Download presentation
Presentation is loading. Please wait.

1
Triple negative breast cancer
19th Annual NOCR meeting Las Vegas, March 15th 2013 Ruth M. O’Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of Hematology and Medical Oncology, Georgia Cancer Center for Excellence, Grady Memorial Hospital

2
Natural history of “triple negative” breast cancers
Basal/TN Sorlie et al PNAS 2003 Copyright ©2003 by the National Academy of Sciences

3
Triple negative breast cancers
High grade aggressive cancers with a high propensity to distant metastases in short-term Poor outcome is multi-factorial but is associated with Chemo-resistance (only about one-third respond to chemotherapy) Lack of molecular targets towards which novel agents can be developed
 Lack of molecular targets towards which novel agents can be developed.")
4
Topics to be covered Triple negative subtyping
Use of pre-operative chemotherapy Activity of chemo-therapeutics in TNBC from pre-operative and metastatic trials Clinical data on potential targets in TNBC Chemo-resistant TNBC

5
BiPar Sciences Iniparib does not improve outcome in unselected metastatic triple negative breast cancer PFS GC (N=258) GCI (N=261) Median PFS, mos (95% CI) 4.1 (3.1, 4.6) 5.1 (4.2, 5.8) HR (95% CI) 0.79 (0.65, 0.98) p-value 0.027 OS GC (N=258) GCI (N=261) Median OS, mos (95% CI) 11.1 (9.2, 12.1) 11.8 (10.6, 12.9) HR (95% CI) 0.88 (0.69, 1.12) p-value 0.28 1.0 1.0 0.9 Pre-specified alpha = 0.01 0.9 Pre-specified alpha = 0.04 0.8 0.8 0.7 0.7 0.6 0.6 Probability of Progression Free Survival 0.5 Probability of Survival 0.5 0.4 0.4 0.3 0.3 0.2 0.2 0.1 0.1 2 4 6 8 10 12 14 16 2 4 6 8 10 12 14 16 Months Since Study Entry Months No. at risk GC 258 171 116 63 38 18 6 1 GCI 261 187 138 83 53 11 2 No. at risk GC 258 239 214 181 151 99 38 11 GCI 261 248 230 204 169 111 52 15 O’Shaughnessy PASCO 2011
 GCI. (N=261) Median PFS, mos (95% CI) 4.1. (3.1, 4.6) 5.1. (4.2, 5.8) HR (95% CI) 0.79 (0.65, 0.98) p-value OS. GC. (N=258) GCI. (N=261) Median OS, mos (95% CI) (9.2, 12.1) (10.6, 12.9) HR (95% CI) 0.88 (0.69, 1.12) p-value Pre-specified alpha = Pre-specified alpha = Probability of Progression Free Survival Probability of Survival Months Since Study Entry. Months. No. at risk. GC GCI No. at risk. GC GCI O’Shaughnessy PASCO")
6
Sub-types of triple negative breast cancer
Evaluated gene expression profiles from 21 breast cancer data sets (14 training and 7 validation = 587 cases of TNBC) Used cluster analysis to sub-divide TNBC into 6 sub-types displaying unique gene expression and ontologies Identified breast cancer cells lines representative of each subtype Lehmann et al JCI 2011
 Used cluster analysis to sub-divide TNBC into 6 sub-types displaying unique gene expression and ontologies. Identified breast cancer cells lines representative of each subtype. Lehmann et al JCI")
7
Click on image to magnify. Basal-like 1: cell cycle, DNA repair and
Basal-like 1: cell cycle, DNA repair and proliferation genes Basal-like 2: Growth factor signaling (EGFR, MET, Wnt, IGF1R) IM: immune cell processes (medullary breast cancer) M: Cell motility and differentiation, EMT processes MSL: similar to M but growth factor signaling, low levels of proliferation genes (metaplastic cancers) LAR: Androgen receptor and downstream genes, luminal features Lehmann et al JCI 2011
 IM: immune cell. processes (medullary. breast cancer) M: Cell motility and differentiation, EMT. processes. MSL: similar to M but. growth factor signaling, low. levels of proliferation genes. (metaplastic cancers) LAR: Androgen receptor. and downstream genes, luminal features. Lehmann et al JCI")
8
Sub-types demonstrate differential response to therapies in vivo
Click on image to magnify. Sub-types demonstrate differential response to therapies in vivo Vehicle Cisplatin Anti-androgen P13K/mTOR inhibitor Lehmann et al JCI 2011

