Download presentation
Presentation is loading. Please wait.

1
Shou-Ching Tang MD, PhD, FACP, FRCP (C) GRU Cancer Center
2013 SABCS Review Shou-Ching Tang MD, PhD, FACP, FRCP (C) GRU Cancer Center
 GRU Cancer Center.")
2
Disclosure Nothing to declare

3
outline Prognostic and predictive biomarkers Prevention
Early breast cancer locally advanced breast cancer Advanced breast cancer Targeted therapy Conclusion

4
Prognostic and predictive biomarkers

5
Genetic landscape of MBC Bachelot et al, #S6-07, SABCS 2013
Exome sequencing of 100 pairs of MBC and normal breast tissue DNA (Integragen Inc, Hiseq platform) Targeted sequencing of 100 genes in 240 MBC biopsies PIK3CA 26%, AKT1 4%, PTEN 4%, ERBB 2%, K-Ras 1%, ATM 1%, CDH1 2%, GATA3 2%. PTPN11 1%, PTPRD 1%, ROS1 1% Many of them are drugable and involved in metastatic process and drug resistance
 Targeted sequencing of 100 genes in 240 MBC biopsies. PIK3CA 26%, AKT1 4%, PTEN 4%, ERBB 2%, K-Ras 1%, ATM 1%, CDH1 2%, GATA3 2%. PTPN11 1%, PTPRD 1%, ROS1 1% Many of them are drugable and involved in metastatic process and drug resistance.")
6
Exome sequencing to identify actionable mutations in mTNBC Blackwell et al, S4-04, SABCS 2013
38 pts with mTNBC and matched specimens of germ-line DNA, primary and metastatic tumors Whole-exome sequencing by Agilent solution-based system of exon capture with 10 GB of sequencing data Striking genetic heterogeneity between primary and metastatic tumors continues

7
Exome sequencing to identify actionable mutations in mTNBC Blackwell et al, S4-04, SABCS 2013
No single driver mutation that was common to metastatic tumors, indicating diverse genetic pathways contributing to metastasis Mutations in APC and mTOR more frequent in metastatic than primary tumors Nonsense mutations of ER in primary and metastatic tumors but not in germ-line DNA EGFR and HER2 mutations not detected

8
Gene mutations and protein expression in TNBC vs non-TNBC O’Shaughnessy et al, #PD4-1, SABCS 2013
5500 pts evaluated for mutation (Sanger or Illumina Truseq), protein expression (IHC) and/or amplification/rearrangement (FISH or CISH), 16% with TNBC Mutation: TNBC has higher p53 mutation (60% vs 30%), lower PIK3CA (12% vs 31%) Amplification: TNBC has higher amplification of EGFR (24% vs 13%), lower HER2, PIK3CA, cMYC and TOP2A IHC: TNBC has higher AR (56% vs 15%)
, protein expression (IHC) and/or amplification/rearrangement (FISH or CISH), 16% with TNBC. Mutation: TNBC has higher p53 mutation (60% vs 30%), lower PIK3CA (12% vs 31%) Amplification: TNBC has higher amplification of EGFR (24% vs 13%), lower HER2, PIK3CA, cMYC and TOP2A. IHC: TNBC has higher AR (56% vs 15%)")
9
Heterogeneity between primary and met BC prior to Tx Bidard et al, #S6-06, SABCS 2013
High-depth whole exome sequencing and SNP6 copy number profiling of primary and met biopsies from 7 pts with de novo MBC prior to systemic therapy Significant genomic differences between primary and met tumors Median 105 of single nucleotide variants (SNVs) and 54 insertions/deletions (indels) identified, of which 36 and 11 were shared between the primary and secondary tumors 50% driver SNV’s and 70% pathogenic indels were restricted to either primary or met tumors, including the epithelial-to-mesenchymal transition (EMT)-related genes TGFB1, SMAD4 and TCF7L2
 and 54 insertions/deletions (indels) identified, of which 36 and 11 were shared between the primary and secondary tumors. 50% driver SNV’s and 70% pathogenic indels were restricted to either primary or met tumors, including the epithelial-to-mesenchymal transition (EMT)-related genes TGFB1, SMAD4 and TCF7L2.")
10
Community-based NGS to guide clinical trial selection Yardley et al, abst PD4-3, SABCS 2013
594 advanced BC profiled Most frequently altered gene: PIK3CA (24%), followed by RUNX1 (4%) and FGFR3 (2%) Infrequent: PIK3R1, MET, KRAS, KIT, FGFR2, HER2, BRAF, SMO, MYC, DDR2 and AKT1, one pt each 6% pts enrolled in phas I trials based on NGS (PI3K and mTOR inhibitor), 29% pts potentially eligible for ongoing trials at SCRI PIK3CA mutation accounted for 70% of 35% actionable mutations detected
, followed by RUNX1 (4%) and FGFR3 (2%) Infrequent: PIK3R1, MET, KRAS, KIT, FGFR2, HER2, BRAF, SMO, MYC, DDR2 and AKT1, one pt each. 6% pts enrolled in phas I trials based on NGS (PI3K and mTOR inhibitor), 29% pts potentially eligible for ongoing trials at SCRI. PIK3CA mutation accounted for 70% of 35% actionable mutations detected.")
11
PI3KCA mutation predicts resistance in HER2+/ER+ BC Loibl et al, #S4-06, SABCS 2013
Prospectively analyzed 512 pts from Geparsixto and validated in 225 pts from GeparQuinto trials PI3KCA mutation found in 19.2% HER2+ tumors, more in HER2+/ER+, 21.5% pCR in pts with and without PI3KCA mutation vs 43.6 %, p=0.001 with HER2+/ER+ tumors 6.5% vs 30.8%, p=0.005 No difference in HER2+/ER- tumors 42.9% vs 46.1%, p=0.852

