in September 2001 after being in the US for 5 years Her CD4+ cell count is 328 cells/ml and her HIV RNA is 102,000 copies/ml She is started on a regimen of Sustiva and Combivir In January 2002 her CD4+ cell count is 579 and her HIV RNA is <50 copies

13
In April 2002, her CD4+ cell count has dropped to 402 cells, but she remains undetectable In July of 2002, her CD4+ cell count is now 245, yet her viral load is still undetectable. Why is her CD4+ cell count steadily dropping? She has had no opportunistic infections. The decline is likely not due to adherence since she consistently is undetectable.

14
She is tested for HIV-2 and found to be positive. She was very likely infected in Sierra Leone. HIV-2 is not sensitive to Sustiva. Combivir is the active component of the regimen and dual-nucleoside therapy was not adequate for sustained suppression of HIV-2 The patient is likely having a rebound of HIV-2 (resistant to AZT/3TC), causing CD4+cell decline while the HIV-1 is remains totally suppressed by the regimen. The regimen was changed to a PI-based regimen including abacavir, which lead to CD4+ cell recovery
, causing CD4+cell decline while the HIV-1 is remains totally suppressed by the regimen. The regimen was changed to a PI-based regimen including abacavir, which lead to CD4+ cell recovery.")
16
Substance abuse, particularly stimulant use, is very common among gay men and is associated with increased numbers of partners and unprotected anal intercourse (e.g. Mimiago et al., Drug Alcohol Depend. 2010;110(1-2):30-7)
:30-7).")
18
Leaves from the plant Catha edulis are dried and chewed for the stimulant properties of khat This plant is grown in North and East Africa and the middle East for it’s stimulant effects Abuse of khat is a serious medical problem in Africa and parts of Asia with striking parallels to the crack- cocaine/methamphetamine epidemic in the US

19
Alkaloids of Catha edulis, cathinone and cathine have sympathomimetic effects and stimulant activity Pharmacologic actions similar to those of amphetamine Khat alkaloids increase dopamine concentrations in the critical brain regions for addiction, just as amphetamine but less potent than amphetamine in some brain areas

20
Cathinone Amphetamine

21
Khat use is associated with high-risk sexual behavior in region with high HIV prevalence Alemu et al., J Health Popul Nutr. 2007 Sep;25(3):344-50; Taffa et al Int J STD AIDS. 2002 Oct;13(10):714-9. Khat and its synthetic derivative can be purchased over the internet Wood DM et al.J Med Toxicol. 2010 Sep;6(3):327-30. Clinicians treating patients from Ethiopia, other parts of East Africa and the Middle East should include discussions about khat use when evaluating Mental Health and substance abuse in HIV treatment or prevention programs
:344-50; Taffa et al Int J STD AIDS Oct;13(10): Khat and its synthetic derivative can be purchased over the internet Wood DM et al.J Med Toxicol Sep;6(3): Clinicians treating patients from Ethiopia, other parts of East Africa and the Middle East should include discussions about khat use when evaluating Mental Health and substance abuse in HIV treatment or prevention programs.")
22
All proteins involved in pharmacokinetics (drug absorption, distribution, metabolism and excretion) are under genetic control Alleles are genetic variants in a particular trait and at a specific genetic locus Genetic variation within a specific locus are called polymorphisms These genetic differences in nucleotide sequence can affect the functioning of the protein or even the protein’s expression The frequency of a polymorphism in a population often differs across racial and/or ethnic groups
 are under genetic control Alleles are genetic variants in a particular trait and at a specific genetic locus Genetic variation within a specific locus are called polymorphisms These genetic differences in nucleotide sequence can affect the functioning of the protein or even the protein’s expression The frequency of a polymorphism in a population often differs across racial and/or ethnic groups")
23
Polymorphisms in metabolic enzymes can result in increased or decreased enzyme activity These changes can translate into decreased or increase plasma drug concentrations, respectively Drug concentration determines drug efficacy as well as drug toxicity