9
Importance of Pathologic CR
Overall Survival Liedtke et al. JCO 2008; 26(8):
:")
10
Among Basal-like Tumors
RCB I (n = 2) RCB 0 (n = 16) RCB II (n = 17) RCB III (n= 9) Log-rank P = 5.5 x 10-7 10
 RCB 0 (n = 16) RCB II (n = 17) RCB III (n= 9) Log-rank P = 5.5 x")
11
Incidence of pCR by Breast Cancer Subtype
107 patients treated with neoadjuvant AC and hormone therapy if HR+. Response Type All Patients N=107 (%) Basal Like N=34 HER2 N=11 Luminal B N=26 Luminal A N=36 CR 14 29 10 8 6 PR 47 56 60 50 33 SD 38 15 30 42 58 PD 1 3 pCR 16 27 36 Carey et al; Clin Cancer Res 2007; 13(8) 11
 Basal Like. N=34. HER2. N=11. Luminal B. N=26. Luminal A. N=36. CR PR SD PD pCR Carey et al; Clin Cancer Res 2007; 13(8) 11.")
12
Neoadjuvant Cisplatin in BRCA1-deficient and Triple Negative Breast Cancer
Patient Population Stage Regimen Pathological Complete Response, n (%) BRCA1 mutation (n = 25) I – III* Cisplatin 75 mg/m2 q3w X4 18 (72%) Triple negative (n = 28) II - III 6 (22%)** (n = 51) Cisplatin 75 mg/m2 q3w X4 + bevacizumab 15 mg/kg q3w X3 8 (16%) (n = 78) Multiple cisplatin - based*** NA (32%) Bottom line: Activity of platinums in TNBC appears similar to other agents but appear particularly active in cancers with mutations of BRCA (and maybe in cancers with other defects in DNA repair) Gronwald et al. J Clin Oncol 2009 Garber et al. Breast Cancer Res Treat 2006 Ryan et al. J Clin Oncol Leone et al. J Clin Oncol 2009
 BRCA1 mutation. (n = 25) I – III* Cisplatin 75 mg/m2 q3w X4. 18 (72%) Triple negative. (n = 28) II - III. 6 (22%)** (n = 51) Cisplatin 75 mg/m2 q3w X4 + bevacizumab 15 mg/kg q3w X3. 8 (16%) (n = 78) Multiple cisplatin - based*** NA (32%) Bottom line: Activity of platinums in TNBC appears similar to other. agents but appear particularly active in cancers with mutations of. BRCA (and maybe in cancers with other defects in DNA repair) Gronwald et al. J Clin Oncol 2009 Garber et al. Breast Cancer Res Treat Ryan et al. J Clin Oncol 2009 Leone et al. J Clin Oncol")
13
GEICAM Phase II Study ARM A pCR =35% ARM B pCR =30%
Epirubicin 90mg/m2 + Cyclophosphamide 600mg/m2 (q 21 days x 4 courses) followed by Docetaxel 100mg/m2 (q 21 days x 4 courses) ARM A Stratification criteria: Tumor size (<1 cm vs. 1-2cm vs. 2-5 cm vs. >5) Tumor grade (I vs. II vs. III) Nodal status (N0 vs. N1/N2). Basal-like by IHC R A N D O M I Z T pCR =35% Epirubicin 90mg/m2 + Cyclophosphamide 600mg/m2 (q 21 days x 4 courses) followed by Docetaxel 75mg/m2 + Carboplatin AUC 6 mg/ml/min (q 21 days x 4 courses) ARM B pCR =30% Alba E, et al. Abstract 74933, ASCO 2011 13