12
PIK3CA mutation and/or low PTEN predict resistance to lapatinib and trastuzumab Contreras, et al, #PD1-2, SABCS 2013 Neoadjuvant L plus T (no chemo) x 12 wks 59 pts tested for PTEN (IHC) and 33 for PI3KCA mutation (36% by NGS) pCR: overall 16% high vs low PTEN 32% vs 9% p=0.04 PIK3CA mutation: 0% p=0.06 low PTEN and PIK3CA mutation vs normal: 0% vs 36% p=0.01
 x 12 wks. 59 pts tested for PTEN (IHC) and 33 for PI3KCA mutation (36% by NGS) pCR: overall 16% high vs low PTEN 32% vs 9% p=0.04. PIK3CA mutation: 0% p=0.06. low PTEN and PIK3CA mutation vs normal: 0% vs 36% p=0.01.")
13
Prognostic value of tumor infiltrating lymphocytes (TIL’s)
% of lymphocyte infiltration in tumor stroma reflects host immune reaction The presence of TIL’s was correlated with benefit from: trastuzumab in HER2+ EBC in 156 pts from the neoadjuvant GeparQuattro trial (Loi et al, #S1-05, SABCS 2013) the addition of carbo to neoadjuvant therapy in TN and HER2+ EBC in Geparsixto trial (Dunkert, et al, #S1-06) adjuvant therapy in ECOG 2197 and 1199 in TNBC (Adams et al, #S1-07, SABCS 2013)
 the addition of carbo to neoadjuvant therapy in TN and HER2+ EBC in Geparsixto trial (Dunkert, et al, #S1-06) adjuvant therapy in ECOG 2197 and 1199 in TNBC (Adams et al, #S1-07, SABCS 2013)")
14
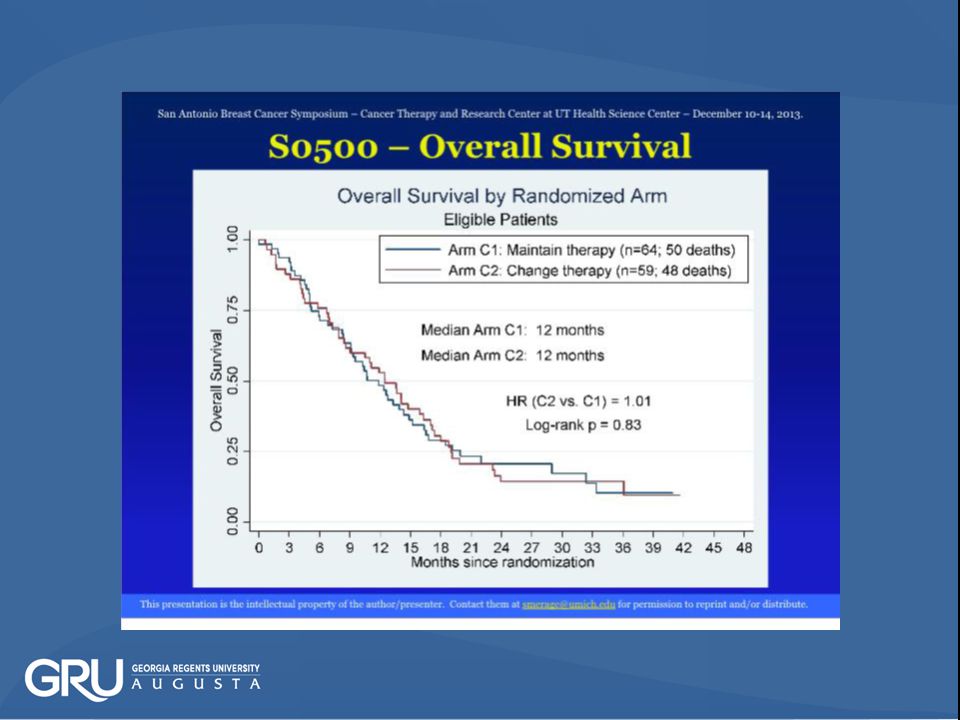
SWOG S0500 CTC’s in guiding CT in MBC Smerage et al, #S5-07, SABCS 2013
(CTC found in 75% MBC, half >5CTC/7.5 ml whole blood) Primary end point: OS
 Primary end point: OS.")
19
SWOG S0500 CTC’s in guiding CT in MBC Smerage et al, #S5-07, SABCS 2013
Conclusion: CTC prognostic in MBC at baseline and after first chemo Changing chemo based on CTC after first chemo does not affect OS or PFS

