Download presentation
Presentation is loading. Please wait.

1
Design and Implementation of a Web-Based Patient Portal Linked to an Ambulatory Care Electronic Health Record: Patient Gateway for Diabetes Collaborative Care RICHARD W. GRANT, M.D., M.P.H., JONATHAN S. WALD, M.D., ERIC G. POON, M.D., M.P.H., JEFFREY L. SCHNIPPER, M.D., M.P.H., TEJAL K. GANDHI, M.D., M.P.H., LYNN A. VOLK, M.H.S., and BLACKFORD MIDDLETON, M.D., M.P.H., M.Sc. DIABETES TECHNOLOGY & THERAPEUTICS 2006

2
Outline Introduction Introduction Conceptual framework Conceptual framework Key design elements Key design elements Evaluation & Results Evaluation & Results Comment Comment

3
Introduction Increasing patient's knowledge about risk factor levels and facilitating collaboration between patients and physicians have both been demonstrated to improve clinical outcomes. Increasing patient's knowledge about risk factor levels and facilitating collaboration between patients and physicians have both been demonstrated to improve clinical outcomes. Personal health records (PHRs) represent one innovative means to achieve these goals. Personal health records (PHRs) represent one innovative means to achieve these goals. But, there have been no large-scale studies of interventions that integrate PHRs directly with the electronic medical records(EMRs) used by patients' own primary care physicians (PCPs). But, there have been no large-scale studies of interventions that integrate PHRs directly with the electronic medical records(EMRs) used by patients' own primary care physicians (PCPs).
 represent one innovative means to achieve these goals. Personal health records (PHRs) represent one innovative means to achieve these goals. But, there have been no large-scale studies of interventions that integrate PHRs directly with the electronic medical records(EMRs) used by patients own primary care physicians (PCPs). But, there have been no large-scale studies of interventions that integrate PHRs directly with the electronic medical records(EMRs) used by patients own primary care physicians (PCPs)..")
4
We hypothesized that enabled patients to both read (eg, laboratory results )and write (eg, medication list) to the EMR was crucial to achieve measurable changes in DM control. We hypothesized that enabled patients to both read (eg, laboratory results )and write (eg, medication list) to the EMR was crucial to achieve measurable changes in DM control. Using the DM-specific PHR would result in improved care by increasing patient knowledge and engagement in their own care and by facilitating patient-physician communication. Using the DM-specific PHR would result in improved care by increasing patient knowledge and engagement in their own care and by facilitating patient-physician communication.
and write (eg, medication list) to the EMR was crucial to achieve measurable changes in DM control. Using the DM-specific PHR would result in improved care by increasing patient knowledge and engagement in their own care and by facilitating patient-physician communication. Using the DM-specific PHR would result in improved care by increasing patient knowledge and engagement in their own care and by facilitating patient-physician communication..")
5
Conceptual framework The key barriers to Diabetes Care: The key barriers to Diabetes Care: lack of patient engagement with therapeutic care plans. lack of patient engagement with therapeutic care plans. lack of medication adjustment by physicians during clinical encounters. lack of medication adjustment by physicians during clinical encounters. If properly prepared and engaged in care patients themselves may be effective catalysts for changing clinical care processes. If properly prepared and engaged in care patients themselves may be effective catalysts for changing clinical care processes. A patient web-portal designed to encourage patients with discuss corresponding medication initiation or dose adjustment would help reduce clinical inertia. A patient web-portal designed to encourage patients with discuss corresponding medication initiation or dose adjustment would help reduce clinical inertia.

6
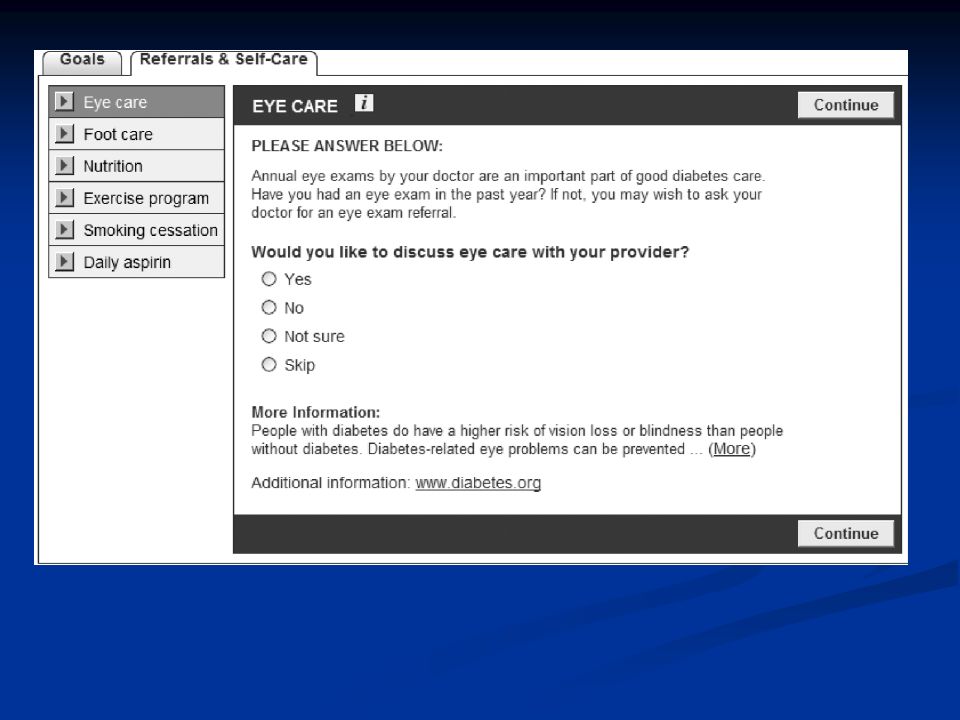
The patient s view The key goals of the design for the patient interface were The key goals of the design for the patient interface were to organize the clinical data in an educational format. to organize the clinical data in an educational format. to enable patients to author a detailed, tailored Diabetes Care Plan to share with their PCP. to enable patients to author a detailed, tailored Diabetes Care Plan to share with their PCP. Key design elements