 followed by. Docetaxel 100mg/m2. (q 21 days x 4 courses) ARM A. Stratification criteria: Tumor size (<1 cm vs. 1-2cm vs. 2-5 cm vs. >5) Tumor grade (I vs. II vs. III) Nodal status (N0 vs. N1/N2). Basal-like by IHC. R. A. N. D. O. M. I. Z. T. pCR =35% Epirubicin 90mg/m2 + Cyclophosphamide 600mg/m2 (q 21 days x 4 courses) followed by. Docetaxel 75mg/m2 + Carboplatin AUC 6 mg/ml/min. (q 21 days x 4 courses) ARM B. pCR =30% Alba E, et al. Abstract 74933, ASCO")
16
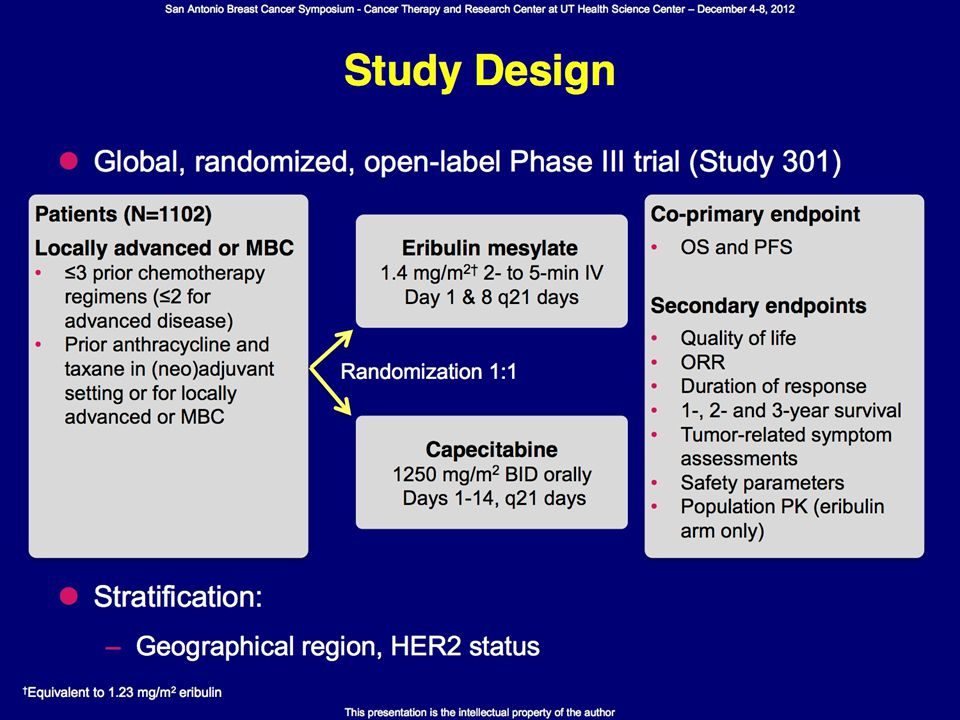
Capecitabine ± Ixabepilone in Triple Negative MBC
Efficacy Ixa + Cape (n = 191) Cape (n = 208) ORR 31% 15% CR 3% 1% PR 28% 14% Median PFS 4.2 mos 1.7 mos HR 0.63 P value < .0001 Median OS 10.3 mos (n = 213) 9.0 mos (n = 230) 0.87 .18 Pooled triple negative subgroup (n = 443) Rugo et al. SABCS 2008, Abstract 3057 16 16
 Cape (n = 208) ORR. 31% 15% CR. 3% 1% PR. 28% 14% Median PFS. 4.2 mos. 1.7 mos. HR P value. < Median OS mos. (n = 213) 9.0 mos. (n = 230) Pooled triple negative subgroup (n = 443) Rugo et al. SABCS 2008, Abstract")
17
BiPar Sciences Iniparib does not improve outcome in unselected metastatic triple negative breast cancer PFS GC (N=258) GCI (N=261) Median PFS, mos (95% CI) 4.1 (3.1, 4.6) 5.1 (4.2, 5.8) HR (95% CI) 0.79 (0.65, 0.98) p-value 0.027 OS GC (N=258) GCI (N=261) Median OS, mos (95% CI) 11.1 (9.2, 12.1) 11.8 (10.6, 12.9) HR (95% CI) 0.88 (0.69, 1.12) p-value 0.28 1.0 1.0 0.9 Pre-specified alpha = 0.01 0.9 Pre-specified alpha = 0.04 0.8 0.8 0.7 0.7 0.6 0.6 Probability of Progression Free Survival 0.5 Probability of Survival 0.5 0.4 0.4 0.3 0.3 0.2 0.2 0.1 0.1 2 4 6 8 10 12 14 16 2 4 6 8 10 12 14 16 Months Since Study Entry Months No. at risk GC 258 171 116 63 38 18 6 1 GCI 261 187 138 83 53 11 2 No. at risk GC 258 239 214 181 151 99 38 11 GCI 261 248 230 204 169 111 52 15 O’Shaughnessy PASCO 2011
 GCI. (N=261) Median PFS, mos (95% CI) 4.1. (3.1, 4.6) 5.1. (4.2, 5.8) HR (95% CI) 0.79 (0.65, 0.98) p-value OS. GC. (N=258) GCI. (N=261) Median OS, mos (95% CI) (9.2, 12.1) (10.6, 12.9) HR (95% CI) 0.88 (0.69, 1.12) p-value Pre-specified alpha = Pre-specified alpha = Probability of Progression Free Survival Probability of Survival Months Since Study Entry. Months. No. at risk. GC GCI No. at risk. GC GCI O’Shaughnessy PASCO")
18
No response in normal BRCA status
PARP Inhibitor Trials – Activity Seen Only in BRCA1/2 Mutation Carriers Agent Author BRCA1/BRCA2 TNBC Response Rate Olaparib (phase I; mixture tumor types) Fong 60 patients 37% -BRCA1/2 mutations N/A 63% clinical benefit rate (only in BRCA associated cancers) Olaparib 400 mg po BID Tutt 27 patients BRCA1 67% BRCA2 33% 50% 41% ABT888 +temozolomide Isakoff 41 patients BRCA1: 7.3% BRCA2: 12% 56% BRCA 1 and 2: 37.5% No response in normal BRCA status 1. Fong PC, et al. N Engl J Med. 2009; 361:123-34; 2. Tutt, et all. Lancet Vol. 376 No pp ; 3. Isakoff et al. J Clin Oncol 28:15s, 2010 (suppl; abstr 1019) ;