20
PAM50 to predict late relapse in EBC Sestak et al, #S6-04, SABCS 2013
2485 pts from ABCSG-8 and transATAC trials who did not relapse in 0-5 yrs Clinical treatment score (CTS, from transATAC) is the strongest prognostic score for late relapse PAM50 risk of recurrence (ROR) score adds significant prognostic value for late relapse Risk of distant relapse at 10 yrs for low risk group is 5.7%, intermediate risk 14.6% and high risk 29.3% Pts with luminal A subtype had a 70% lower risk of distant relapse than luminal B (HR 0.03, p<0.0001)
 is the strongest prognostic score for late relapse. PAM50 risk of recurrence (ROR) score adds significant prognostic value for late relapse. Risk of distant relapse at 10 yrs for low risk group is 5.7%, intermediate risk 14.6% and high risk 29.3% Pts with luminal A subtype had a 70% lower risk of distant relapse than luminal B (HR 0.03, p<0.0001)")
21
prevention

22
IBIS-II Chemo-prevention in high risk postmenopausal women Cuzick et al, #S3-01, SABCS 2013
Randomized phase III UK trial 3864 women with high risks of BC, median f/u 5.03 yrs Primary end point: incidence of BC, including DCIS Anastrozole vs placebo for 5 years

23
IBIS-II: Chemo-prevention in high risk postmenopausal women Cuzick et al, #S3-01, SABCS 2013
5-yr BC incidence: 53% reduction, p<0.0001 Significant reduction in all invasive BC (50%), ER+ BC (58%) and DCIS (70%) Significant reduction of cancer at other sites (RR=0.58) Deaths from BC and other causes similar in both arms Musculoskeletal and vosomotor events higher and bone # non-significantly higher in anastrozole arm In support of other chemoprevention trials: TAM (NSABP P-1), raloxifen (STAR)and exemestane (MAP3)
, ER+ BC (58%) and DCIS (70%) Significant reduction of cancer at other sites (RR=0.58) Deaths from BC and other causes similar in both arms. Musculoskeletal and vosomotor events higher and bone # non-significantly higher in anastrozole arm. In support of other chemoprevention trials: TAM (NSABP P-1), raloxifen (STAR)and exemestane (MAP3)")
24
Early breast cancer

25
Hormone and physical exercise (HOPE) in EBC Irwin et al, #S3-03, SABCS 2013
Randomized phase III multicenter US trial 121 pts on adjuvant AI for > 6 m and with >3/10 worst joint pain on Brief Pain Inventory-Short form (BPI) 150 min/wk mod-intense aerobic exercise and twice-wkly supervised resistance exercise or usual care Primary end point: change in BPI worse joint pain score between 0-12 momths reduction of BPI score (20% vs 3% , p=0.017), joint pain intensity (p=0.025), body wt (p=0.0057) and increase in cardiopulmonary fitness (p=0.024) Impact on adherence to AI’s and survival?
 150 min/wk mod-intense aerobic exercise and twice-wkly supervised resistance exercise or usual care. Primary end point: change in BPI worse joint pain score between 0-12 momths. reduction of BPI score (20% vs 3% , p=0.017), joint pain intensity (p=0.025), body wt (p=0.0057) and increase in cardiopulmonary fitness (p=0.024) Impact on adherence to AI’s and survival")
26
Bisphosphonates and survival in EBC: meta-analysis Coleman et al, #S4-07, SABCS 2013
36 randomized trials, 22,982 pts Primary end point: time to recurrence, to first distance recurrence and breast cancer mortality

27
Bisphosphonates and survival in EBC: meta-analysis Coleman et al, #S4-07, SABCS 2013
RR 10-yr gain % 2p value All pts BC mortality distance recurrence Post-menopausal pts BC mortality distance recurrence