24
Marzolini C, et al. AIDS. 2001;15:71-75.

25
Haas D W et al. J Infect Dis. 2005;192:1931-1942

26
Haas DW, et al. AIDS. 2004;18:2391-2400. All Subjects European Americans African Americans 250 200 150 100 50 0 GG GT TT CYP2B6 G516T genotype Efavirenz AUC 0-24hr ( g x hr/mL)
.")
27
Many drugs are substrates for transport proteins that regulate their distribution into tissues. Transporters are involved in intestinal absorption, drug uptake by hepatocytes (metabolism) and bile (elimination), and entry and efflux from renal tubules Examples: ▪ P-glycoprotein (gut, kidney) ▪ MRP’s (kidney, gut) ▪ SCLO (liver)
 and bile (elimination), and entry and efflux from renal tubules Examples: ▪ P-glycoprotein (gut, kidney) ▪ MRP’s (kidney, gut) ▪ SCLO (liver).")
28
Disparities in treatment outcomes for hepatitis C by race and ethnicity are well established. hENT is a major transport protein involved in uptake of ribavirin into cells (also AraC in leukemia and lymphoma therapy). SLC29A1 is the gene that produces hENT and genetic polymorphisms affect the expression of hENT -706 G>C polymorphism affects the expression of the gene and is present in 21% of Caucasians but only 5% African-Americans. Two polymorphisms were found only in African-Americans, - 1345C>G and -1050G>A with allele frequencies of 8% and 19 % (Myers et al.,Pharmacogenet Genomics. 2006 May;16(5):315-20).
. SLC29A1 is the gene that produces hENT and genetic polymorphisms affect the expression of hENT -706 G>C polymorphism affects the expression of the gene and is present in 21% of Caucasians but only 5% African-Americans. Two polymorphisms were found only in African-Americans, C>G and -1050G>A with allele frequencies of 8% and 19 % (Myers et al.,Pharmacogenet Genomics May;16(5):315-20)..")
29
Main Predictors of Rapid Virological Response to Peginterferon-Ribavirin Therapy in Patients Coinfected with Human Immunodeficiency Virus and Hepatitis C Virus (HCV). Morello J et al. J Infect Dis. 2010;202:1185-1191 © 2010 by the Infectious Diseases Society of America

30
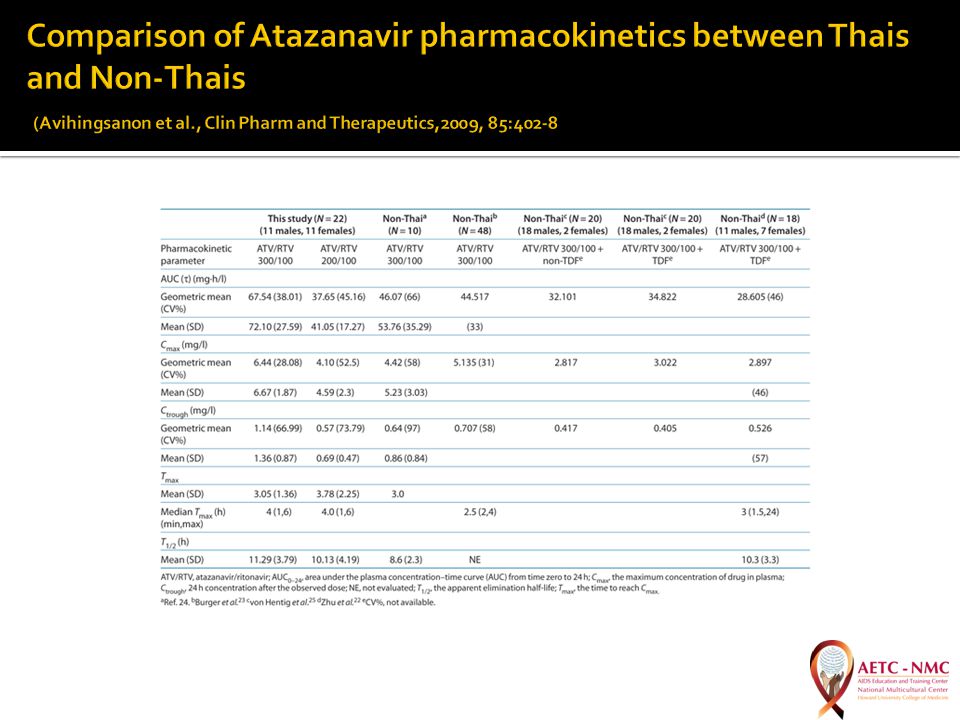
Weight-based dosing has been recommended for some antiretroviral drugs (e.g. stavudine, didanosine) which could possibly minimize toxicities while maintaining efficacy. ART’s used at approved doses, based on phase II/III studies in Caucasians, may have different pharmacokinetic profiles when used at these doses in other populations These differences can be due to differences in body weight and composition as well as pharmacogenetics
 which could possibly minimize toxicities while maintaining efficacy. ART’s used at approved doses, based on phase II/III studies in Caucasians, may have different pharmacokinetic profiles when used at these doses in other populations These differences can be due to differences in body weight and composition as well as pharmacogenetics.")
32
Rozenberg al., AIDS. 2009 Nov 27;23(18):2439-50.
:")
34
CCR5 is a receptor for the chemokines MIP-1 α, MIP-1β expressed on the surface of macrophages and memory T-lymphocytes CCR5 is required as a co-receptor for HIV to infect these cells A 32-base pair deletion mutation polymorphism in the CCR5 gene results in a impaired receptor expression and impaired ability of HIV to infect these cells. Delta-32 deletion homozygotes are Long- term non-progressors in HIV disease This observation suggested that CCR5 could be a target for HIV therapy which lead to development of the chemokine receptor antagonists (e.g. Maraviroc).
..")
35
Homozygous ~ 1% of white population [1] Lack CCR5 molecules on CD4+ cell surface [2,3] Relatively normal immune function Heterozygous 10% to 15% of white population [1] Fewer CCR5 molecules on CD4+ cell surface [4] Normal immune function [2] 1. McNicholl JM, et al. Emerg Infect Dis. 1997;3:261-271. 2. Liu R, et al. Cell. 1996;86:367-367. 3. Samson M, et al. Nature. 1996;382:722-725. 4. Wu L, et al. J Exp Med. 1997;185:1681-1691.
![ Homozygous ~ 1% of white population [1] Lack CCR5 molecules on CD4+ cell surface [2,3] Relatively normal immune function Heterozygous 10% to 15% of white population [1] Fewer CCR5 molecules on CD4+ cell surface [4] Normal immune function [2] 1.](http://images.slideplayer.com/11/3308035/slides/slide_35.jpg "McNicholl JM, et al. Emerg Infect Dis. 1997;3: Liu R, et al. Cell. 1996;86: Samson M, et al. Nature. 1996;382: Wu L, et al. J Exp Med. 1997;185:")
37
Abacavir produces a potentially fatal hypersensitivity reaction in about 5% of users A polymorphism in the HLA-B genetic locus (HLA-B*5701) was found associated with abacavir hypersensitiviy in whites and Latinos, but in African-Americans, initial studies found it alone lacked sufficient predictive value to identify patients at risk (Hughes, et al., Pharmacogenomics. 2004 Mar;5(2):203- 11). The rate of hypersensitivity is higher in whites, from 5-8%, compared to about 3% in African-Americans
: ). The rate of hypersensitivity is higher in whites, from 5-8%, compared to about 3% in African-Americans.")
38
Sensitivity of HLA-B*5701 Test Patient Group, %White PatientsBlack Patients CS-HSR4414 Skin test positivity100 Control9699 Saag et al.,Clin Infect Dis. 2008 Apr 1;46(7):1111-8
:")
40
Digitalis from Foxglove – CHF, atrial fibrillation Cinnchona alkaloids from Cinnchona bark – quinidine–anti-arrhythmic, quinine – anti-malarial Coumadin from Red clover – anticoagulant Salicylates from Willow bark – aspirin - anti-inflammatory, analgesic, anti- pyretic Cocaine from Coca leaves – local anesthetic Opioid alkaloids from Poppy – morphine – analgesic for moderate to severe pain Artemisinins –anti-malarials Vinca alkaloids from Periwinkle, vincristine, vinblastine – anti-cancer Ergot alkaloids from fungus, Claviceps pupura – migraine treatment and prophyllaxis, obstetric complications Rauwolfia alkaloids - reserpine – HTN, schizophrenia Guanidine from Goat’s Rue – Diabetes Penicillins –from molds Tetracyclins- from molds Taxanes – from Yew, paclitaxel, taxotere for treating various tumors

