Download presentation
Presentation is loading. Please wait.

1
NSAID gastropathy Professor Yaron Niv Rabin Medical Center Tel Aviv University

2
NSAID gastropathy u The problem u Pathogenesis u Role of Helicobacter pylori u Prophylactic therapy u Potentially safer NSAIDs

3
Scope of NSAID Gastropathy (after 3 months therapy) u Dyspepsia 10%-20% u Gastric ulcer in 15%-20%(x5) u Duodenal ulcer in 5%-8% u Risk of severe complication is 2% - 4%/y
 u Dyspepsia 10%-20% u Gastric ulcer in 15%-20%(x5) u Duodenal ulcer in 5%-8% u Risk of severe complication is 2% - 4%/y")
4
Scope of NSAID Gastropathy u In USA NSAIDs are used regularly by 13 millions. u 103,000 develop severe GI complication, 16,500 deaths/y (1:788). u Mortality from GI complications in users x4.21 controls. u $20,000 per hospitalization, $2 b/y.
. u Mortality from GI complications in users x4.21 controls. u $20,000 per hospitalization, $2 b/y..")
6
On the Average in Quebec, for Every Dollar Spent on NSAIDs, Another $0.73 Were Needed for GI Problems $0.94 $1.28 *Gastroprotective agents, *visits to Gastroenterologists, *GI diagnostic tests, *GI hospitalizations Cost of GI-Related Events Cost of NSAID + Dispensing Fee

7
NSAID - ulcer: Clinical Presentation Among asymptomatic patients, bleeding or perforation is frequently the first manifestation of ulcer disease. Explanations: 1. NSAID-induced analgesia 2. NSAID may exacerbate a previously existing “silent” ulcer 3. Anti-platelet action - bleeding

8
NSAIDs Vs. H.pylori Related Ulcer NSAIDs Vs. H.pylori Related Ulcer u Gastric > Duodenal u More often asymptomatic u Surrounding mucosa normal u Duodenal > Gastric u Usually pain or dyspepsia u Surrounding mucosa inflamed

9
NSAID gastropathy u The problem u Pathogenesis u Role of Helicobacter pylori u Prophylactic therapy u Potentially safer NSAIDs

10
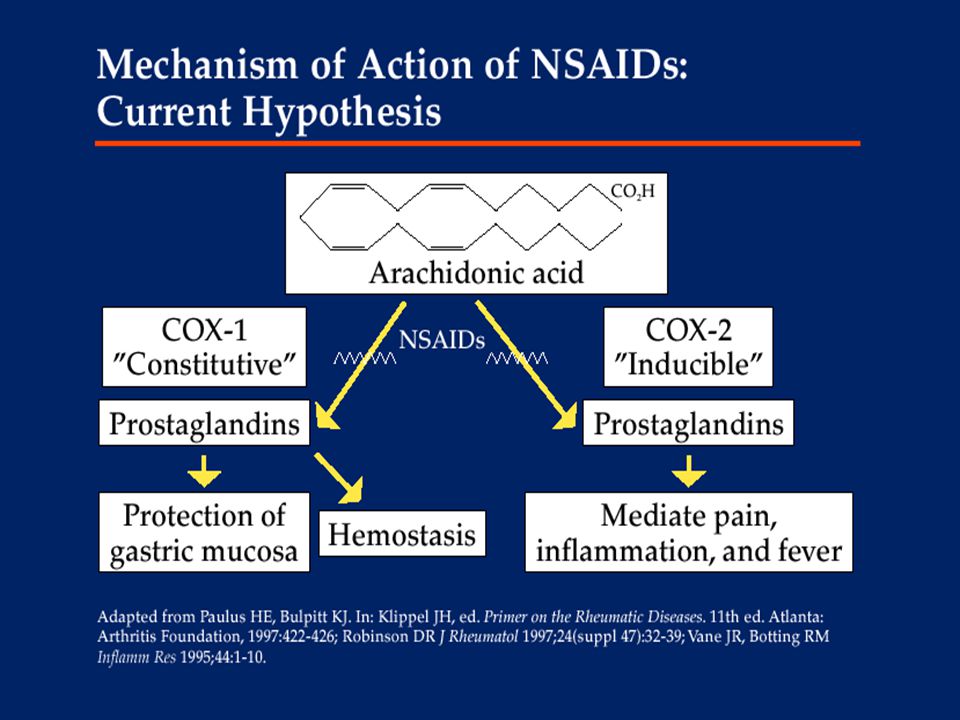
NSAID - Pathogenesis u 1. Prostaglandin (COX) inhibition u 2. Impaired mucosal defense u 3. Leukocyte margination u 4. Topical effect

11
Gastric Mucosal Barrier COX 1 H+ pH<2 H+ MUCUS HCO 3 - pH=7 Mucosal Cells Circulation Surface active phospholipids Epithelial proliferation