28
Bisphosphonates and survival in EBC: meta-analysis Coleman et al, #S4-07, SABCS 2013
Reduction in bone relapse in postmenopausal pts similar regardless of type of BP tx, duration and schedule or concomitant chemotherapy Adjuvant BP improves survival in postmenopausal pts with EBC No benefit in premenpausal pts in bone or other recurrences Currently indicated for prevention or treatment of bone loss

29
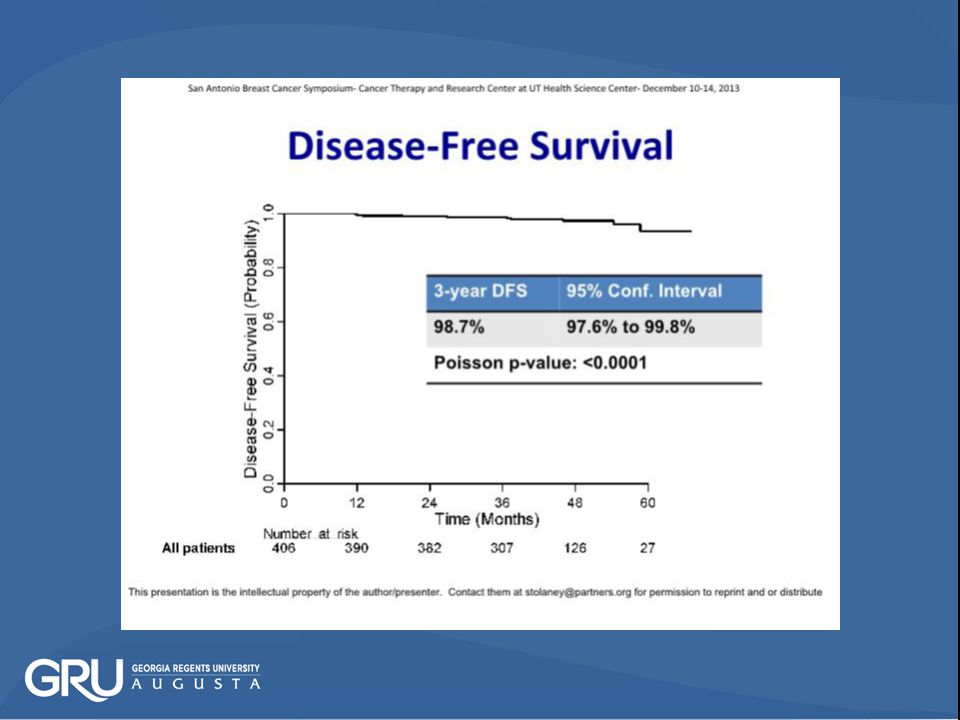
Phase II study of TH in HER2+ and node- EBC Tolaney, S et al, #S1-04, SABCS 2013
410 pts, HER2+ EBC T1mi 3%; T1a 27%, T1b 20%, T1C 41%, T2<3 cm 9% Wkly paclitaxel x12 with trastusumab for one year Null hypothesis: 3-year failure rate of 9.2% (failure) Alternative hypothesis: 3-year failure rate of 5% (success) Due to limited number of events, DMSB approved data release with 1316 PYFU and median f/u of 3.2 years
 Alternative hypothesis: 3-year failure rate of 5% (success) Due to limited number of events, DMSB approved data release with 1316 PYFU and median f/u of 3.2 years.")
31
TH in node-/HER2+ EBC TH is highly effective and well tolerated
Can be considered an option in majority of stage 1 HER2+ EBC Single arm study, 67% HR+ tumor, limited follow up of 3.6 years Superior survival data suggest not all pts with stage 1 HER2+ EBC require trastuzumab-based chemotherapy, esp those with T1aN0 tumor Addition of another biological agent to TH backbone is unlikely to have substantial benefit in this pt population (TDM-1 vs TH ongoing)
")
32
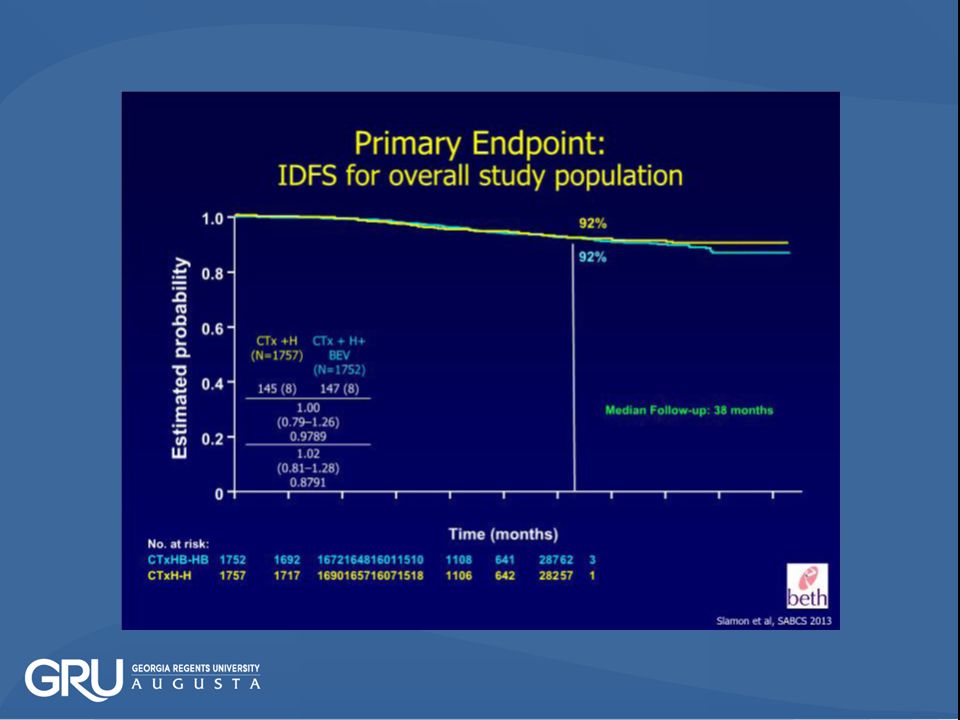
Primary results of BETH trial in HER2+, node+ or node- high risk EBC Slamon D et al, #S1-03, SABCS 2013 3509 pts, phase III Median f/u 3 years Invasive disease-free survival (IDFS) BETH Trial Docetaxel x 6 Carboplatin x 6 Trastuzumab x 1 y Bevacizumab 15mg q3 wk x 1 y 92% or 5-FU x 3 Epirubicin x 3 Cylophos x 3 Docetaxel x 3 Trastuzumab x 1 y Observation 8%
 BETH Trial. Docetaxel x 6. Carboplatin x 6. Trastuzumab x 1 y. Bevacizumab 15mg. q3 wk x 1 y. 92% or. 5-FU x 3. Epirubicin x 3. Cylophos x 3. Docetaxel x 3. Trastuzumab x 1 y. Observation. 8%")
37