8
Medication Module to allow patients to view their EHR medication list( ). Medication Module to allow patients to view their EHR medication list( ). Diabetes-specific medication library used to treat each of three conditions. Diabetes-specific medication library used to treat each of three conditions.
. Diabetes-specific medication library used to treat each of three conditions. Diabetes-specific medication library used to treat each of three conditions..")
9
Increase the detection and handling of discrepancies and adverse drug events (ADEs). Increase the detection and handling of discrepancies and adverse drug events (ADEs).
..")
11
The physician s view The system was designed with the following workflow The system was designed with the following workflow Only one diabetes module at a time can be open per patient. Only one diabetes module at a time can be open per patient. A Diabetes Care Plan can only be submitted if the visit still appears in the scheduling system. A Diabetes Care Plan can only be submitted if the visit still appears in the scheduling system. Once submitted, a Diabetes Care Plan link appears near the patient's name on the provider schedule. Once submitted, a Diabetes Care Plan link appears near the patient's name on the provider schedule. Patient submissions auto close after 21 days of inactivity. Patient submissions auto close after 21 days of inactivity. Avoiding physicians receive multiple care plans from a single patient, or care plans submitted without an appointment. Avoiding physicians receive multiple care plans from a single patient, or care plans submitted without an appointment.

12
Clinical Data Repository

13
Evaluation & Results This study was conducted in 11 primary care practices within the Partners HealthCare system (Boston, MA). This study was conducted in 11 primary care practices within the Partners HealthCare system (Boston, MA). Patients were unaware of their PHR assignment (intervention, control) when consenting to enroll in the study. Patients were unaware of their PHR assignment (intervention, control) when consenting to enroll in the study. Control practices who were invited to use an online family history and health maintenance PHR (non–DM-specific PHR) Control practices who were invited to use an online family history and health maintenance PHR (non–DM-specific PHR) The primary distinction between the 2 study arms was the content of the PHR modules. The primary distinction between the 2 study arms was the content of the PHR modules.
. Patients were unaware of their PHR assignment (intervention, control) when consenting to enroll in the study. Patients were unaware of their PHR assignment (intervention, control) when consenting to enroll in the study. Control practices who were invited to use an online family history and health maintenance PHR (non–DM-specific PHR) Control practices who were invited to use an online family history and health maintenance PHR (non–DM-specific PHR) The primary distinction between the 2 study arms was the content of the PHR modules. The primary distinction between the 2 study arms was the content of the PHR modules..")
15
No significant differences between intervention and control. No significant differences between intervention and control.

16
Patients who submitted DM PHR Care Plans were more likely to have a medication initiation or dosage adjustment. Patients who submitted DM PHR Care Plans were more likely to have a medication initiation or dosage adjustment.

17
There were too few patients for meaningful comparisons by risk factor within the on treatment subset. There were too few patients for meaningful comparisons by risk factor within the on treatment subset. Patients with medication changes had clinically and statistically significant subsequent decreases in HbA 1c level and LDL-C level. Patients with medication changes had clinically and statistically significant subsequent decreases in HbA 1c level and LDL-C level.

18
Comment Users of the DM-specific PHR were markedly more likely to have their medical regimens changed at their next clinic visit. Users of the DM-specific PHR were markedly more likely to have their medical regimens changed at their next clinic visit. Specific patient portals linked directly to physicians EMRs can have an important impact on reducing clinical inertia. Specific patient portals linked directly to physicians EMRs can have an important impact on reducing clinical inertia. The lack of an impact on DM-related risk factor levels The lack of an impact on DM-related risk factor levels Only a small proportion of potentially eligible patients signed up for access to the Web portal. Only a small proportion of potentially eligible patients signed up for access to the Web portal. Patients with poor metabolic control were less likely to enroll in the Prepare for Care study. Patients with poor metabolic control were less likely to enroll in the Prepare for Care study.

19
Study population consist of younger and more affluent patients and thus may not be immediately generalizable to other patient groups. Study population consist of younger and more affluent patients and thus may not be immediately generalizable to other patient groups. limitations of the study limitations of the study Did not seek to significantly change the ways in which PCPs currently practiced. Did not seek to significantly change the ways in which PCPs currently practiced. Did not collect patient measures such as DM knowledge, level of engagement in care, or confidence with patient- physician communication. Did not collect patient measures such as DM knowledge, level of engagement in care, or confidence with patient- physician communication.

20
Thanks for your attention.

Similar presentations




>")



>")






 System to California’s Foster Care Population.>")