12
Effects of Prostaglandins Inhibition Cox 1 inhibition pH<2 H+ MUCUS HCO 3 - Cellular damage Circulation Chronic injury Adhesion molecules Neutrophil adherence Stasis Microvascular ischemia Free radical formation Erosion Scheiman, Clin North Am 96;25:279

13
Mechanisms of NSAIDs Gastroduodenal Injury NSAID Hepatic metabolism Active NSAID metabolite Decrease in gastric mucosal PGs Systemic effect

14
NSAID gastropathy u The problem u Pathogenesis u Role of Helicobacter pylori u Prophylactic therapy u Potentially safer NSAIDs

15
Helicobacter pylori u Antral gastritis - 95% u Duodenal ulcer - 90% u Gastric ulcer - 75% u Gastric adenocarcinoma u Maltoma A possible synergistic relation with NSAID use?

16
NSAID and Helicobacter pylori Before a long course of NSAID or aspirin, eradication (test and treat) of Helicobacter pylori should be considered
 of Helicobacter pylori should be considered")
17
חיסול הליקובקטר לפני טיפול ממושך ב NSAID Chan, Lancet 2002;359:9-13 102 חולי ארטריטיס שע " פ תבחין נשיפה חיוביים להליקובקטר פילורי רנדומיזציה לחיסול החיידק ע " י טפול משולש (OAC) או אומפרזול ופלצבו לאנטיביוטיקה 6 חדשי טיפול בוולטרן 100 מג ' ליום גסטרוסקופיה אחרי 6 חדשים
 או אומפרזול ופלצבו לאנטיביוטיקה 6 חדשי טיפול בוולטרן 100 מג ליום גסטרוסקופיה אחרי 6 חדשים")
18
Hp and NSAID in ulcer disease: a meta-analysis Huang, Lancet 2002;359:14-22 u 25 acceptable studies u Ulcer in NSAID-taker: Hp + 42%, Hp - 26% u NSAID-taker Hp+ x 61 ulcer than non-takers Hp - (either factor alone x 20) u Ulcer bleeding: Hp infection x 1.79, NSAID x 4.85, together x 6.13
 u Ulcer bleeding: Hp infection x 1.79, NSAID x 4.85, together x 6.13")
19
NSAID gastropathy u The problem u Pathogenesis u Role of Helicobacter pylori u Prophylactic therapy u Potentially safer NSAIDs

20
Risk Factors for NSAID Ulcers u Prior NSAID-induced or peptic ulcer u Higher doses or more than one sort u Advanced age (>70 years) u Anticoagulation u Concomitant steroid use u Major illness u Possible: H. pylori, IHD, RA, Ethanol, Smoking

21
For how long? u The greater risk is within the first 3 m of initiation. u The risk of NSAID- associated GI hemorrhage remains constant over an extended period of observation.

22
Options for NSAID Prophylactic Therapy (prevent ulcer and dyspepsia) u PPI (omeprazole 20-40mg 1x1/d) > PGE1, Misoprostol (cytotec 200 g 1x3/d) > H2 receptor antagonist (famotidine 40mg 1x2/d or ranitidine 300 mg 1x2/d). u Misoprostol good for prevention of gastric ulcer but causes diarrhea.

23
Therapy of NSAID-induced dyspepsia, ulcer or erosive gastritis u Stop NSAID u H. pylori status ( 13 C-urea breath test) - eradication. u PPI (if dyspepsia continuous or NSAID has to be continued).
 - eradication. u PPI (if dyspepsia continuous or NSAID has to be continued)..")
24
NSAID gastropathy u The problem u Pathogenesis u Role of Helicobacter pylori u Prophylactic therapy u Potentially safer NSAIDs

26
COX-2 inhibitors Val 523 Arg 120 Iso 523 NSAID NSAID - needs pocket COX-2 Pocket COX-1COX-2 Arachidonic acid Chr 9, 71kDChr 1, 71kD 75% a.a. homology

27
Comparison of Rofecoxib and Ibuprofen Laine, GE 99;117:776 u 742 0steoarthritis PTS. u Base line endoscopy - N. u Randomization: vioxx 25 or 50 mg, ibuprofen 2.4 gr or placebo. u Endoscopy was repeated at 12 weeks.

28
Summary: NSAID Gastropathy u NSAID Gastropathy is a serious problem. u The mechanism of NSAID ulceration is multifactorial. u H. pylori may aggravate NSAID ulcers. u PPI, Misoprostol and H2 antagonists decrease NSAID ulcers. u Prophylactic therapy should be reserved for high risk patients. u COX-2 inhibitor is safer.

Similar presentations


 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")





>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")


>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")


 2004 Elsevier Inc. All rights reserved. Drugs for Peptic Ulcer Disease Chapter 73.>")
>")


 AspirinAspirin is.>")