BETH primary result Addition of one year bevacizumab to chemotherapy did not prolong invasive disease-free survival (IDFS) TCH is an effective adjuvant regimen for pts with HER2+ EBC, including node+ tumors No new or unexpected safely signals No added benefit of bev in MBC, LABC and EBC in unselected pts, biomarker studies urgently needed (ongoing repeat of ECOG trial with biomarkers included)
")
38
GIM-2 EC or FEC with dd P or not in node+ EBC Cognetti et al, # S5-06, SABCS 2013
Italian multicenter randomized phase III 2x2 design 2019 pts, node+, < 70 yo, median f/u 7 yrs EC x4 or FEC x4 then P q 2 (with G) or 3 wks x4 Primary end point: DFS DD CT improved DFS and OS : HR 0.78 (p=0.007) and 0.68 (p=0.002) respectively Benefit of DD CT independent of HR status Addition of F to EC did not improve outcome
 or 3 wks x4. Primary end point: DFS. DD CT improved DFS and OS : HR 0.78 (p=0.007) and 0.68 (p=0.002) respectively. Benefit of DD CT independent of HR status. Addition of F to EC did not improve outcome.")
39
PRIME II: Adjuvant RT in pts > 65 yo Kunkler et al, #S2-01, 2013 SABCS
Multicenter UK trial, 1326 pts, median f/u 5 yrs >65 yo, T 1-2 (up to 3 cm), N0/M0, HR+, margin > 1mm, could be grade 3 or LVI but not both, required adjuvant hormonal therapy Primary end point: ipsilateral breast tumor recurrence no RT (%) RT (%) p IBTR OS Regional relapse Contralateral relapse Distance relapse Results similar to CALGB, ECOG and RTOG trial (pASCO 2010) Omission of adjuvant RT safe in selected older pts
, N0/M0, HR+, margin > 1mm, could be grade 3 or LVI but not both, required adjuvant hormonal therapy. Primary end point: ipsilateral breast tumor recurrence. no RT (%) RT (%) p. IBTR OS Regional relapse Contralateral relapse Distance relapse Results similar to CALGB, ECOG and RTOG trial (pASCO 2010) Omission of adjuvant RT safe in selected older pts.")
40
10-yr survival update of NSABP B-32 Julian et al, #S2-05, SABCS 2013
Randomized phase III of SLND plus ALND or ALND 5611 pts Still no difference in OS, DFS and loco-regional relapse (HR 1.09, p=0.35; HR 1.02, p=0.72; HR 0.96, p=0.77 respectively) No difference in OS and DFS in pts with occult mets detected by IHC with or without ALND IHC has no prognostic role in EBC
 No difference in OS and DFS in pts with occult mets detected by IHC with or without ALND. IHC has no prognostic role in EBC.")
41
Locally advanced breast cancer