41
What dose is most effective and how often should it be given? No dose studies are done for most herbal products so where do the recommended doses come from? How much of the specified compound is actually in the product? In some studies, analysis found none of the “medicinal” compound in the product. Herbal products have no regulation. Is the product safe? Herbal products have no safety requirements and seldom identify any precautions. People have died from using some of these products (e.g. Ephedrine) Does the product actually work? Efficacy studies are not required to market supplement product.
 Does the product actually work. Efficacy studies are not required to market supplement product..")
42
Plants produce varying quantities of alkaloids based on there growing conditions There are seasonal variations in the quantity of “medicinal” product produced by the plant Variation in extraction procedures result in varying efficiencies in yield of the product. There is often little standardization of this crucial process

43
Calanolide A is one of the most potent inhibitors of HIV from natural sources Derived from the Southeast Asian plant Calophyllum lanigerum Inhibits HIV reverse transcriptase at concentrations comparable to antiretrovirals

44
St. Johns Wort reduces the bioavailability of indinavir Garlic supplementation decreased the bioavailabilty of Saquinavir Milk Thistle shown not to have an effect on indinavir levels

45
Piscitelli et al., Lancet. 2000 Feb 12;355(9203):547-8.
:547-8.")
46
Among many ethnic groups, traditional medical practices may include the use of herbal therapies. Which statement is correct about herbal treatments and HIV disease? A. Because herbal products are natural, the body can handle the compound differently than it does synthetic drugs, and hence, herbs are not toxic. B. These products may have interactions with antiretroviral drugs that can affect their efficacy C. These products are regulated by the Food and Drug administration as “foods” and are proven to be safe D. Both A and C are correct E. All of the above are correct

47
Goulda Downer, Ph.D., RD, LN, CNS - Principle Investigator/Project Director (AETC-NMC) Tina Edmunds-OGBUOKIRI Pharm.D I Jean Davis, PhD, PA, AAHIVS Michael R. Noss, DO Josepha Campinha-Bacote, PhD, MAR, PMHCNS-BC, CTN-A, FAAN

48
48

Similar presentations











 Glycoprotein envelope with protein knobs on surface. Core is cone-shaped & contains RNA and the.>")





 is the virus that causes Acquired Immunodeficiency Syndrome (AIDS).>")