 Fong. 60 patients. 37% -BRCA1/2 mutations. N/A. 63% clinical benefit rate. (only in BRCA associated cancers) Olaparib 400 mg po BID. Tutt. 27 patients. BRCA1 67% BRCA2 33% 50% 41% ABT888 +temozolomide. Isakoff. 41 patients. BRCA1: 7.3% BRCA2: 12% 56% BRCA 1 and 2: 37.5% No response in normal BRCA status. 1. Fong PC, et al. N Engl J Med. 2009; 361:123-34; 2. Tutt, et all. Lancet Vol. 376 No pp ; 3. Isakoff et al. J Clin Oncol 28:15s, 2010 (suppl; abstr 1019) ;")
19
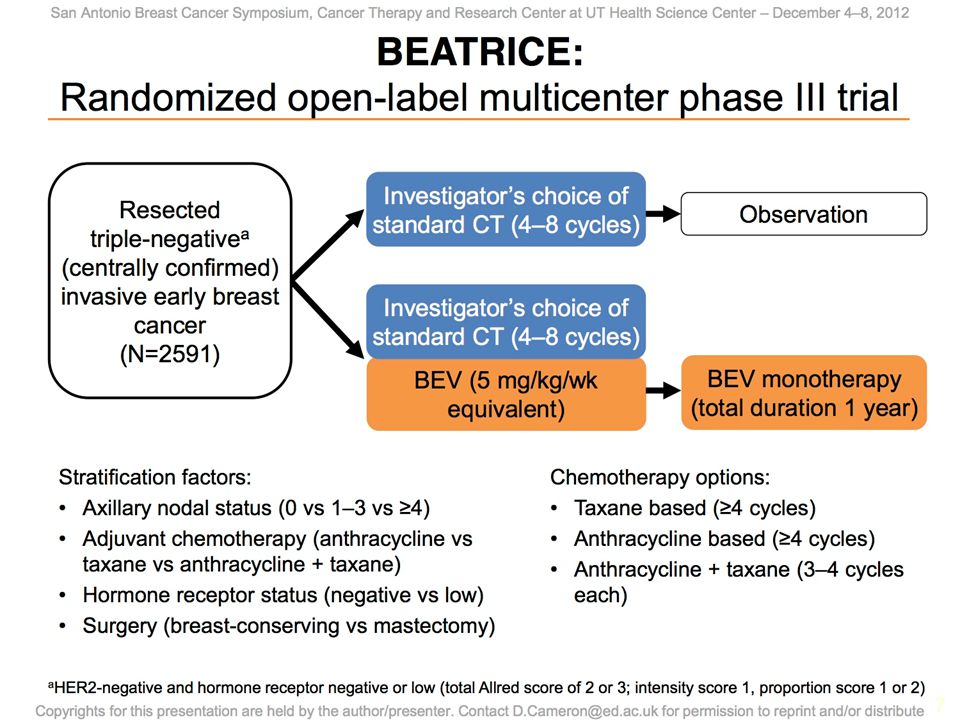
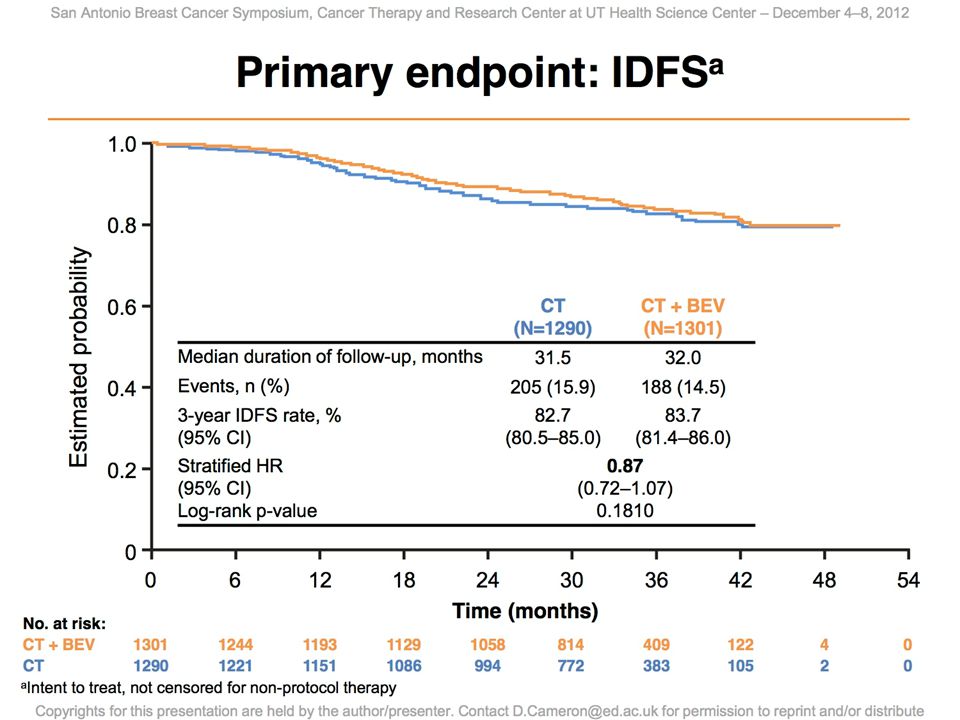
Angiogenic inhibitors in triple negative breast cancer
Addition of bevacizumab to paclitaxel in 1st line triple negative metastatic breast cancer significantly improves DFS (HR 0.47) Addition of bevacizumab to chemotherapy significantly improves DFS in 2nd line triple negative metastatic breast cancer (HR 0.53 versus HR-positive 0.89 (NS)) Miller at al NEJM, Brufsky el al PASCO 2010
 Addition of bevacizumab to chemotherapy significantly improves DFS in 2nd line triple negative metastatic breast cancer (HR 0.53 versus HR-positive 0.89 (NS)) Miller at al NEJM, Brufsky el al PASCO")
23
No adjuvant chemo planned
Neoadjuvant Chemo plus Carboplatin +/- Bevacizumab in Stage II-III TNBC (Phase II CALGB 40603) Paclitaxel 80mg/m2 wkly x4 ddAC x4 Surgery 4-8 wks after last ddAC XRT No adjuvant chemo planned Paclitaxel 80mg/m2 wkly x4 ddAC x4 Bevacizumab 10mg/kg q2w x 9 Paclitaxel 80mg/m2 wkly x4 ddAC x4 Carboplatin AUC 6 q3w x 4 Paclitaxel 80mg/m2 wkly x4 ddAC x4 Bevacizumab 10mg/kg q2w x 9 Carboplatin AUC 6 q3w x 4 Sikov WM, et al. J Clin Oncol. 2010;28:15s (Abstract TPS 110).
 Paclitaxel 80mg/m2 wkly x4. ddAC x4. Surgery. 4-8 wks after last ddAC. XRT. No adjuvant chemo planned. Paclitaxel 80mg/m2 wkly x4. ddAC x4. Bevacizumab 10mg/kg q2w x 9. Paclitaxel 80mg/m2 wkly x4. ddAC x4. Carboplatin AUC 6 q3w x 4. Paclitaxel 80mg/m2 wkly x4. ddAC x4. Bevacizumab 10mg/kg q2w x 9. Carboplatin AUC 6 q3w x 4. Sikov WM, et al. J Clin Oncol. 2010;28:15s (Abstract TPS 110).")
24
Phase II Neoadjuvant Trial of Sorafenib in combination with Cisplatin followed by dose dense Paclitaxel for ER-, PR-, Her2- (Triple Negative) Early-stage Breast Cancer PET Biopsy PET Biopsy Biopsy PET Early Stage Triple Negative BreastCancer Sorafenib 400 mg po bid x 4 weeks Cisplatin 75 mg/m2 q3wk x 4 cycles Paclitaxel 175 mg/m2 q2wk x 4 cycles Surgery Sorafenib 400 mg po bid