42
Neo ALTTO Survival update Piccar-Gebhart, M et al, #S1-01, SABCS 2013
Stratification: T ≤ 5 cm vs. T > 5 cm ER or PgR + vs. ER & PgR – N 0-1 vs. N ≥ 2 Conservative surgery or not Invasive operable HER2+ BC T > 2 cm (inflammatory BC excluded) LVEF 50% N=450 S U R G E Y A N D O M I Z E lapatinib trastuzumab paclitaxel + 12 wks 6 wks 34 weeks 52 weeks of anti-HER2 therapy lapatinib trastuzumab F E C X 3 Median f/u years 42
 LVEF 50% N=450. S. U. R. G E. Y. A. N. D. O. M. I. Z. E. lapatinib. trastuzumab. paclitaxel wks. 6 wks. 34 weeks. 52 weeks of anti-HER2 therapy. lapatinib. trastuzumab. F. E. C. X. 3. Median f/u 3.77 years. 42.")
43
NeoALTTO Efficacy – pCR and tpCR
L: lapatinib; T: trastuzumab; L+T: lapatinib plus trastuzumab pCR pathologic complete response HR: hormone receptors Baselga J et al. SABCS 2010; abstract S3-3

48
NeoALTTO survival update
First study to show that pts with pCR had significantly better EFS and OS with HER2+ tumors Study was powered to detect difference in pCR, but underpowered to detect moderate difference in survival Dual HER2 blockade is superior HER2+/HR- and HER2+/HR+ subgroups are different diseases

49
TRIO-US B07 final analysis Hurvitz S et al, #S1-02, SABCS 2013
Randomized phase II of neoadjuvant H or L or both in stage 1-3, HER2+ EBC 106 pts in 13 US centers, primary end point, pCR Run-in cycle of H or L or both followed by 6 cycles of TCH (A) vs TCL (B) or TCHL (C) Overal pCR: 42% (A 43%, B 25% and C 52%, p=0.069) Pair-wise comparison: pCR in B significantly lower than C (p=0.021), not different between A and B (p=0.14) and A and C (p=0.45)
 vs TCL (B) or TCHL (C) Overal pCR: 42% (A 43%, B 25% and C 52%, p=0.069) Pair-wise comparison: pCR in B significantly lower than C (p=0.021), not different between A and B (p=0.14) and A and C (p=0.45)")
50
CALGB 40603 (Alliance) neoadjuvant carbo +/- Bev in TNBC Sikov et al, #S5-01, SABCS 2013
2x2 randomized phase II in locally advanced TNBC in 545 pts

51
CALGB 40603 (Alliance) neoadjuvant carbo +/- Bev in TNBC Sikov et al, #S5-01, SABCS 2013
pCR (%, breast and axilla): no Cb Cb Bev effect No Bev Bev p=0.031 Cb benefit p=0.033 Addition of Cb or Bev to NAC significantly increases pCR in TNBC, and the increases are additive Several studies now support the addition of Cb to standard CT in LABC (CALGB 40604, GeparSixto and I-Spy 2), adjuvant trials ongoing
: no Cb Cb Bev effect. No Bev Bev p= Cb benefit 10.3 p= Addition of Cb or Bev to NAC significantly increases pCR in TNBC, and the increases are additive. Several studies now support the addition of Cb to standard CT in LABC (CALGB 40604, GeparSixto and I-Spy 2), adjuvant trials ongoing.")
52
Learn and adapt from each patient as we go along
I-SPY 2 TRIAL: Learn, Drop, Graduate, and Replace Agents Over Time Paclitaxel+ Trastuzumab Randomize Paclitaxel + Trastuzumab* + New Agent A HER 2 (+) AC Paclitaxel + Trastuzumab* + New Agent B Surgery Learn and adapt from each patient as we go along Paclitaxel + Trastuzumab* + New Agent C Paclitaxel + Trastuzumab* + New Agent F Patient is on Study Paclitaxel MRI Residual Disease (Pathology) Key Randomize Paclitaxel + New Agent C Paclitaxel + New Agent F HER 2 (–) AC Surgery Paclitaxel + New Agent GH Paclitaxel + New Agent D Paclitaxel + New Agent E *Investigational agent may be used in place
 AC. Paclitaxel + Trastuzumab* + New Agent B. Surgery. Learn and adapt from each patient as we go along. Paclitaxel + Trastuzumab* + New Agent C. Paclitaxel + Trastuzumab* + New Agent F. Patient is on Study. Paclitaxel. MRI. Residual. Disease. (Pathology) Key. Randomize. Paclitaxel + New Agent C. Paclitaxel + New Agent F. HER 2. (–) AC. Surgery. Paclitaxel + New Agent GH. Paclitaxel + New Agent D. Paclitaxel + New Agent E. *Investigational agent may be used in place.")
53
I-SPY 2: the first graduate Rugo et al, #S5-02, SABCS, 2013
Primary end point: pCR Graduate regimens have >85% Bayesian predictive probability of success in a 300-pts biomarker-linked neoadjuvant phase III trial Veliparib+carbo met the 85% predictive probability criterion in HR-/HER2- and all HER2- pts % pCR p V+Cb better p of successful phase III All HER vs % 71% HR+/HER vs % % TNBC 52 vs % 92% V/Cb graduated with a TNBC signature and recommended for future trial Biomarker study? (lesson from iniparib)
")
54
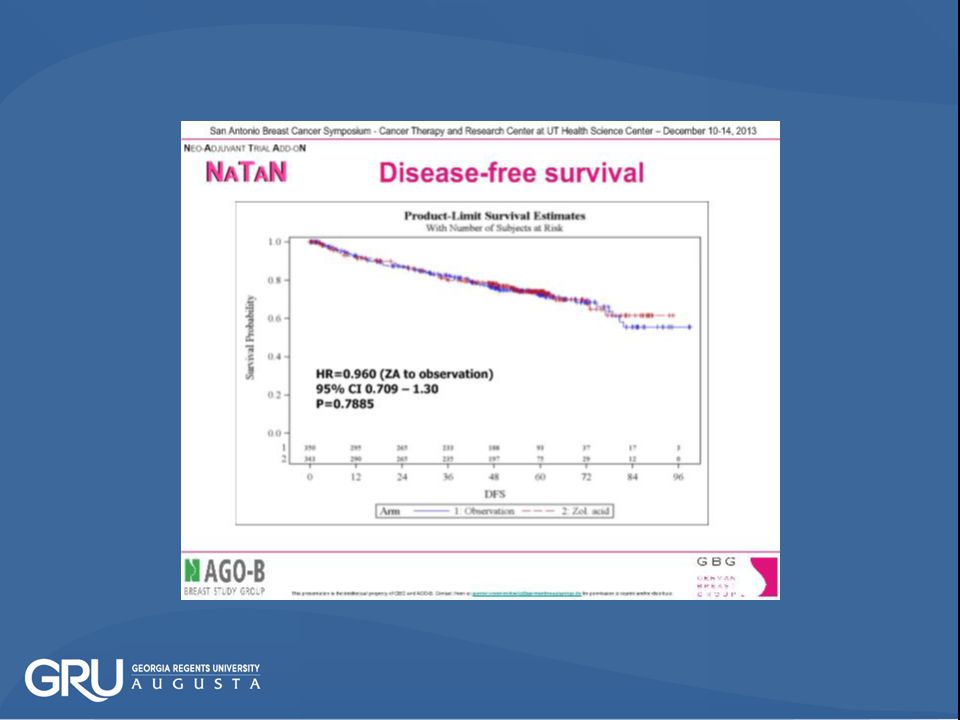
NATAN, post-neoadjuvant zoledronate trial von Minckwitz et al, #S5-05, SABCS 2013
Randomized phase III trial in 693 pts with residual tumor after at least 4 cycles of NAC with taxanes and anthracyclines, median f/u 48 m Z q4wks x6m, q3mx2yrs and q6mx2.5 yrs for 5 yrs vs no Primary end point: EFS at 5 years DFS: HR 0.96 p=0.7885 OS: HR p=0.4082 Decreased BC mortality in post-menopausal pts: RR 0.83 (SE 0.06)
")
59
Metastatic breast cancer

60
Resection of primary BC and ALN in MBC Badwe et al, #S2-02, SABCS 2013
Randomized phase III trial, local regional treatment (LRT) or not, 350 pts, median f/u 17 months, Primary end point: OS Median survival (M): 18.8 vs 20.5, HR=1.07, p=0.60 Overall survival at 2-yr (%): 40.8 vs 43.3 No difference in OS after adjusting age, ER, HER2, site and # of metastasis in Cox regression model (p=1.00) LRT should be reserved for palliative reasons
 or not, 350 pts, median f/u 17 months, Primary end point: OS. Median survival (M): 18.8 vs 20.5, HR=1.07, p=0.60. Overall survival at 2-yr (%): 40.8 vs No difference in OS after adjusting age, ER, HER2, site and # of metastasis in Cox regression model (p=1.00) LRT should be reserved for palliative reasons.")
61
Resection of primary BC in de novo stage IV MBC Soran et al, #S2-03, SABCS 2013
Randomized Turkish trial of LRT vs not, 278 pts, median f/u / m Type of LRT and systemic therapy at the discretions of SO and MO Primary end point: OS OS at 5 m (%): 35 vs 31, p=0.24 OS longer in pts with bone only, HR+, age <50 yr but shorter in TNBC Ongoing US cooperative trial (E2108)
: 35 vs 31, p=0.24. OS longer in pts with bone only, HR+, age <50 yr but shorter in TNBC. Ongoing US cooperative trial (E2108)")
62
ROSE/TRIO-12 trial of ramucirumab in MBC Mackey et al, #S5-04, SABCS 2013
Randomized multicenter phase III trial of ramucirumab (anti-VEGFR2) or placebo in first line HER2- MBC, with biomarker study 1144 pts, 1:2 randomization Primary end point: PFS Median f/u 16.3 m
 or placebo in first line HER2- MBC, with biomarker study pts, 1:2 randomization. Primary end point: PFS. Median f/u 16.3 m.")
67
Targeted therapy