25
Is EGFR a viable target for triple negative breast cancer?
EGFR/HER1 K-Ras GRO1 TCF4 Frizzled 7 Laminin gamma 2 c-KIT Keratin 5 Keratin 17 P-Cadherin

26
Randomized Phase II: Cetuximab +/- Carboplatin for Triple-Negative MBC
Cetuximab + Carboplatin at Progression N=22 Cetuximab + Carboplatin N=49 Arm 1 Cetuximab Cetuximab + carboplatin Arm 2 Cetuximab + carboplatin Arm 1b + 2 N 31 24 71 95 ORR CR PR 2 (6%) 4 (17%) 12 (17%) 1 (1%) 11 (15%) 16 (17%) 15 (16%) SD 5 (16%) 6 (25%) 16 (23%) 22 (23%) Carey et al. J Clin Oncol 2012
 4 (17%) 12 (17%) 1 (1%) 11 (15%) 16 (17%) 15 (16%) SD. 5 (16%) 6 (25%) 16 (23%) 22 (23%) Carey et al. J Clin Oncol")
27
EGFR inhibitors in TNBC
PD01-01 Met TNBC ≤ 1 chemo for mets Cisplatin + Cetuximab (n=114) R Cisplatin (n=57) Cis + EGFR Cis p Response (%) 20 10 0.5 PFS (mo) 3.7 1.5 0.032 Baselga et al SABCS 2010
 R. Cisplatin (n=57) Cis + EGFR. Cis. p. Response (%) PFS (mo) Baselga et al SABCS")
28
Phase 2 trial of bicalutamide in AR+ ER- PR- MBC
Screening 452 patients with TNBC: 51 (12%) were AR+ 26 patients were treated with bicalutamide 150mg daily No responses, stable disease > 6-months in 5 patients Median PFS 12-months Gucalp et al Proc ASCO 2012 Abstract 1006
 were AR+ 26 patients were treated with bicalutamide 150mg daily. No responses, stable disease > 6-months in 5 patients. Median PFS 12-months. Gucalp et al Proc ASCO 2012 Abstract")
29
Use of pre-operative approach for prognosis and novel trials
PCR Good prognosis Early stage triple negative breast cancer 25 to 30% Pre-operative chemotherapy SX 70% BX Residual chemo- resistant disease Trials with novel agents/ approaches