68
Cross-talks among signal transduction pathways

69
Dual function of YAP-1 in caner
Wang and Tang, Can and Met Rev, 2013

70
Letrozole plus dasatinib improves PFS in MBC Paul et al, #S3-07, SABCS 2013
Randomized phase II multicenter USO trial HR+, HER2- MBC first line, 116 evaluable pts Adjuvant AI allowed if completed > 1yr before entry Letrozole +/- dasatinib (Src TKI), cross over allowed Primary end point: CBR (PR/CR/SD>6m) DL L CBR (%) PFS (M) p=0.05 Toxicities: fatigue (38%), nausea (38%), anemia (25%), rash (23%), pleural effusion (16%) and edema (13%) 27% pts required dose reduction for dasatinib Other promising drugs: everolimus, palbociclib, HDACI,PI3KI
, cross over allowed. Primary end point: CBR (PR/CR/SD>6m) DL L. CBR (%) PFS (M) p=0.05. Toxicities: fatigue (38%), nausea (38%), anemia (25%), rash (23%), pleural effusion (16%) and edema (13%) 27% pts required dose reduction for dasatinib. Other promising drugs: everolimus, palbociclib, HDACI,PI3KI.")
71
New Drugs to Overcome Resistance in Hormonal Therapy
Afinitor Product W Product X Product Y Mechanism of Action mTOR inhibitor CDK4/6 kinase inhibitor HDAC inhibitor P13K inhibitor Comparator Exemestane Letrozole Fulvestrant Median PFS Afinitor + Exemestane -7.8 months vs. Exemestane alone -3.2 months (HR = 0.45) Product W + Letrozole months vs. Letrozole alone months (HR = 0.37) Product X + Exemestane -7.1 months vs. Exemestane alone -4.1 months (HR = 0.58) N/A Median OS OS results are not mature Product X + Exemestane months vs. Exemestane alone -22 months (HR = 0.75) Ziaudinn and Tang Review paper in preparation
 Product W + Letrozole months vs. Letrozole alone -7.5 months (HR = 0.37) Product X + Exemestane -7.1 months vs. Exemestane alone -4.1 months (HR = 0.58) N/A. Median OS. OS results are not mature. Product X + Exemestane months vs. Exemestane alone -22 months (HR = 0.75) Ziaudinn and Tang. Review paper in preparation.")
72
Summary Genetic alteration is common in primary and metastatic tumors and in tumors undergoing treatment Identification of biomarkers and drugable mutations by genome sequencing will not only unravel mechanismS of drug resistance but help to offer pts tailored targeted therapy TIL’s are associated with favorable response to breast cancer chemotherapy

73
Summary-2 Biosphophonates reduce tumor relapse in postmenopausal women with EBC, current approval is for their use in bone loss Pts with stage I HER2+ tumors may be offered TH chemotherapy Anti-angiogenesis (bev and ramucirumab) is unlikely effective in unselected pts with BC, biomarker studies are urgently needed
 is unlikely effective in unselected pts with BC, biomarker studies are urgently needed.")
74
Summary-3 Veliparib and/or carboplatin added to taxane backbone increase pCR in TNBC Surgical management of primary tumor in pts with MBC does not improve survival and should only be considered for symptom control and in clinical trials Dasatinib increases the efficacy of letrozole in MBC. Blocking cross talks of ER pathways will help to overcome drug resistance

75
Acknowledgement Industry supporters: Amgen, Genomic Health and Merck
GRU support team: Susan Everitt, Lisa Middleton and Caroline English GRU Cancer Center Leadership and educational grant

76
Thank you

Similar presentations























 on the Efficacy.>")
 Baselga.>")

 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")


 on Aromatase Inhibitor-Associated Bone Loss in Postmenopausal Women with Early Breast Cancer Receiving Adjuvant Letrozole:>")



: investigational agents TTP = median time to disease progression OS = median overall survival.>")
 as part of the adjuvant therapy for all patients with Her2 positive early breast cancer?>")