32
Pre-operative trial in triple negative breast cancer
PET Biopsy PET Biopsy Biopsy PET PCR Early Stage TNBC (not LABC) SORAFENIB CISPLATIN PACLITAXEL Surgery SORAFENIB Residual cancer Cell surface receptors Stem cell isolation Genomic Analysis Wnt pathway inhibitor (BL2, Mes, Mes-stem subtypes)
 SORAFENIB. CISPLATIN. PACLITAXEL. Surgery. SORAFENIB. Residual cancer. Cell surface receptors. Stem cell isolation. Genomic Analysis. Wnt pathway inhibitor. (BL2, Mes, Mes-stem subtypes)")
33
Targeting growth factors in chemo-resistant TNBC
Mouse “clinical trial” Residual Chemo-resistant TNBC Gene expression (Vanderbilt subtypes) Pre-operative Chemotherapy (Phase 2 clinical trials) TNBC Theranostic Nanoparticles (EGFR/IGF1R) Human TNBC Xenografts
 Pre-operative. Chemotherapy. (Phase 2 clinical trials) TNBC. Theranostic. Nanoparticles. (EGFR/IGF1R) Human TNBC. Xenografts.")
34
Summary TNBC remains a major therapeutic challenge
TNBC is an umbrella term for a heterogeneous group of breast cancer Major issues include chemo-resistance and lack of therapeutic targets Use of pre-operative approach appears optimal

Similar presentations










 on the Efficacy.>")
 Baselga.>")

 –Localised to breast +/- lymph nodes –Recommended standard treatment involves NEPTUNE Taxane.>")




 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")




